INTRODUCTION
Treatment of acute Achilles tendon (AT) ruptures (ATR) has long remained controversial. Historically, operative management (OM) was thought to provide a reduced risk of re-rupture albeit with the possibility of postoperative complications.1,2 More recently, studies using non-operative management (NOM) with accelerated rehabilitation by early mobilization have demonstrated comparable results to OM.3–8 Despite these advancements, strength and functional deficits are common following ATR.9–17
AT elongation and calf muscle atrophy have been proposed as causative factors for strength deficits following an ATR, yet the literature is ambiguous. AT elongation has been associated with calf muscle atrophy,9 decreased plantar flexion strength,9 heel-rise test deficits (height, repetitions, work)18 and altered ankle kinetics and kinematics during walking, jogging and running.19 This was further examined with a randomized trial comparing OM to NOM with identical rehabilitation.10 At 18 months, AT length was increased in NOM, and OM patients had 10% to 18% greater plantar flexor strength. Carmont et al11 concluded that tightness of the tendon repair during surgery was the most important modifiable risk factor for tendon elongation and heel-rise deficits. However, others have found that AT elongation does not influence plantar flexion strength, patient’s subjective interpretation of recovery,12 nor does it relate to muscle volume and calf muscle circumference.13 Methodological variation across studies may partially explain the varied findings, as strength deficits may be larger in greater degrees of plantar flexion relative to analysis of peak torque.
Evaluations of functional performance have focused on muscular strength,9–13 with minimal research investigating the relationship between AT length and dynamic performance (i.e. jumping and hopping).14,15 Brorsson et al19 found that individuals with heel rise deficits greater than 30% had increased AT length and the limb symmetry index (LSI) of heel-rise test work correlated with kinetic variables during hopping. Nicholson et al14 found that although there were no differences in peak isokinetic plantar flexion strength between limbs, there was significant reductions in single-leg countermovement jump (CMJ) height. They also showed longer bilateral drop vertical jump contact time for the injured side without differences in landing forces.14 This suggests that dynamic performance cannot be assumed to be recovered by strength measures alone.
Further research is required to understand the relationship between tendon morphological changes following ATR, isolated muscular strength, and dynamic performance measures. The purpose of this study was to determine if functional performance including strength, jumping, and hopping outcomes differed between OM and NOM of acute ATR. The secondary objective was to assess the degree of association between AT morphology and performance outcomes. It was hypothesized that in patients following NOM of ATR, AT length would be greater, and performance would be reduced (including muscular strength, hopping, and jumping) relative to OM.
MATERIALS AND METHODS
Participants
This was a retrospective cohort study with a single prospective evaluation. Eligible participants were between 18 - 65 years old, that had undergone treatment for an acute complete ATR between October 2014 and October 2019 at a regional orthopedic clinic, and were treated within three weeks of the injury. Informed consent was obtained prior to participating in the study. Patients were excluded if they had a re-rupture of their AT, ATR on their contralateral leg, surgical site infection, or any significant ankle, knee, or medical comorbidities that prevented functional testing. Ethics approval was obtained by the University of Manitoba Research Ethics Board prior to commencing the study.
Surgical Technique and Non-Operative Management
All surgeries were performed in an open manner during which each end of the tendon was debrided of abnormal tissue and repaired in a side to side fashion with No. 2 Fiberwire sutures (Arthrex, Naples Fl). A backslab (below knee half cast) was placed on the ankle in plantarflexion and converted to a boot with elevated heel wedges at the two-week mark. The management of those who were treated non-operatively differed based on clinician. However, these patients were all managed by some variation of initial non-weight bearing in plantar flexion alongside progressively reduced heel lifts and gradual restoration of weight-bearing, with referral for physical therapy.
Gastrocnemius and Achilles Tendon Morphology
Calf circumference was recorded with participants in a seated position with the knees flexed to 90° over the edge of the examination table. Measurements were recorded at 15 cm distal to the medial knee joint line (identified via palpation),16 and at the point of maximal circumference. Tendon and muscle morphology was determined via B-Mode ultrasound (GE Healthcare LOGIQ, Chicago, IL, USA, 12mHz, linear transducer). Thickness of the lateral and medial gastrocnemius was recorded at 30% of the distance from the respective articular cleft to the malleolus.17 Patients were positioned prone with knees flexed 10° with the feet resting off the examination table for morphological assessment.20 Tendon thickness was recorded at the height of the medial malleolus.20 Tendon length was determined by identifying and marking the proximal (musculotendinous union of the medial gastrocnemius) and distal landmarks (calcaneal insertion) with B-mode ultrasound.20 Landmarks were projected onto the skin by placing a modified (blunted) 18-gauge needle between the ultrasound probe and the skin, which allowed for translation of the anatomical landmark on the ultrasound image to a superficial location on the skin at the position of the needle. The location of the non-inserted needle was then marked on the skin with ink to allow for distance measurement. AT length was normalized relative to estimated tibial length (tibial length = AT length / 0.6 + 53).21
Range of Motion and Achilles Tendon Resting Angle
Ankle range of motion (ROM; active plantar- and dorsiflexion) was recorded via goniometer with participants positioned supine in 30° of knee flexion. AT resting angle was measured in prone with the knee passively flexed to 90° with a goniometer.16,22–25
Patient-Reported Outcome Measures
Patients completed a demographic form and patient-reported outcome measures (PROMS) including the Achilles Tendon Total Rupture Score (ATRS), a Physical Activity Scale (PAS) and the Foot and Ankle Outcome Score (FAOS) Sports and Recreation subscale. The ATRS had patients rank their level of limitation due to symptoms and during certain activities, with each question scored ranging from 0-10 on a Likert scale, with established validity and reliability in patients following ATR and an MCID of 8 points.26,27 The PAS had patients rank their current level of physical activity from “0”, representing “hardly any physical activity”, to “6”, including hard or very hard exercise regularly several times a week (i.e. jogging, skiing). The FAOS assessed patients’ difficulty doing a series of movements over the past week due to their foot or ankle, ranking patients’ difficulty on a 5-point scale ranging from “None”, to “Extreme”.
Performance Assessment
All patients completed a standardized warm up of five minutes on a stationary bicycle, at a self-selected pace, followed by two sets of 10 bilateral heel raises.
Jumping Tests
Participants then completed the jumping tests, which were recorded using dual force plates (1000 hz; AMTI, Watertown, MA, USA). Jump heights were estimated from flight time (height = ½g(t/2)2; g = 9.81 m*sec−2, t = time in air). Participants completed two or three familiarization attempts, before three trials of each jump. For the bilateral countermovement jump (CMJ), participants stood upright with hands placed on their hips, and on cue bent their knees to a depth of their preference and performed a maximal effort jump. For the bilateral squat jump, the method was the same as the bilateral CMJ, however participants would pause for three seconds in the squat position (maximum 90o knee flexion) before completing a maximal effort vertical jump. Unilateral CMJs used the same methodology as the bilateral CMJs, except participants would take off on a single limb, and land on the same limb. Drop vertical jumps (DVJ) were completed with participants starting on a 30 cm elevated platform with the force plates positioned at a distance of half of the participants height from the platform. Participants jumped down from the platform to the force plates, followed by a maximal effort jump for height in a fluid motion. For the single leg DVJ (SL-DVJ) the force plates were positioned at a distance of 25% of the participant’s height from the 30 cm box. Participants would jump down from the box to the plates on a single limb, then complete a maximal single leg jump in one fluid motion, landing on the same single leg to complete the test.
Hop Testing
Four different hop tests were completed on each leg. Each test began with a practice attempt followed by two trials on each limb, alternating between unaffected and affected limbs. The single hop had participants perform a single hop forward for maximal distance. The triple hop consisted of three consecutive hops to achieve maximal distance. The crossover hop had participants complete three consecutive hops for distance, crossing over a 15 cm wide longitudinal marker with each hop. Distances were recorded from the front of patient’s foot on takeoff to the heel on landing. The 6-meter timed hop test had participants hop on one foot for six meters as quickly as possible (Brower Timing Systems TCi System, Draper, UT, USA).
Strength Testing
Isokinetic plantar- and dorsiflexion torque were measured at 60 o/s and 120 o/s (Biodex System 4, Mirion Technologies, Atlanta, GA, USA). Participants were seated with the knee flexed to 10°, the waist and knee immobilized via belts, and foot strapped to the plate attached to dynamometer. Participants were able to practice at each speed before completing five repetitions of maximal effort plantarflexion and dorsiflexion, followed by a 60 second break between trials. Peak torque, and angle-specific torque at 20o of plantarflexion were extracted for analysis.
Statistical Analysis
Two-way analysis of variance (ANOVA; Group: Operative, Non-operative; Side: Affected, Unaffected) were completed for all tests with unilateral values. Independent t-tests were used for between-group comparisons for bilateral outcomes (countermovement jump). Linear regressions were completed for normalized AT length against performance outcomes of the affected limb in absolute measures (i.e. distance, torque) and as a limb symmetry index (LSI) for peak and angle-specific torque and the single leg hop test. Statistical significance was considered at p < 0.05, and all values are presented as means ± standard deviation unless stated otherwise.
RESULTS
Participants
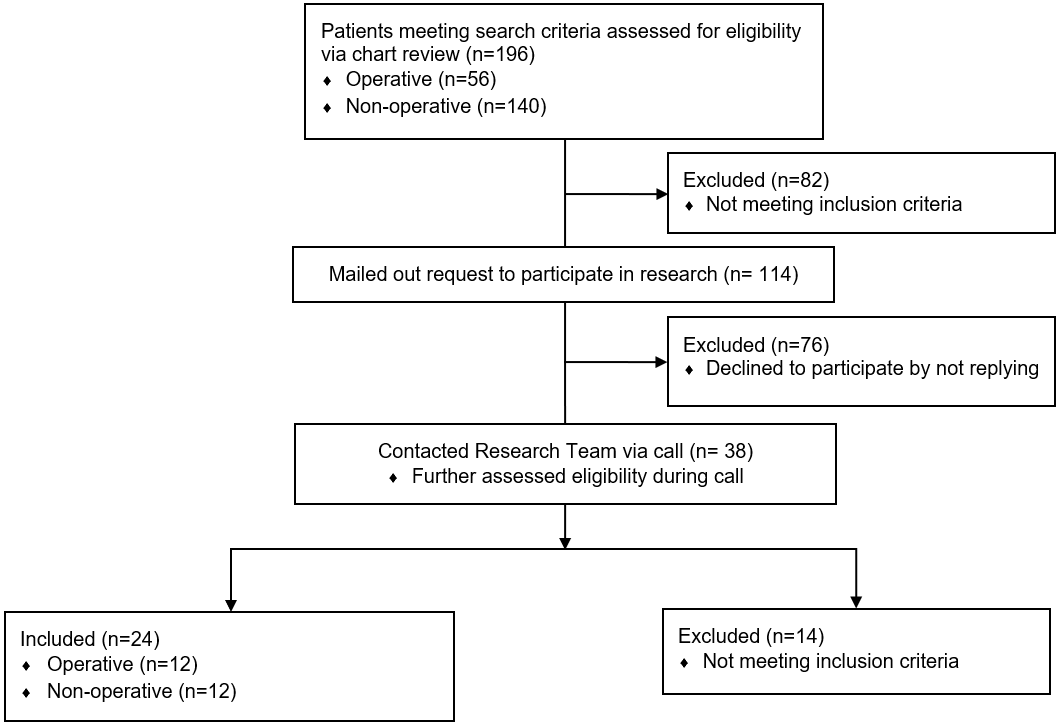
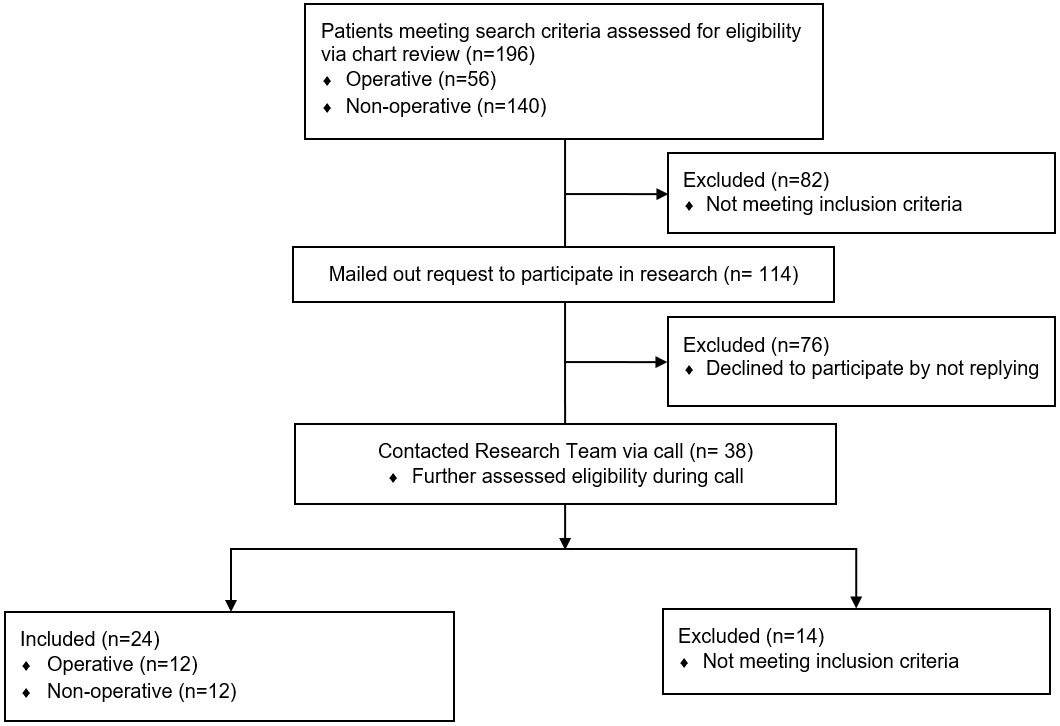
Records (n = 196) were screened against eligibility criteria and a resultant 114 patients were contacted by mail to indicate their potential eligibility to participate in the study. Thirty-eight patients contacted the research center, with 24 ultimately eligible to participate in the study and completing testing, a total of 12 per group (Figure 1). There were no significant differences in demographic data between groups (Table 1). Amongst PROMs only PAS differed for which the NOM group was more active.
Range of motion and Achilles Tendon Resting Angle
Active ROM for dorsiflexion and plantar flexion was not statistically different between limbs or groups (Table 2). AT resting angle was lower on the affected limb (p <0.001) with no effect of group or interaction or group and side (Table 2).
Muscle and Tendon Morphology
There was no effect of side, group, or interaction of group and side on calf girth. Both medial (p = 0.002) and lateral (p = 0.008) gastrocnemius thickness were reduced on the affected side regardless of group. AT thickness was greater on the affected side (F(1,44) = 176.18, p <0.001), with no effect of group or interaction. AT length was greater on the affected limb (p = 0.009) with no effect of group or interaction (Table 2).
Muscular Strength
Isokinetic peak plantar flexor torque at 60o/s and 120o/s was similar between groups and sides, with no interaction of group and side (Table 3). Torque at 20o plantar flexion was reduced on the affected limb when measured at 120o/s (F(1,42) = 5.201, p = 0.028), and while reduced at 60o/s this was not statistically significant (F(1,40) = 3.732, p = 0.06; Table 3). There was no effect of group, or interaction of group and side for angle-specific torque at 20o plantar flexion.
Hop and Jump Performance
Performance was not statistically significantly different between limbs for all single leg hop and single leg jump tests (Table 4). The only significant difference was greater single leg drop vertical jump height in the operative relative to non-operative group (F(1,36) = 6.541, p = 0 .015; Table 4), with no effect of side or interaction. Bilateral jump tests were also not significantly different between groups (Table 5).
Relationship between Achilles Tendon Length and Performance
Regression analyses identified minimal to no association between AT length and single leg hop distance across both the affected and unaffected limbs (Table 6). Only torque at 20o plantar flexion when measured at 120o/s was found to have a significant association with AT length, with AT length explaining 11% of the variance (p = 0.03, Table 6), and peak torque at 120o/s approached significance (8.4%, p = 0.05, Table 6). No significant associations were identified between affected limb AT length and LSI values for the single leg hop or strength outcomes, while the LSI of Peak Torque at 120o/s approached statistical significance (15.6%, p = 0.06; Table 6).
DISCUSSION
This study found persistent gastrocnemius atrophy alongside tendon elongation and thickening regardless of operative or non-operative management of ATR. Impairment in plantar flexor strength was found when measured at 20o plantar flexion at 120o/s, but not when considering peak torque or at slower testing velocities. Despite this reduction, performance on dynamic jumping and hopping tests were comparable between limbs and treatment groups, apart from higher SL-DVJ heights in the operatively managed group. AT length had no association with single leg hop distance or LSI, whereas a minor association was found with overall AT length and plantar flexor torque at 20o plantar flexion at 120o/s.
The relationship between AT length and plantar flexion strength is inconsistent in the literature.9,10,12,13 Similar to some studies, this study found impaired isokinetic plantar flexor strength when measured at greater degrees (20o) of plantar flexion.9,28,29 Both Pajala et al30 and Heikkinen et al9 demonstrated positive correlations between work or peak torque deficits and tendon elongation following ATR, suggesting impaired force production with tendon elongation. Conversely, others have found no relationship between isokinetic work or peak torque and AT length following ATR.28,29,31 The overall lack of agreement regarding strength measurement techniques, including the mode of contraction (isokinetic versus isometric), the metric used to quantify (peak torque versus work), the angle of determination (peak torque versus angle-specific torque), may partially explain the discrepant findings. The development of standardized testing protocols, with test velocities of 120-180o/s with angle-specific measurement of plantar flexor torque at 20-30o plantar flexion, may provide further clarification on the relationship of AT length to plantar flexor strength.
Altered movement patterns and kinetics in walking, jogging and CMJs have been observed following ATR12; however, altered kinematics and kinetics do not necessarily translate into reduced performance outcomes. These results indicate that performance in unilateral hopping and bilateral jumping was comparable between both limbs and groups, apart from the single-leg DVJ which was greater in operative patients, despite significant AT elongation in both groups. Deficits in functional tasks are variable in the literature, of which the evaluation of differing post-operative time points and functional tests are confounding factors. Deficits in SL-DVJ performance have been previously described, upwards of six years post-operative,32,33 while others have found no difference in SL-CMJ and vertical hopping height.15,34 Kinetic compensations during jumping or hopping indicate reduced use on the ankle, with reduced concentric and eccentric plantar flexor power,19,33 and increased eccentric33 or concentric knee power.34 Comparable SL-DVJ between operative and non-operative management has been found, whereas the present study found increased jump height in the operative group, that did not extend across other hop or jump tests. Brorsson et al35 found impaired single leg hop for distance, in contrast to the present results; however, the average LSI values approached 95%, indicating minimal difference between limbs despite statistically significant differences as well as no difference between operative and non-operative groups.
Unique to the present study is the observation that AT length did not have an association with single leg hop performance. Few studies have evaluated the direct relationship between AT length and dynamic performance. Brorsson et al19 identified that patients with >30% heel-rise deficit had reduced ankle concentric and eccentric plantar flexor power during drop jumps and vertical hopping, alongside reduced peak Achilles tendon force and impulse. However, AT length did not correlate with any kinetic differences between the groups. It is possible that there is a threshold whereby AT length impacts dynamic performance, as while others have demonstrated altered walking kinematics,12 Kastoft et al36 recently found near symmetrical between-limb walking kinematics up to 4.5 years after non-operative management, except for a slight delay in heel lift-off, despite upwards of 1.7 cm AT elongation. Conversely, the previously discussed knee-dominant kinetic strategies may be sufficient to maintain hopping and jumping performance, such that no relationship with AT length would be expected on performance outcomes alone. Functional task selection may be important when considering altered kinetic strategies, as ankle, hip and knee contributions vary between vertical or horizontal hops.37 In this case, contribution of the ankle is greatest in the concentric (take-off) phase of horizontal hopping, which suggests future kinetic and kinematic investigations should focus on horizontal hopping, whereas current studies have evaluated primarily vertical hopping and jumping.19,33,34
There were some limitations within this study that should be considered when examining these results. One limitation was the small sample size amongst the potentially eligible screened population. Secondly, due to recruitment being voluntary, bias may exist as the individuals who responded and underwent an assessment may not be entirely representative of the population of individuals with ATRs. Achilles rehabilitation is not standardized across surgeons and sports medicine physicians at this center which introduces variability in participants’ recovery processes and limits the ability to isolate differences between management groups.
CONCLUSION
Participants’ musculotendinous morphology, strength, and functional performance did not differ between operative and non-operative management of acute ATR. Despite persistent gastrocnemius atrophy, plantarflexion weakness and tendon elongation, lower extremity dynamic performance measures were maintained. While no relationship was found between AT length and single leg hop performance, AT length did partially explain isokinetic plantar flexor strength when measured at 20o plantar flexion at higher speeds (120o/s).
Conflicts of Interest
The authors report no conflicts of interest.