Introduction
Lateral ankle sprain (LAS) is a common musculoskeletal injury among active individuals, with incidence rates reported at 7.2 per 1000 person-years, making this one of the most common reasons for accessing healthcare.1–7 Despite the high occurrence, a majority of individuals report not seeking medical care following an ankle sprain, with acute foot and ankle injuries resulting in more work limitations than any other body region.8,9 The strongest risk factor for a future ankle or foot injury (AFI) is a history of an AFI in the previous two years, with 47-70% of those injured sustaining a second LAS within one year.4,10 The high incidence and re-injury rate of LASs result in long term healthcare cost, delayed return to normal recreational and work related activities as well as the development of chronic ankle instability (CAI) in at least 40% of individuals who sustain a LAS.7,11–14
The long-term effects of acute ankle sprains and CAI can be substantial. Approximately 78% of people with CAI develop post-traumatic osteoarthritis (PTOA).15 Patients with ankle PTOA are an average of 14 years younger at time of diagnosis compared to those of other joints, resulting in increased duration of pain, loss of function, and associated economic burdens to society.16 Because the journey to this chronic condition begins at initial injury, the identification and application of appropriate management techniques aimed at the prevention of reinjury and disease progression is essential.
Standard methods of assessing ankle sprains, such as palpation and orthopaedic tests and measures provide only dichotomous information to describe an ankle sprain into either injured or uninjured.17–20 For ankle sprains, a clinical examination alone is unable to provide the comprehensive knowledge of individual injury characteristics to guide treatment decisions and predict long term prognosis.17,18,21,22 Current clinical practice heavily relies on the ability of the clinical exam to accurately evaluate ligamentous damage and to characterize the associated functional impairments. This practice approach is unable to describe the extent and degree of injury in a manner to guide management and predict long-term disability from an acute injury.23,24 Ankle sprains are diagnostically challenging due to variability in presentation with respect to the amount of pain, edema, range of motion loss and functional limitation.
Ultrasound (US) imaging can identify the severity of ligamentous injury in acute ankle sprains to grade and provide prognostic factors for long term outcomes.21 Previous studies have found that US has high sensitivity, specificity and accuracy of 95% or greater when used for the diagnosis of ligamentous injuries and fractures of the foot when compared to magnetic resonance imaging.25–27 Additionally, excellent inter-observer agreement has been observed between expert and novice trained sonographers performing POCUS for ankle sprains.27 Utilization of point of care ultrasound (POCUS) allows for real time, dynamic evaluation of neuromusculoskeletal structures to include joints, ligaments, tendons, muscles and nerves.25 POCUS provides an opportunity to determine the severity of ligamentous injury in LASs to facilitate early and accurate diagnosis and guide management descisions.21,25–29 The purpose of this study was to describe and observe the outcomes associated with POCUS guided early management of acute and sub-acute lateral ankle sprains.
Methods
A prospective case series of individuals presenting with a recent lateral ankle sprain was conducted. This study was approved by the Institutional Review Board at Brooke Army Medical Center, Fort Sam Houston, TX. All participants provided informed consent prior to enrollment in this study.
Participants
A convenience sample of 14 individuals with an inversion ankle sprain within 28 days of injury were recruited from the local emergency department, primary care clinics or direct access physical therapy clinics at Brooke Army Medical Center. Inclusion criteria required participants to be between 18 and 45 years of age, negative Ottawa Ankle rules30 or negative radiographs of the foot and ankle, and sufficient English language skills to complete self-reported outcome measures. Participants were excluded if their clinical examination was consistent with a tibiofibular syndesmosis sprain, a fracture of the foot or ankle was identified, the existence of any condition that prevented the wearing of an ankle brace, or they were unable to commit to the course of care.
POCUS and Clinical Examination
A standardized clinical evaluation, including ultrasound examination was performed to classify participants with a lateral ankle sprain into one of four graded categories. The clinical exam included palpation of injured and potentially injured structures, assessment of swelling, physiologic active and passive range of motion, passive accessory motion, soft tissue mobility, gait, balance, and strength. Range of motion assessment consisted of ankle dorsiflexion and plantarflexion using a goniometer as well as the Ankle Lunge Test (ALT) as a measure of weight bearing dorsiflexion.31 Ankle girth was used to quantitate soft tissue edema, using a standard figure-of-eight measurement as previously described by Devoogdt et al.32–34
A standard and focused POCUS examination of the ankle was then performed using a LogiQ e (GE Healthcare, Milwaukee, WI) with a 4-12 MHz or 8-18 MHz linear transducer by a physical therapists trained to perform musculoskeletal (MSK) ultrasound examinations of the foot and ankle region. All scans were reviewed by a physical therapist Registered in Musculoskeletal sonography with over ten years of experience performing MSK ultrasound examinations. Guidelines of the Ultrasound Subcommittee of the European Society of Musculoskeletal Radiology (ESSR) were utilized to establish the scanning protocol and included examination of the joints, tendons, ligaments, bone surfaces and visible articular surfaces of the ankle.35 The examiner classified each structure as either stretched with minimal tearing, partially torn or completely torn to establish a grade of ligamentous injury.36 During the ultrasound exam all areas of pain were assessed but the extent of ligamentous injury along with range of motion loss and joint edema were used to assign a grade of injury. Clinical and ultrasound findings were integrated to determine the extent of ligamentous protection strategies such as movement and weight bearing restrictions along with bracing techniques to maximize early protection of injured structures. Injury grading and bracing strategies are detailed in Table 1. During a two-week follow-up, participants received a second ultrasound examination to confirm the injury severity and describe any progression of pathology, such as joint effusion or inflammatory changes.
Rehabilitation
Initial treatment focused on protecting injured ligamentous structures, reducing edema and pain free active dorsiflexion and plantarflexion range of motion. Assistive devices were utilized as needed to normalize gait. Treatment also included adherence to bracing strategies listed in Table 1, and the avoidance of active ankle inversion for six weeks to avoid stressing injured tissues.37 After week six, participants were instructed to add gentle pain free inversion motion in varying degrees of plantar and dorsiflexion to facilitate a return to full pain free range of motion and to provide moderate tensile force to the healing ligament. Identified impairments of range of motion, strength, balance and gait were addressed as part of an evidence-based intervention plan consistent with current clinical practice guidelines.38 Treatment was tailored to the severity of the injury with current impairments determining the focus of each treatment session. Interventional strategies aimed to decrease pain and swelling, increase range of motion, strength, weight-bearing and exercise tolerance were used Integration of clinical and sonographic examination of the injury provided the treating clinician information to guide early treatment decisions such as bracing recommendations and weight bearing status. Medication and imaging referral decisions were permitted and determined by the treating physical therapist.
Outcome Measures
All participants provided demographic information and completed patient reported outcomes to include the Foot and Ankle Ability Measure (FAAM) activities of daily living (ADL) and Sports subscale,39 the Foot and Ankle Outcome Score (FAOS),40 Patient Reported Outcomes Measurement Information Systems Global Health (PROMIS-GH),41 Tampa Scale of Kinesiophobia (TSK-11),42 Cumberland Ankle Instability Tool (CAIT),43 and the Numeric Pain Rating Scale (NPRS).44 Participants completed the FAAM, FAOS, PROMIS-GH, TSK-11 and NPRS as well as the Ankle Lunge Test (ALT) and Figure 8 measurements at baseline, 4 weeks, 8 weeks and 12 weeks post enrollment. The FAAM Sport subscale, all FAOS subscales, and the TSK-11 were also collected at 24 weeks while the CAIT was collected at baseline and 24 weeks. The anterior, posteromedial, and posterolateral directions of the Star Excursion Balance Test (SEBT) were assessed at 4, 8 and 12 weeks after enrollment to assess dynamic balance.45–47 Balance was not assessed at baseline to protect injured ligamentous structures.37
Primary Outcomes
The FAAM consists of a 21 item ADL and eight-item Sports subscale. The FAAM demonstrates excellent reliability, responsiveness for ADL participation, and is a valid measure of physical function for individuals with a wide range of musculoskeletal disorders of the lower leg, foot, and ankle.39,48 Each question is scored on a 5-point Likert scale from 4 (no difficulty) to 0 (unable to do). Scores range from 0 to 84 for the ADL subscale and 0 to 32 for the sports subscale.49 To calculate scores the total number of points are added, divided by the total number of possible points and then multiplied by 100. The FAAM has been validated in patients from 9-86 years of age and is a recommended outcome measure for lateral ankle sprains.38,39
Forty-two items that represent five subscales of pain (9 items), activities of daily living (17 items), sport and recreational function (5 items), foot and ankle related quality of life (4 items), and other symptoms (7 items) comprise the FAOS. Each question is scored on a 5-point Likert scale from 0-4 (Never, Rarely, Sometimes, Often, Always). The FAOS has been validated among patients with lateral ankle instability up to 60 years of age and is recommended as an outcome measure for a variety of ankle diagnoses.40 The FAOS demonstrates excellent reliability40 and has established MCIDs for each subscale.50 Additionally, previous literature has established an excellent outcome as >450/500 total score.51
Secondary Outcomes
The CAIT is designed to measure the degree of functional ankle instability.52 This self-reported nine item questionnaire has demonstrated excellent reliability and construct validity, while a discriminant score for functional ankle instability has been determined to be ≤ 25 out of a possible 30 points.43,53 The NPRS is a 0-10 numeric pain rating scale (0 indicating no pain, and 10 indicating the worst imaginable pain) used to assess pain intensity. Numeric pain scales are known to have excellent test-retest reliability.44
Designed to measure pain-related fear of movement/reinjury, the TSK-11 is an 11 item instrument, with all items scored on a 4-point Likert scale (1–4) from “Strongly disagree” to “Strongly agree.”54 The TSK score ranges from 11 to 44, with higher scores indicating greater fear of pain, movement and injury.55 The TSK-11 has been found to be valid, with construct validity determined by the significant correlations between the TSK and Roland Disability Questionnaire, and the Pain Visual Analog Scale.56
The PROMIS-GH is a 10-item short form that efficiently gathers general perceptions of health. Questions assessing global physical health and global mental health are utilized to efficiently summaries physical and mental health in patient reported outcomes with higher scores indicating better global physical and mental health.41
The ALT was used as a weight bearing measurement of ankle dorsiflexion and is considered more functionally relevant than a non-weight bearing measurement.31 It is a common way of measuring ankle dorsiflexion among various ankle injuries and has demonstrated excellent intra and inter-rater reliability.31,57 Minimal detectable change (MCD) and minimal clinically important differences (MCID) for each outcome measure is detailed in Table 2.
Dynamic balance
The SEBT is a quick and inexpensive method of measuring balance with good reliability.59 The SEBT consist of eight reach directions with previously published studies establishing acceptable intra-tester and inter-tester reliability in health young adults.46 Based on findings of shared variance across the eight reach directions the recommendation has been made that assessment of only three reach directions (anterior, posteromedial, posterolateral) be performed.60 Four practice trials were performed on each limb and in each of the three reach directions.46 The average of three measured trails was calculated and normalized to leg length. A composite score was also calculated.59
Statistical Analysis
A priori significance was set at p ≤ 0.05 for all analyses with a sample size estimate of 18 participants being needed to detect a 22.5 point change in the FAOS sport subscale, α =0.05, β =0.20.51 Descriptive statistics were calculated for participant demographics and all patient reported outcome measures. Prior to statistical comparison analysis, Levene’s test of homogeneity of variance, Shapiro-Wilk test for normality and Mauchly’s test of sphericity were performed. Primary and secondary outcomes with three or more levels of measure were analyzed using a repeated measures analysis of variance, with time as the within-subjects factor. For significant findings a post hoc analysis was performed with a Bonferroni correction applied. Secondary outcomes with two data points were assessed via paired t-test. Data were analyzed using Statistical Package for Social Sciences (SPSS) Version 27.0 (IBM, Inc., Armonk, New York).
Results
Twenty-five consecutive individuals were screened for eligibility with ten choosing not to participate due to the time commitment of the study and one individual not participating due to an identified foot fracture. Fourteen individuals met the inclusion criteria and consented to participate in the study (Table 3). All participants completed all in-clinic treatment and data collection at 12 weeks but only eleven participants completed patient reported outcome measures at 24 weeks.
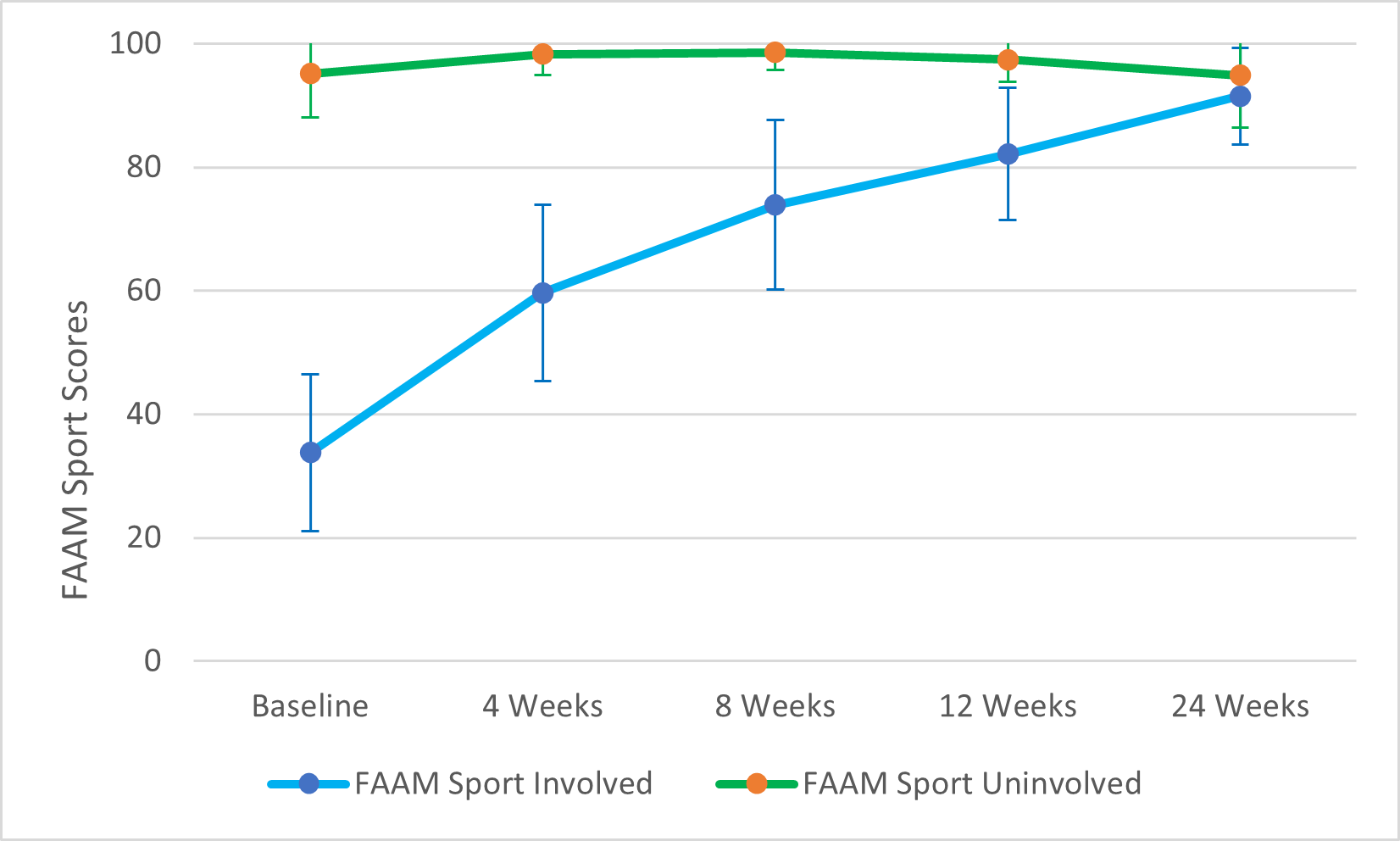
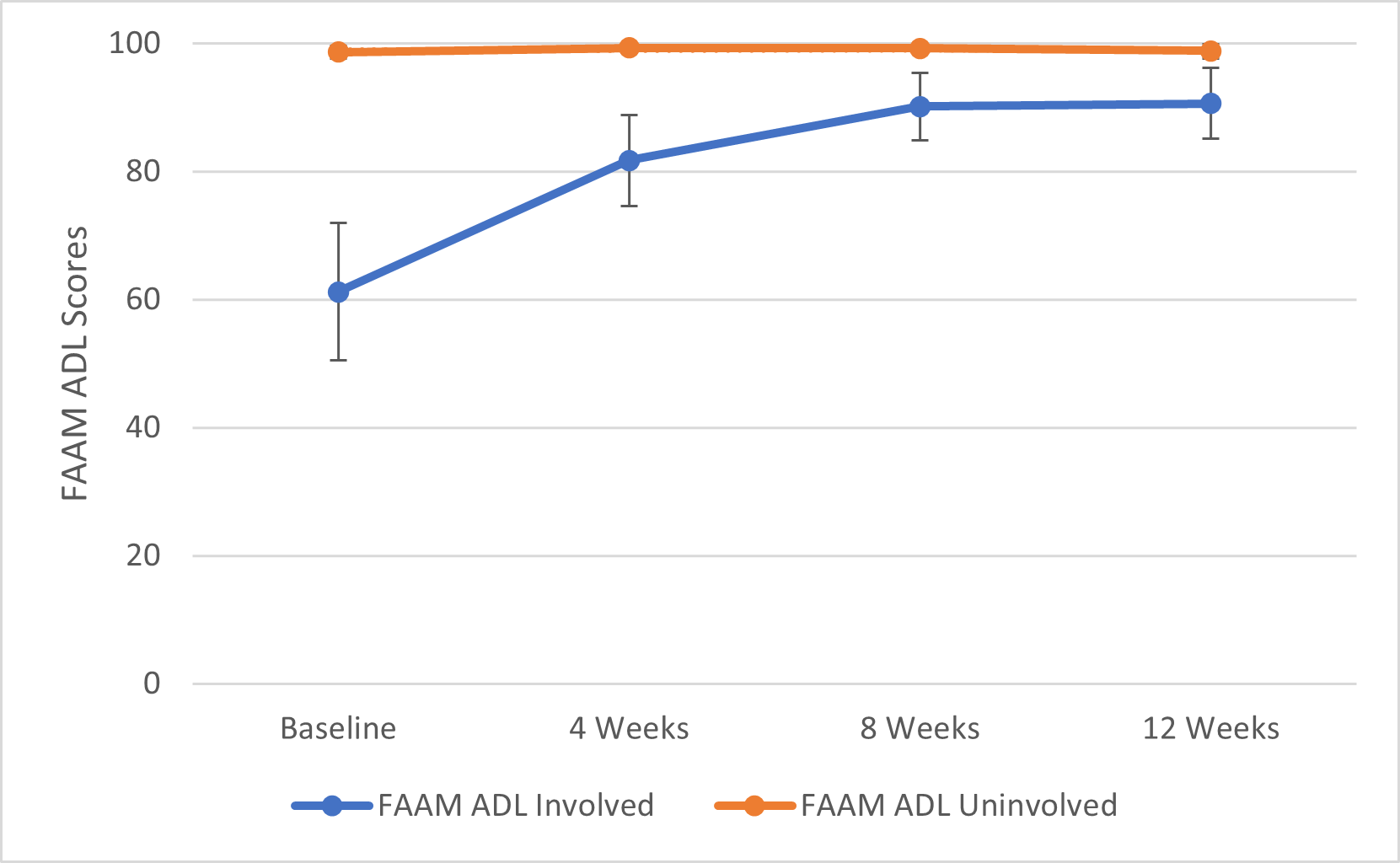
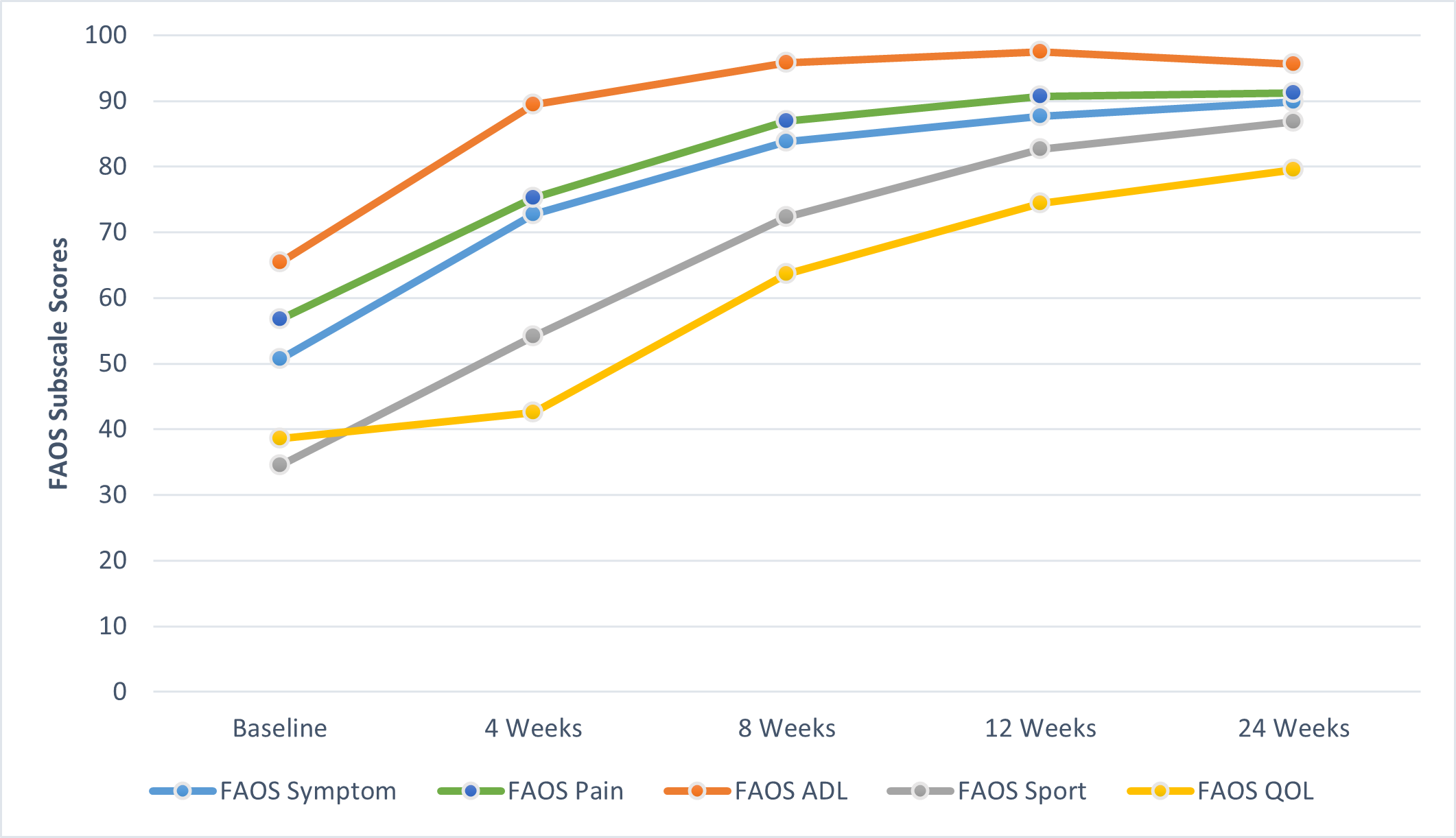
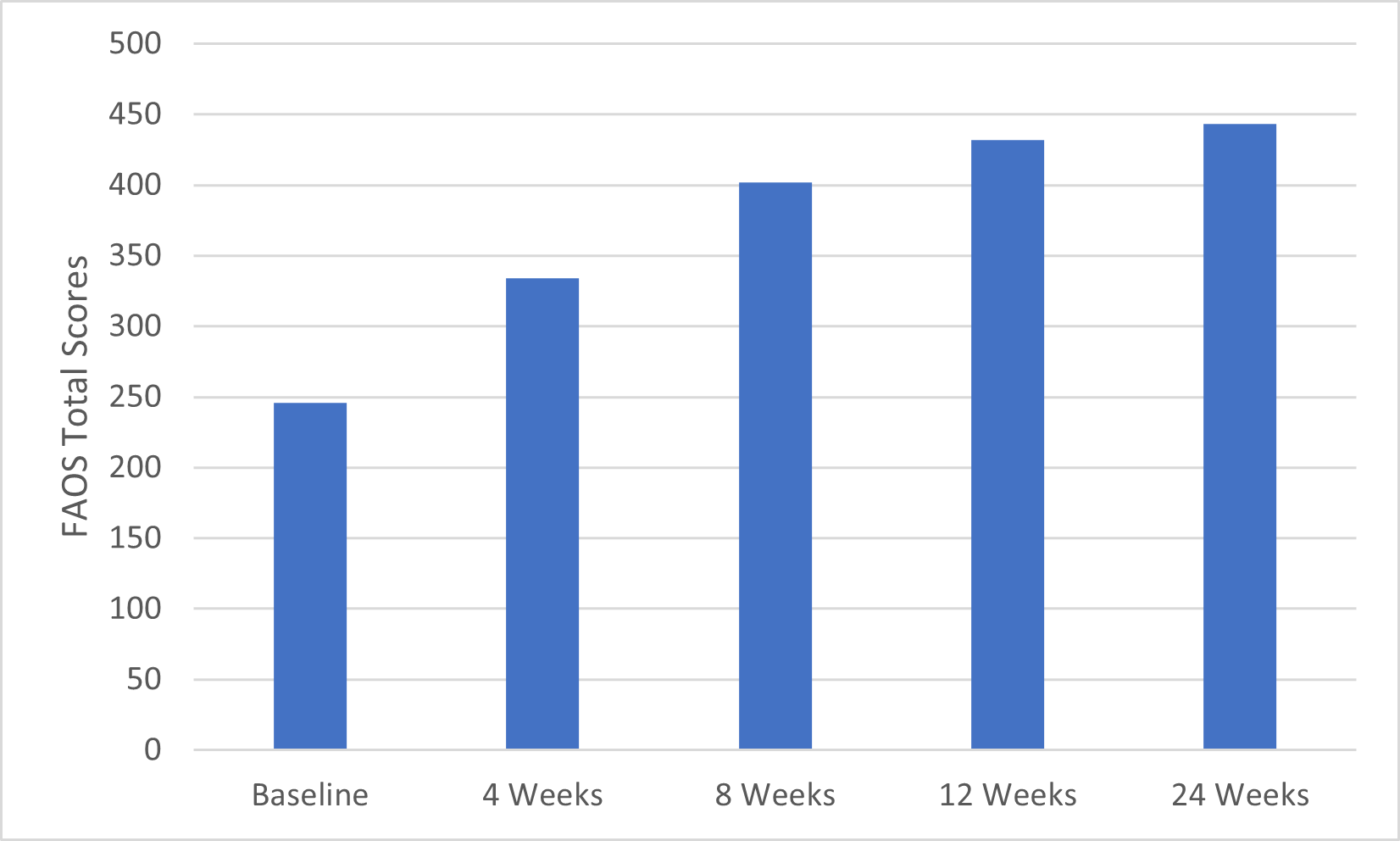
FAAM ADL scores of the involved side significantly increased at 4, 8 and 12 weeks compared to baseline with score improvement at 4 and 8 weeks exceeding the MCID of 8 points, compared to the previous time point. FAAM sport scores of the involved side significantly increased at all time points and exceeded the MCID of 9 points when compared to the previous time point at 4, 8, and 24 weeks. An 8.2-point improvement was observed between weeks 8 and 12. Lastly, all component scores of the FAOS and total scores were significantly increased compared to baseline measurements except for Sport scores at four weeks and Quality of life scores at four and eight weeks. Pain, Other symptoms and ADL subscale MCIDs of the FAOS were initially exceeded at four weeks, while Sport and Quality of life scores exceeded MCIDs at eight weeks. FAAM Sport and ADL scores are also shown graphically in Figure 1 and Figure 2. Individual FAOS score are detailed in Figure 3 and total FAOS scores are shown in Figure 4.
._error_bars_.png)
_subscale_scores_(involved_and_unin.png)
_subscale_scores._activities_of_daily_living_(adl)_and_.png)
_total_scores.png)
Secondary Outcome Measures
Statistically significant differences were observed in 15 of 17 secondary outcome measures across multiple time points. All primary and secondary outcome measures are detailed in Table 4.
Discussion
This case series of ultrasound guided early management and ligamentous protection of lateral ankle sprains observed significant improvement in primary functional outcomes across all data points from baseline to 24 weeks. While conducting this case series, the authors observed that detailed evaluation of lateral ankle ligaments and grading with ultrasound can provide valuable information to guide clinical decisions such as bracing strategies and functional rehabilitation while improving management.29
The continued improvement in primary outcomes from baseline to 24 weeks suggest that a ligamentous injury to the lateral ankle is not one in which full anatomical and functional recovery is rapidly obtained. The application of a tailored management plan with an emphasis on ligamentous protection, guided by POCUS findings shows promise in the management of this injury. Sport and ADL subscales of the FAAM and FAOS both showed large improvements from baseline to eight weeks with a ceiling effect being observed with FAAM and FAOS ADL scores from 8 to 24 weeks. FAAM Sport subscale scores continued to exceed the MCID through 24 weeks when compared to the previous data points, possibly due to higher level function associated with sporting activity being slower to return than tolerance to daily activities.
Secondary measures assessing global physical health, pain, range of motion, ankle edema and dynamic balance revealed significant improvement when compared to baseline data. ALT scores of the involved limb showed improvement from baseline to eight weeks, with a slight decrease in scores from eight to 12 weeks. Improvements on the involved side from baseline to four weeks and four weeks to eight weeks met or exceeded the MDC of 1.9 cm. It was observed in this case series that rehab strategies focused on restoring range of motion and bracing strategies based on clinical practice guidelines did not result in prolonged joint stiffness or a loss in dorsiflexion range of motion.38,61–64
TSK-11 scores from baseline to 24 weeks improved from 28.0 to 21.5, exceeding the MDC of 5.6 points, suggesting a decrease in pain related movement and fear of reinjury.49 All individuals scored well below the threshold score of ≤ 25 on the CAIT at baseline with a mean score of 7.1. A 14.1-point improvement was observed over 24 weeks which exceeded the MCID of ≥ 3 but only one of eleven participants completing the CAIT at 24 weeks scored above 25 points, indicating that 90% of participants continued to be classified as having CAI of the injured ankle, which is associated with increased recurrence.53
For dynamic balance, there was a significant difference in normalized anterior reach direction scores and composite scores of the involved limb at eight and 12 weeks when compared to initial data collected at four weeks, suggesting that improvements in dynamic balance were maintained.
The results of this case series are consistent with the findings of Sanjay et al. who reported on the management of 80 grade one and grade two lateral ankle sprains with ultrasound guided management and bracing strategies.65 Grade two ankle sprains were braced for six weeks with a short leg synthetic cast with restricted weight bearing for the first four weeks.65 The current case series utilized functional bracing (Table 1) for six to 12 weeks depending on injury severity that allowed for full weight bearing during this time period. Improvement in outcomes over the first eight weeks of treatment was observed with the use of functional bracing
Brison et al. conducted a randomized controlled trial of 503 participants to assess the efficacy of supervised physiotherapy in the management of clinically diagnosed grade one and grade two acute ankle sprains.51 Results at four weeks for FAOS ADL and Sport scores in a per protocol analysis showed mean differences favoring physiotherapy care and reported mean scores of 28 and 34 respectively, while the current study observed mean ADL scores of 89.4 and Sport scores of 54.1 at four weeks. Brison et al. also reported FAOS ADL scores of 37 and Sport scores of 58 at 24 weeks, compared to the current study reporting FAOS ADL scores of 95.6 and Sport scores of 86.8, in which 65% of participants were classified as a Grade 2 sprain and 30% classified as a Grade 3 or 4 sprain while utilizing a more restrictive bracing strategy for the first six to eight weeks.
In this case series, FAAM ADL score improvement from baseline to 12 weeks of 28.1 points and FAAM Sport score improvement from baseline to 24 weeks of 57.7 points, exceeded previously published MCIDs of 8 points for the ADL and nine points for the Sport subscale.39 Similar improvement in the FAOS ADL and Sport scores from baseline to 24 weeks of 30.2 and 52.3 points, exceeded the MCIDs of 17.6 and 22.5 points respectively.50 In this case series it was observed that the management strategy described above was beneficial in the management of lateral ankle sprains in the included participants. It was observed that more restrictive bracing strategies focused on ligamentous protection to promote healing and reduce re-injury rates did not result in worse outcomes over a 24-week period. Early and accurate diagnosis is critical to the proper management of acute musculoskeletal injuries. During the initial phase of an acute injury, ligamentous tissues remain mechanically weak and subject to reinjury.66 This is due to the fact that significant improvements in mechanical ligamentous stability do not occur until at least six weeks to three months after injury.67 During this process, acute inflammatory, proliferation and remodeling phases are ongoing with increases in tissue tensile strength not seen until late in the remodeling phase.66 Patients who return to activity during this time period are at an increased risk of reinjury and further disease progression.23,68 The timeline for returning to activity is highly dependent on the severity of the injury and phases of tissue healing.66 Utilizing a progressive rehabilitation process while protecting fragile and injured structures should be the primary focus following injury.69,70 This manuscript is one of the first to describe and observe the use of POCUS guided clinical management of lateral ankle sprains along with ligamentous protection. These findings provide a model for the integration of POCUS examination of lateral ankle sprains into clinical practice and warrant further research.
Over the course of this case series two participants suffered additional inversion ankle injuries.
One participant sustained an inversion injury of the uninvolved ankle at 22 weeks post enrollment, resulting in decreased FAOS scores across all subscales and a reduced FAAM sport score of the uninvolved ankle at 24 weeks. A second participant reinjured the involved ankle while stepping out of the shower at 11 weeks post enrollment, resulting in a significant decrease in the individual’s SEBT scores at 12 weeks. SEBT scores of all other participants continued to improve at this time point. The 14% re-injury rate observed during this case series is consistent with previously reported re-injury rates of 14-17%.71
The current study had several strengths including the implementation of POCUS-guided management of lateral ankle sprains and ligamentous protection strategies. The pragmatic management approach along with a heterogenous sample of injury severity and acuity is consistent with current clinical practice and may aid clinicians in managing this patient population.
This study has several limitations. The first is the small number of participants, rendering it a case series, due to insufficient number of subjects to achieve power while also increasing the chance of a type I error. Second, all participants were from a single patient group, which may limit generalizability beyond this population. Future research should investigate this management strategy with a comparison group and longer follow up periods.
Conclusion
Using POCUS to guide early management and ligamentous protection of lateral ankle sprains may be useful in improving function and return to sporting activity. When comparing the results to previously published studies that did not adhere to any or used less restrictive ligamentous protection strategies, primary and secondary outcomes in this case series were observed to be equal to or improved at higher rates.51,65 The use of POCUS can help accurately diagnose ligamentous injuries, enabling the implementation of protection strategies specific to the grade of ligamentous injury, while also maintaining joint function and overall joint health. The observations from this study suggest that conservative functional bracing strategies focused on ligamentous protection to promote healing and reduce re-injury rates does not delay improvement in functional outcomes.
Conflicts of Interest
None
Disclaimer
The authors are military service members or employees of the U.S. Government. This work was prepared as part of their official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C. §101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. The views expressed herein are those of the author(s) and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, the Department of Defense, nor any agencies under the U.S. Government. The study protocol was approved by the San Antonio Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Research data were derived from an approved San Antonio Institutional Review Board protocol, number C.2021.104d.