
Introduction
Following traumatic knee injury, treatment recommendations include thorough guidelines of phase-based physical rehabilitation with focus on restoring function of the knee and surrounding structures.1–3 Recent research has shown that psychological factors are also important for ensuring return to sport,4–6 and existing recommendations include addressing these psychological aspects.1–3 However, the degree of detail is scarce in comparison with physical rehabilitation, with limited descriptions of psychological interventions. The observed associations between psychological factors and failure to return to sport7,8 indicate that rehabilitation may not be taking full advantage of psychological interventions to prepare people both physically and psychologically for return to sport.
Suggested methods of improving psychological aspects related to rehabilitation include general support and encouragement. Specific structured psychological skills training interventions are evidence-based methods that aim to improve enjoyment, motivation, and performance, for example. Psychological factors have been shown to be important for both return to activity outcomes, as well as risk of reinjury,9 indicating a need for targeted strategies. Goal-setting, arousal regulation, and imagery are examples of psychological skills training interventions as methods of improving psychological factors following traumatic knee injury.2,3 Research indicates that these interventions are effective for improving psychosocial10 and performance11 outcomes. However, intervention studies on injured populations are less prevalent, and show varying degrees of efficacy.12 Physical therapists (PTs) describe a lack of psychological strategies in qualitative interviews,13,14 and research suggests persisting psychological problems,8,15 which could indicate that interventions are insufficiently implemented.
Clinicians and researchers may need a better understanding of current clinical methods and perceptions on the use of psychological interventions during rehabilitation. This may help to address the identified knowledge gap regarding methods of influencing physical and psychological factors to aid in reaching successful rehabilitation outcomes. Research is sparse, with only one recent study surveying physical therapists (PT’s) and physical therapy (PT) students regarding views of and education in psychological interventions during rehabilitation.16 Addressing this gap could lead to further development of strategies to ensure that both physical and psychological readiness to return to sport are addressed. The aim of this study was to investigate whether, and to what extent, Scandinavian physical therapists address psychological factors in treatment of physically active people with traumatic knee injury.
Methods
Design and Participants
The study used a cross-sectional online survey design reported according to the Checklist for Reporting of Survey Studies (CROSS) Guidelines.17 Data were collected using Survey and Report (Artisan Global Media), hosted by Lund University.
Clinically active PTs in Denmark, Norway, and Sweden who regularly treated physically active people with traumatic knee injury (at least five per year on average to ensure data on commonly used strategies) were eligible for inclusion. PTs involved in the MOTIFS study, a randomized controlled trial coordinated by the first author which integrates imagery into rehabilitation training,18 were excluded.
Procedures
Survey Development
The study-specific survey was developed in English by the authors, then translated and cross-culturally adapted by experts with native-language proficiency in Swedish, Danish, and Norwegian, respectively. Translation was aided by the free online artificial intelligence translation tool DeepL Translator,19 checked for consistency by the authors and pilot-tested twice on third-party (n=7) people familiar with PT and research. An overview of the survey (not including demographic questions) is provided in Table 1. The full survey, including answer alternatives, is available in Appendix 1.
Based on literature searches and expert discussion on current recommendations and common clinical practice regarding use of psychological skills training, the domains “Specific Understanding of Psychological Skills Training” and “Need/Desire for Further Education” were identified. Within these, three psychological skills training principles were identified as important to return to sport or activity outcomes: goal-setting (short- or long-term rehabilitation goals), imagery (mental and/or physical simulation), and arousal regulation (regulation of physical and psychological stress).16,20 Each of these were further categorized into the constructs “Use,” “Confidence,” “Importance.” A “Target Group” was also included, inspired by previous research.21,22 Included in the “Use” construct are questions regarding direct or indirect involvement of other activity-specific actors such as coaches in treatment strategies.
Thirty-two items are included in the survey, with between 20 and 30 items possible based on conditional logic. Nine items record demographic and background information, including location, experience, and education. Four additional items collect consent and confirm exclusion criteria (if relevant). The Swedish version includes an extra exclusion criterion regarding involvement in the MOTIFS study.18
Thirty items are single- or multiple-choice, in which participants answer according to one or several alternatives, respectively. Items on the constructs Confidence and Importance include a 1 (low) to 5 (high) Likert-type scale (i.e. 1 [not confident at all] – 5 [extremely confident]). The Use and Target Group constructs include example alternatives (i.e. “once in the beginning,” “once per phase,” etc.). Item 31 is a matrix, in which six alternatives (brochures, popular science materials, academic articles, workshops, professional courses, and formal education) are rated on their perceived utility, and item 32 is optional, allowing free-text suggestions.
Data Collection
Participants were recruited according to a convenience and snowball sampling method, distributed via personal contacts and social media using a language-specific survey link, in which responses from one computer were restricted for 10 minutes after entering the survey link.
Data Analysis
Due to the exploratory nature and lack of studies regarding this topic, no sample size was defined. Demographic and background variables were presented on a group level, exported from the data collection software into the IBM SPSS (v29) statistical software package. Results are presented as median (IQR) and/or number (percent) to present the full context of the results and prevalence for each answer alternative. Free-text responses were translated to English using the DeepL Translate tool,19 checked by native speakers of each language, and categorized based on similarity. Responses to all questions were required, so no data was missing.
Ethical Considerations
All participants received written information, and informed consent was collected. All data was stored on a secure server at Lund University in Sweden. Ethical approval was not required according to the Danish, Norwegian, and Swedish ethical review regulations, as responses are anonymized and do not include any sensitive data.
Results
Demographics
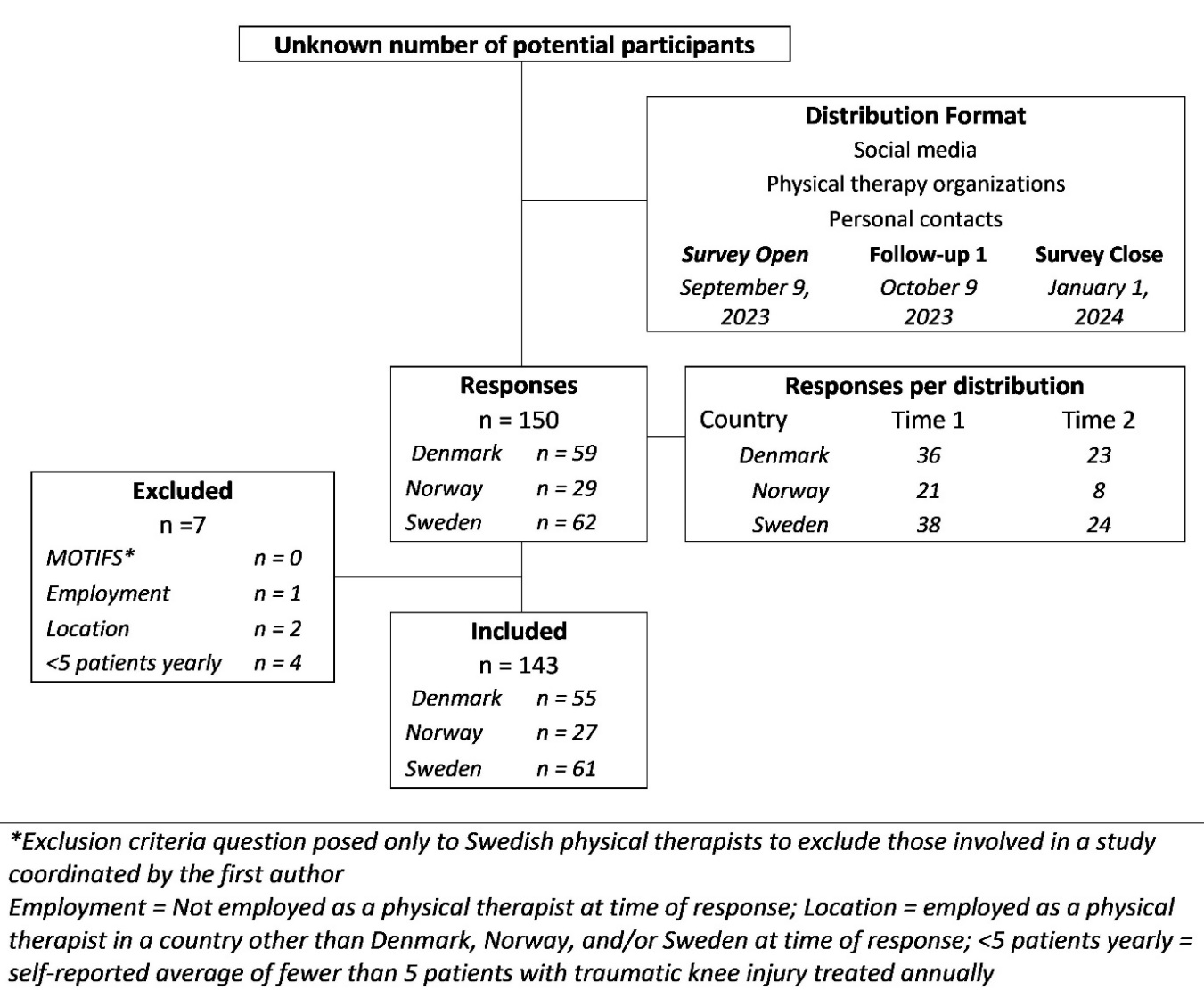
Responses were collected between September 2023 and January 2024 (Table 2) from n=150 PTs, n=143 of whom were eligible for inclusion (participant flow diagram in Figure 1). Median age of participants was 41-50 years, with median experience greater than 11 years.

Return to Activity Testing
Responses indicate that n=142 (99%) use physical return to sport testing, the most common of which are strength and functional hop measures (Table 3). Psychological measures are used by n=135 (94%), most commonly discussions with the patient and behavior observation. Structured psychological follow-up strategies are reported as being used by n=132 (92%), most commonly patient education.
Psychological Skills Training Use
Goal-Setting
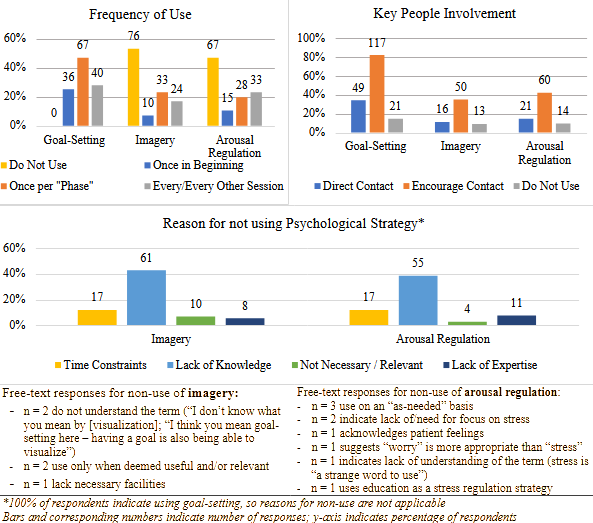
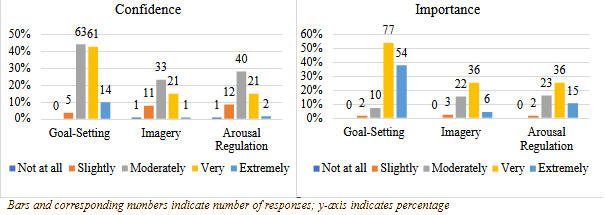
Goal-setting was used by n=143 (100%). Sixty-seven (47%) use goal-setting once per phase; n=117 (82%) report encouraging use through direct contact with key people (Figure 2). Importance (median 4 [IQR 1]), and confidence (median 4 [IQR 1]) are shown in Figure 3. Goal-setting use with different patient groups is shown in Figure 4. Free-text responses included n=1 clarifying special attention to non-physically active people who require physical training for their rehabilitation.

Imagery
Imagery was used by n=67 (47%). Imagery was most frequently reported as being used once per phase (n=33; 23%); lack of knowledge was the most frequently reported reason for non-use (n=61; 43%), and n=50 (35%) reported encouraging use through direct contact with key people (Figure 2). Importance (median 4 [IQR 1]), and confidence (median 3 [IQR 1]) is shown in Figure 3. Figure 4 shows use of imagery with different patient groups.
Arousal Regulation
Arousal regulation was used by n=76 (53%); n=33 (23%) reported use every or every other session; lack of knowledge was the most frequently reported reason for non-use (n=55; 38%), and n=60 (42%) report encouraging use through direct contact with key people (Figure 2). Importance (median 4 [IQR 1]), and confidence (median 3 [IQR 1]) are shown in Figure 3. Arousal regulation use with different patient groups is presented in Figure 4.


Need/Desire for Further Education
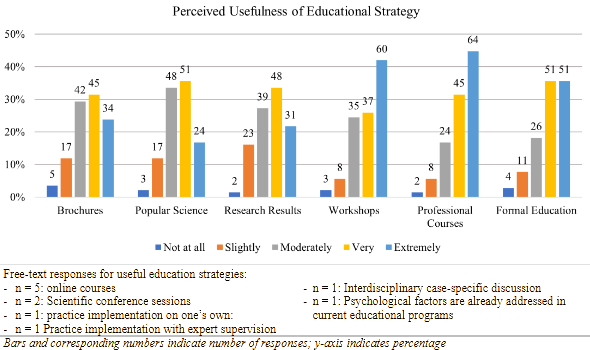
Perceived usefulness of educational strategies is presented in Figure 5. Professional courses were rated as having greatest perceived usefulness (median 4, IQR 1).

Discussion
Results of this study suggest that goal-setting is a commonly used psychological strategy by Scandinavian PTs in the treatment of patients with knee injury. Use of imagery and arousal regulation was reported by only approximately half of respondents, despite perceptions of these strategies as being very important in helping people with psychological factors during rehabilitation. Relatively few PTs report directly involving key people, instead encouraging the patient to initiate this contact. The most frequently reported reason for not using imagery and arousal regulation strategies was lack of knowledge. To address this gap, respondents indicate that practical workshops and continuing professional development courses would be useful tools.
Literature has shown that psychological factors are important for return-to-activity outcomes,4,23 and current recommendations include increasing focus on these factors during rehabilitation.2,3 However, results of this study confirm qualitative research results indicating a general lack of knowledge on what constitutes psychological measures and interventions.13,14 The vast majority of PTs indicated that they use psychological return-to-activity measures (most frequently discussion with the patient and observation of behavior). Previous research suggests, however, that PTs have insufficient knowledge of what questions to ask to gain insight into the sources of patients’ psychological difficulties.14 This could potentially explain the current results indicating follow-up strategies of educating patients and reducing physical training load rather than targeted psychological interventions.
The fact that PTs indicate a need and/or desire for practical education in the form of workshops or courses indicates a continued dualistic perspective in rehabilitation, in which physical and psychological factors are separate, rather than adopting a holistic perspective. Lack of proper education in psychological interventions despite considerable evidence of their importance indicates that physical therapy culture has not adopted the necessary holistic approach which has long been advocated. It is therefore important for researchers and practitioners to focus on increasing the knowledge base in order to develop methods of delivering structured and evidence-based interventions in the clinic.
Goal-setting seems to be a well-used intervention by Scandinavian PTs, as all respondents included in this survey indicate use. However, due to the formulation of the questions, it is difficult to know how this was implemented in practice. Previous research has indicated that goal-setting occurs mainly through the PT informing of goals,13,14 rather than dynamic and learning-based goals as outlined in current goal-setting theory.24 This is an important distinction to make, as inappropriate goal-setting may have detrimental effects, including inhibition of proper learning, misrepresenting efforts (i.e. lying about compliance), and/or skipping steps to stay on schedule.24 In sport injury rehabilitation, it is therefore imperative that PTs are able to deliver a goal-setting intervention which follows convention and has a positive psychological effect. Future research should explore intervention delivery methods to design pragmatic instructional guides for clinicians.
Imagery interventions were used relatively infrequently, and several free text responses indicated confusion regarding terminology, including one respondent confusing imagery with goal-setting. Based on the results, one can only speculate, but it is possible that PTs are mis- or uninformed regarding imagery. Modern imagery practice has moved beyond quietly and statically sitting while imagining execution,25 instead incorporating movement to create physical and psychological realism.26,27 Clinicians and researchers should further explore using imagery to prepare for return-to-activity in terms of real-world challenges such as dual-task demands28 and pain,29 for example. Previous research on injured populations shows that imagery training may be beneficial in terms of pain, muscle activation, strength, performance30 and self-reported knee function.31 Additionally, imagery interventions have been shown to reduce stress hormones in people with knee injury,32 indicating potential for use as an arousal regulation intervention.
Arousal regulation includes reducing, maintaining, or enhancing physical and/or psychological states to fit the needs of a goal-directed situation.33 This includes controlling one’s stress response to match the situation.34 for example by calming down or “pumping up.” However, several respondents suggested that “stress” is an inappropriate word choice, indicating a problematic misunderstanding of the stressful nature of sport injury and subsequent rehabilitation. Psychological stress is recognized as both a potential cause and an effect of sport injury,35,36 and PTs indicate stress as a pressing issue with patients.14 In the context of sport injury rehabilitation, the goal is often to return to some form of activity, so it is essential that the person can control their levels of stress and arousal to handle the requirements upon return to activity. This is supported by calls for improving dual-task motor control during physical performance with sport-specific external stimuli.37,38
Social support and engagement are important aspects to sport injury rehabilitation,4 especially in implementing psychological skills training interventions. PTs foster self-determined motivation by relating to patients,39,40 discussing proper goal-setting, individualizing imagery, and encouraging arousal regulation techniques. Outside the clinic, this could also include discussing these supplements to rehabilitation methods with key people such as coaches or training partners. Results of this study indicate that very few PTs actively initiate contact with people key to their activity, instead encouraging the person to take the initiative themselves. This therefore represents a missed opportunity to take a truly holistic approach to well-being and rehabilitation. Future research should also examine other key people such as friends and family, as social support from all areas of life is important.
The rehabilitation literature has identified psychological factors as important for rehabilitation outcomes,4,5 and called for increased focus on these factors during rehabilitation,2 but suggests that these are likely not addressed to an appropriate extent.13,14 Results of this study indicate that psychological interventions are not often used, and physical therapists express a desire for education in implementation methods. Following injury, unpleasant feelings are natural and frequent and difficult to get rid of, PTs should help athletes commit to good rehabilitation behaviors and formulate goals during and after the injury period. Sport psychology approaches such as mindfulness and acceptance can help athletes accept (unpleasant as well as pleasant) inner experiences, engage in the present moment and commit to valued behaviors.41 Additionally, proper use of imagery interventions may be a pragmatic clinical tool for preparing people for return to the demands of their activity by creating more meaningful and relevant training. Providing holistic rehabilitation interventions to meet recommendations for treatment of people with knee injury may be an easily implemented method of encouraging more physically and psychologically sound rehabilitation.
Strengths and Limitations
Strengths of this study include the use of a specifically designed and cross-culturally adapted survey to explore PTs’ perspectives on their own use of psychological skills training, exploration of which has been lacking in the literature despite current recommendations. This provides highly relevant information for both clinically active PTs as well as researchers, as it allows for insight into practical use of underrepresented psychological training. Additionally, results provide information which can inform future pragmatic implementation. The survey was developed with feedback from, and pilot tested on, clinically active PTs and researchers, which increases the reliability and relevance of the questions posed, though measurement properties have not been evaluated. Including sports psychologists in the development also allows for a more holistic approach to this interdisciplinary study.
One potential limitation is that the invitation informed participants that the survey aimed to examine psychological skills training use in rehabilitation of knee injury, possibly dissuading those who do not address psychological factors, potentially limiting generalizability. There may also be a sampling bias limiting generalizability, as the contacted groups may not represent the general PT population. Additionally, the size of the potential participant pool is unknown, given that targeting strategies included several social media platforms, increasing likelihood of multiple exposures. It was not possible to identify whether participants registered more than one response, but this is unlikely due to the extent of the survey. The multiple-choice questions may limit validity of responses; for example, options for use of psychological strategies for determining readiness to return to activity include “motivational strategies,” resulting in difficulty in drawing conclusions regarding clinical applications.
Conclusions
While goal-setting use was reported by all PTs, a persistent underuse of other aspects of psychological skills training in rehabilitation following traumatic knee injury, suggesting that best-practice recommendations are not being followed. Future efforts need to focus on providing proper education in holistic and person-centered rehabilitation paradigms to address physical, social, and psychological aspects of sport injury. This should include information on identifying psychological factors, proper methods of communication to address these factors, and methods for clinicians to administer structured psychological interventions.
Conflict of Interest
The authors declare no conflicts of interest.
Data Availability Statement
Data available upon reasonable request.
Acknowledgements
The authors would like to thank Kristian Thorborg for providing feedback on study design and research questions, Axel Ström for statistical guidance, the Danish Sports Physical Therapy Association (DSSF) for help distributing the Danish version of the survey, and the Swedish Association for Physical Activity and Sports Medicine (SFAIM) and the National Network for ACL Research for help distributing the Swedish version of the survey. This study has received funding from the Swedish Research Council; no funding source or other organization had any role in design, implementation, or analysis in this study.