
INTRODUCTION
Functional thoracic spine mobility is crucial for normal components of daily living such as reaching arms overhead and turning to look behind oneself, but is even more critical in rotational sports such as baseball, golf, and swimming where loss of normal thoracic mobility can increase risk for injury and diminish performance.1–5 Impairments involving the thorax have been linked to musculoskeletal pathologies in both the axial and appendicular regions of the body, including dysfunctions in the upper and lower extremities.6–9 Many of the established clinical practice recommendations for the treatment of pain in the neck, low back, shoulder, and even elbow include interventions that address movement dysfunctions and mobility restrictions within the thoracic spine.6–8,10–12 Because knowledge regarding the impact of thoracic function on regional pathologies is growing, especially in athletic populations, and due to the frequent utilization of interventions that address the thorax (consisting of the thoracic vertebrae, ribs, sternum, thoracic viscera, and muscles attaching in and acting on the region), it is important for clinicians to be able to quickly and reliably assess isolated range of motion (ROM) of the thoracic region.
A multitude of reliable ROM measurement procedures exist that attempt to reduce the contribution of the lumbar spine when quantifying thoracic mobility.13–15 Of these known measurements for the thoracic region, none claim to isolate the movement of the thoracic spine from the lumbar spine during spinal rotation other than the quadruped lumbar-locked position.14,15 The quadruped lumbar-locked position utilizes maximal hip and lumbar spine flexion to “lock” these regions from potential contribution to the thorax rotation motion.14 Researchers have suggested that the lumbar-locked thorax rotation testing method results in a more accurate representation of isolated thoracic spine rotation ROM by minimizing the confounding contributions from adjacent joints.14 Additionally, the quadruped lumbar-locked position has demonstrated good intertester (ICC = 0.87), intratester (ICC = 0.87-0.90) and test-retest (ICC = 0.88-0.90) reliability when using a bubble inclinometer placed at the T1-2 vertebral level.14
While obtaining a reliable numerical measurement with a device is crucial in quantifying clinical progress, it may not be necessary when testing for gross passive and active physiological deficits in the thorax. Previous authors have noted the accuracy and clinical importance of visual measurements for joints such as the proximal interphalangeal and metacarpophalangeal joints of the hand, and radiocarpal joint of the wrist.16,17 Visual measurements can aid clinicians in efficient assessment strategies which can maximize time dedicated to implementation of interventions. However, the reliability and validity of a visual estimation of thoracic rotation ROM using the quadruped lumbar-locked position is unknown. Establishing the reliability and validity of visual estimation for the quadruped lumbar-locked thorax rotation test could greatly improve its utilization in the clinical setting but also in sideline assessments or pre-participation exams for athletes where time is often limited. Therefore, the purpose of this study was to establish the reliability and discriminant validity of visual estimation of thorax rotation range of motion across clinicians of differing experience levels in determining normal mobility and active or passive physiological deficits when utilizing the quadruped lumbar-locked position.
Because accurate measurement of range of motion and interpretation of findings is an entry level skill for the physical therapist, it is crucial that physical therapy students and clinicians alike are capable of reliably assessing for mobility deficits in all regions of the body. Therefore, it was hypothesized that an expert clinician, orthopedic physical therapy resident, and physical therapy student would demonstrate “good” inter-rater reliability (k=0.40-0.59) when identifying normal mobility, and active and passive deficits in thoracic rotation. It was hypothesized that subjects identified with active and/or passive physiological restrictions would have lower ROM values compared to subjects with normal mobility.
MATERIALS AND METHODS
Study Design
A prospective cross-sectional design was used to establish the reliability and validity of the visual estimation of the lumbar-locked thorax rotation test among raters of differing experience levels. The study was approved by the Institutional Review Board at the University of Evansville and informed consent was read and signed by all subjects prior to data collection.
Participants
A minimum sample size of 24 subjects was needed to detect a kappa value of >0.40 for a two-tailed test with an alpha level of significance equal to 0.05 and 80% power. A total of 38 individuals (21 female, 17 male) volunteered to participate in the study. Subjects included were active adults recruited from the University of Evansville campus and surrounding community. Inclusion criteria consisted of an active lifestyle defined by the American Heart Association as someone who engages in “at least 150 minutes of moderate intensity aerobic exercise or 75 minutes of vigorous aerobic exercise per week”,18 and an age between 18 and 50 years old. Exclusion criteria consisted of any of the following: current pain, history of spinal surgery with permanent spinal hardware, and inability to get into the starting position for the quadruped lumbar-locked thorax rotation test. Subjects were screened for their ability to get into the starting position in a separate room by a research assistant prior to testing. Subjects were not provided further training regarding the test prior to data collection.
Procedures
The raters included an expert rater (rater A), an orthopedic residency-trained physical therapist (rater B), and a student physical therapist (rater C). Rater A was a licensed physical therapist with a board certification in sports and 12 years of clinical experience. Rater B was a licensed physical therapist who recently completed a residency program specializing in orthopedics with two years of clinical experience. Rater C was a student physical therapist in the second year of a three-year Doctor of Physical Therapy program who had completed one 8-week clinical experience in an outpatient orthopedic clinical setting. Each rater had consistently used the quadruped lumbar-locked thorax rotation test in clinical practice prior to the study.
The raters and research assistants completed a training session one week prior to data collection in order to review the standard testing position, stabilization contact points, and planned order of operations as well as to ensure that the tester could stay blind to the measurement device throughout testing. Additionally, research assistants who were involved in measuring thoracic rotation ROM using the digital inclinometers performed a palpation and measurement skills check-off with the expert rater. The purpose of the skills check off was to ensure the research assistant’s ability to palpate the T1-2 interspinous space by counting down from C7 while the participant was in the quadruped position. Further, the training session allowed each research assistant to calibrate their inclinometer device to the horizontal and the vertical which permitted each research assistant to correctly identify the axis for the zero start and ending positions using the digital inclinometer.
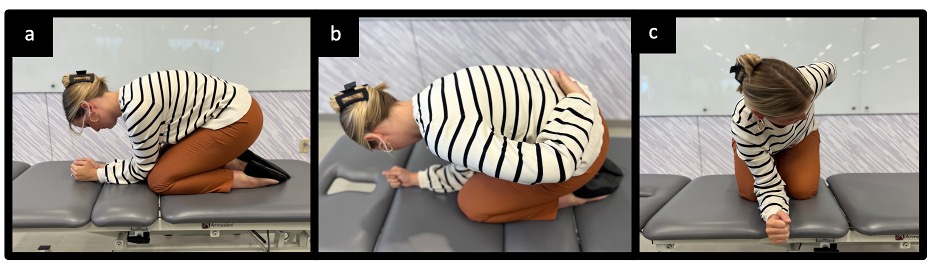
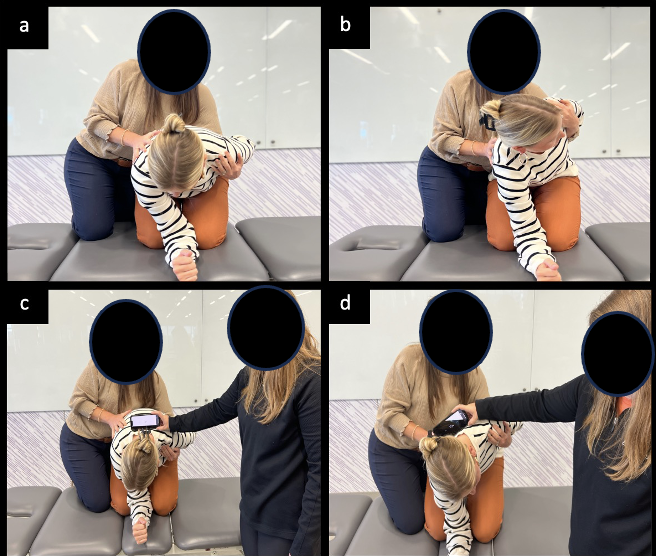
The order in which subjects were evaluated by each rater was randomized prior to data collection. At the assigned rater station, subjects assumed the starting position for the quadruped lumbar-locked thoracic rotation test in the manner previously described by Johnson et al.14 and Bucke et al.15 of quadruped with hips and knees in full flexion, and elbows and forearms resting on the plinth in front of knees (Figure 1a). The testing position for the quadruped lumbar-locked thoracic rotation test was altered from that described by Johnson et al.14 and Bucke et al.15 by having the subjects place the dorsum of the testing-side hand on the sacrum (Figure 1b) before rotating the test side thorax up toward the ceiling (Figure 1c) in the direction of thoracic rotation. Subjects were cued by raters to stay within the imaginary “tunnel” of their body from the starting position in order to avoid side bending of the trunk during the testing motion. Raters observed the active motion of the subject and categorized his or her performance as “Unrestricted” (visually observed 50 degrees thoracic rotation or greater) or “Restricted” (visually observed less than 50 degrees thoracic rotation), while a research assistant simultaneously measured the motion with the Apple iPhone “Measure” application (iPhone© is a trademark of Apple Inc, Cupertino, CA, USA) placed horizontally at T1-2 (Figure 2). This Unrestricted/Restricted criterion was selected based on the previously established normative values for isolated thoracic spine rotation motion.13–15 The rater was blinded to the digital measurement obtained by the research assistant. To obtain a measurement of passive motion, the rater placed the palm of one hand on the anterior aspect of the participant’s shoulder on the side being tested and provided gentle, passive movement in the direction of thoracic rotation up toward the ceiling to the first level of resistance while stabilizing the participant’s opposite shoulder and pelvis (Figures 3a and 3b). The rater categorized the performance as “Unrestricted” or “Restricted” while a research assistant simultaneously measured the passive motion with a digital inclinometer (Apple iPhone “Measure” application) placed horizontally at T1-2 and kept the rater blind to the measurement (Figures 3c and 3d). All testing procedures were performed twice on both the right and left sides and the average of two trials per side were used for data analysis. After completing all measurements with the first rater, the subject repeated the same procedures with the remaining two raters. This process was repeated following a one week washout period in order to capture intra-rater and test-retest reliability.
_starting_position_is_quadruped_on_a_plinth_with_h.jpg)

_start_position__b)_end_position__c)_.png)
Statistical Analysis
Descriptive statistics including means and standard deviations were calculated for all subjects. Intra and inter-rater reliability for all categorical variables were compared between each rater (rater A vs. rater B, rater A vs. rater C, rater B vs. rater C) using a weighted Cohen’s kappa statistic with 95% confidence intervals and percent absolute agreement. Cohen’s kappa statistic quantifies the strength of agreement and was interpreted as: ≤0.40 = poor to slight, 0.41-0.60 = moderate, 0.61-0.80 = substantial, ≥0.80 = excellent.19 Secondary outcomes include lumbar-locked thoracic rotation measurements on a continuous scale using a digital inclinometer. In order to determine discriminate validity, a two-way analysis of variance (ANOVA) with three levels was performed to determine main effects between rater (A, B, and C) and category by comparing the rater’s interpretation of mobility using a previously established threshold of 50 degrees or greater of thoracic rotation (categorized as Unrestricted or Restricted) to a range of motion measurement obtained with a digital inclinometer. Interaction effects were evaluated to determine if differences existed between test performance category (Unrestricted or Restricted) and rater experience level (expert, resident, student). All data were analyzed using SPSS statistical software (IBM SPSS Statistics for Windows, Version 24.0). Tests were considered statistically significant if they did not exceed an alpha level of p < 0.05.
RESULTS
Demographic characteristics of the participating subjects are summarized in Table 1. Significant differences in height (p=0.01) and weight (p=0.01) were noted between male and female subjects. No significant difference in age (p=0.16) was observed. All 38 subjects completed the testing procedures, and the results were included in the data analysis.
Test-Retest Intra-rater and Inter-rater Reliability
Results of test-retest intra-rater reliability following a one-week washout period within all three raters are presented in Table 2, including corresponding Cohen’s kappa values with 95% confidence intervals and percent agreement. Weighted Cohen’s kappa coefficient for test-retest intra-rater reliability demonstrated “moderate to substantial” agreement and ranged from 0.55 to 0.72. Percent absolute agreement ranged from 0.82 to 0.89. The expert rater (rater A) demonstrated the highest level of intra-rater reliability followed by the orthopedic resident (rater B) and finally the PT student (rater C).
Results of inter-rater reliability with Cohen’s kappa values, 95% confidence intervals, and percent absolute agreement are presented in Table 3. Cohen kappa values ranged from 0.45 to 0.59 demonstrating “moderate” agreement between all three raters. Percent absolute agreement between raters ranged from 0.74 to 0.84. Overall agreement was the highest between raters with the greatest clinical experience.
Discriminant Validity
Results for the assessment of discriminant validity using a Two-way ANOVA with three levels are presented in Table 4. Interaction effects were evaluated to determine if differences existed between test performance category (Unrestricted or Restricted) and rater experience level (expert, resident, student) which would allow the researchers to determine if experience level affected the rater’s interpretation of the test. If a significant interaction was not present, then main effects and the mean differences were examined. Two-way ANOVA identified a main effect of category, indicating a significant difference in inclinometer measurements between “Unrestricted” and “Restricted” categories for both active (Unrestricted=54.6-58.9; Restricted=40.4-44.4; p<0.001) and passive measurements (Unrestricted=61.3-63.5; Restricted=39.2-39.7; p<0.001). The only interaction effect present that showed a difference in performance category between raters of different experience levels was for passive left rotation [rater A Restricted =34.3(30.4-38.2); rater C Restricted =43.8(41.3-46.4); p<0.001; (Table 5)].
DISCUSSION
The overarching aim of this study was to establish the reliability and discriminant validity of visual estimation of thorax rotation ROM in the quadruped lumbar-locked position. While several reliable methods for measuring thoracic spine rotation ROM exist, no study to date has established the reliability or validity of utilizing visual estimation in the quadruped lumbar-locked position to test for active and passive physiological deficits of thorax rotation motion. The results of this study support the primary hypothesis indicating that visual estimation of thoracic rotation ROM in the quadruped lumbar-locked position has “moderate to substantial” test-retest intra-rater reliability and “moderate” inter-rater reliability, regardless of clinician level of experience. Consistency among these measures, despite level of expertise, enhances communication amongst clinicians and further validates the therapist’s ability to differentiate between mobility impairments and deficits in strength or neuromuscular control of the thorax.
Similar to previous research, the current study utilized a population of young, healthy individuals and attempted to limit compensatory lumbar motion by positioning the hips, knees, and lumbar spine into full flexion. The lumbar-locked position utilized in the current study was adapted from the positions used by Bucke et al.15 and Johnson et al.14 with both studies using minor positional differences of the upper extremity. Despite minor differences, the results of the current study are consistent with all previous research, which have demonstrated “good” reliability when assessing isolated thoracic rotation motion utilizing the lumbar-locked position.
Unlike previous studies that utilized a measurement tool such as a bubble inclinometer,13,14 universal goniometer,13 or iPhone application15 in determining thoracic spine rotation ROM, this study established the reliability and validity of visual estimation to test isolated thoracic rotation active and passive physiological deficits. Due to its established reliability and validity in previous studies the Apple iPhone “Measure” application was used as the gold standard in this study to compare ROM measurements to Unrestricted/Restricted criteria when establishing the validity of the test.20 It is interesting to note that in the current study the range for differentiating active Unrestricted/Restricted categories (Unrestricted =54.6 to 58.9, Restricted=40.4 to 44.4) were narrower than the passive Unrestricted/Restricted categories (Unrestricted=61.3 to 63.5, Restricted=39.2 to 39.7). Given that the quadruped lumbar-locked starting position allows the acromion processes to align horizontally, and that the ending position for typical thoracic rotation is approximately half-way between the horizontal and the vertical, visual estimation of this motion of the thoracic spine may be easier to assess actively. This may be due to the therapist’s position during the test as the therapist is able to examine the transverse plane motion from a cephalocaudal position relative to the subject. Though the range differed for active motion compared to passive, the performance among raters was similar. Because subjects were performing several series of measurements within a session, the current study attempted to control for carryover effects through randomization of testing order at each rater station. Additionally, only two trials of all testing procedures were performed per side at each rater station in an effort to limit subject fatigue as well as to limit testing effects.
Comparing the agreement of clinical tests among clinicians with various experience levels is a common method for assessing the level of expertise needed to obtain accurate results. Previous studies have not utilized a consistent experience level of raters when establishing reliability of the quadruped lumbar-locked thoracic rotation test. Common methodologies in these studies have used expert clinicians14,15 while others utilized students20 which left the establishment of inter-rater reliability between experience levels of therapists when determining thoracic mobility yet to be explored. Due to the frequent use of students and novice clinicians, such as residents, at pre-participation sports physicals and injury screening events, it is crucial for clinicians at all experience levels to be able to reliably perform field expedient testing such as the quadruped lumbar-locked thorax rotation test in order to identify mobility and neuromuscular impairments. To the authors’ knowledge, this is the first study to compare raters of various experience levels (expert, resident, and student) to establish test-retest intra-rater and inter-rater reliability for visually estimating thorax rotation. The current study found “moderate to substantial” agreement between raters across multiple levels of experience. The clinical implications of this finding are very encouraging as a student physical therapist can assess thoracic rotation ROM similarly to an expert clinician.
Similar to the current study, previous researchers have reported greater intra-rater reliability among clinicians with greater experience when testing the weight-bearing lunge test for ankle dorsiflexion20 and the Functional Movement Screen™.21 While the test-retest and inter-rater reliability of the expert rater (rater A) was consistently higher than that of the student physical therapist (rater C) in the current study, all clinicians were found to have almost perfect agreement on test-retest, and all had moderate inter-rater reliability. The higher reliability of the expert rater (rater A) is likely due to the rater’s ability to determine Unrestricted/Restricted in a narrower range of mobility based on means and standard deviations compared to the more novice raters. A study by Glaws et al21 reported similar findings when establishing intra-rater reliability of the Selective Functional Movement Assessment (SFMA™), which includes the lumbar-locked thorax rotation test. When using criterion checklists, the rater with the greatest experience also had the highest reliability21 This should give confidence to all clinicians utilizing the lumbar-locked thorax rotation test in determining thoracic mobility deficits, though novice clinicians may need to use a more precise measure such as an inclinometer to quantify the available ROM when assessing patients who are demonstrating mobility near restricted ranges.
Though reliability was consistently high for all levels of experience, an interaction effect between rater and category in left passive rotation was found indicating that there was a distinction between raters of differing experience levels when rating left passive rotation only. The mean ROM for participants in the Restricted category was 34.33 (+/- 5.00) for rater C, while the mean ROM for participants in the Restricted category was 43.85 (+/-9.7) for rater A. This interaction effect was not present in any other measure, and as such, the cause is not well-understood. More research is needed to determine the source of this effect and its implications for clinicians. Additionally, future research should investigate the cause of active physiological deficits in thoracic rotation compared to passive physiological deficits as well as determine appropriate interventions for the respective deficit.
Impairments in mobility and neuromuscular control of the thorax have significant implications for athletes across many sports as well as for clinicians treating a multitude of pathologies in the upper quarter and spine. Therefore, it is important for clinicians to have an expedient method to assess for mobility or neuromuscular loss in the thoracic region. If clinicians can quickly and reliably identify a mobility restriction in a patient’s thoracic region, then they may accurately and efficiently determine the need for an intervention. Additionally, a field expedient test for thoracic mobility deficits may be better utilized in the athletic population during sideline assessments, pre-participation exams, and injury risk assessments due to its timeliness and efficiency. Finally, utilizing a visual estimation of thoracic rotation during pre-treatment and post-treatment assessments may allow the therapist to quickly determine the effectiveness of the intervention within the same day.
Limitations
As with all studies, some limitations should be acknowledged. First, the sample recruited for this study does not reflect the population to whom these techniques are often applied. This sample was relatively young, with a mean age of 27 years-old, and no subject was experiencing musculoskeletal pain. Although this specific population demographic maximizes homogeneity, the results may not be generalizable to other age groups and or to individuals in current pain. Second, specific information regarding the subjects’ activity levels, sport participation, and hand dominance were not collected. Doing so may have provided insight into observed asymmetries in thoracic mobility. Thirdly, scapulothoracic joint mobility was not measured or controlled for in this study with positional or active stabilization of the scapula which could have led to participant compensation during the test motion such as excessive scapular retraction in place of spinal rotation. Additionally, this study did not control for learning effects as the same subjects participated in both sessions that occurred one week apart; however, to control variability, subjects were tested by raters in a random order at both sessions. Further, to reduce variability in technique, all research assistants completed a hands-on one-hour training session facilitated and supervised by the expert rater. Research assistants who were involved in measuring thoracic rotation ROM using the digital inclinometers performed a palpation and measurement skills check-off and were obtained approval from the expert rater (KW). Finally, this study only utilized three testers, one representing each experience level from student to resident to expert, and all testers were graduates from the same physical therapy program where the quadruped lumbar-lumbar thorax rotation test is taught within the program. Due to these therapists being similarly trained, the results may not be representative of all physical therapists.
CONCLUSION
Visual estimation of thorax rotation ROM using the quadruped lumbar-locked position is a reliable and valid method in determining normal mobility as well as active and passive physiological deficits of thoracic rotation. Novice and expert clinicians can confidently perform this method to test for rotational mobility deficits in the thorax to expedite the examination and test-retest process.
CONFLICT OF INTEREST
The authors report no conflict of interest.
ACKNOWLEDGEMENTS
The authors of this study would like to thank Dr. Suzanne Leach and the University of Evansville Doctor of Physical Students Parker Rose, Kourtney West, Kyle Patton, Lauren Rennie, Jamie Vance, and McKenzie Goebel for their assistance with the study organization and data collection.