The anterior cruciate ligament (ACL) is a crucial structure of the knee joint that serves multiple vital functions, including resistance against anterior tibial translation, tibial internal-external rotation, and varus-valgus angulation.1 The importance of the ACL becomes especially evident in team ball sports, where non-contact ACL injuries are highly prevalent, especially in female athletes.2 These injuries often occur during dynamic jump landings or cutting maneuvers,3,4 where the ligament’s ability to resist the aforementioned loads is paramount for maintaining knee joint stability and function. Regardless of whether a surgical procedure or conservative approach is chosen, more than half the athletes sustaining an ACL injury will have developed osteoarthritis 10 – 20 years later, often resulting in chronic pain and disability.5,6 Therefore, preventing ACL injuries is essential to preserving the overall health and performance of athletes. However, since non-contact ACL tears occur rapidly, typically within 40 milliseconds after initial contact of the foot with the ground,3 sensory feedback strategies are too slow to correct the movement pattern after contact between the foot and the ground has been made. This suggests that feed-forward strategies aiming at adopting a safe posture at initial ground contact need to be targeted in injury prevention programs to mitigate the risk of ACL injury.
While real-time feedback solutions on joint biomechanics to facilitate motor learning have been proven successful in, e.g., gait retraining studies,7 the highly dynamic nature of landing and cutting tasks makes real-time solutions unsuitable. Therefore, researchers are challenged with developing solutions to provide feedback shortly after the completion of the movement. A systematic review and meta-analysis8 investigating the effects of augmented feedback on jump landing technique found positive effects on sagittal plane hip and knee kinematics and vertical ground reaction forces (GRF). However, little effect was observed on frontal plane biomechanics, which are crucial for reducing the magnitude of the peak external knee abduction moment (pKAM). Previous research strongly suggests that pKAM and the resulting knee valgus are main components of the injury mechanism.3,4,9,10 While a large amount of feedback interventions have focused on drop vertical jumps,8,11 this task might lack external validity and might therefore be unsuitable as a screening task for females participating in team ball sports.12 Hence, adequately designed studies investigating the immediate effect of augmented feedback on team ball sport-specific tasks are lacking. Further, while previous work has mainly focused on a single a priori selected variable for feedback, an individualized approach with the feedback variable tailored to an individual’s technique might improve the outcome of feedback interventions.
Therefore, the primary purpose of this study was to assess the instant effect of individualized augmented technique feedback and instructions on technique and pKAM during a handball-specific sidestep cut. It was hypothesized that highly trained players are able to adapt their technique after a combination of visual and verbal expert feedback and internally- and externally directed verbal instructions. Furthermore, since injury prevention programs usually report group means, thereby potentially concealing meaningful individual responses,13 the relative shares at which the feedback-instruction combinations translated to technique improvements and pKAM reductions were determined. The secondary purpose of the study was to determine the effects of the feedback-instruction combinations on the individual pKAM components, i.e., the resultant GRF and its frontal plane moment arm to the knee joint center. It was hypothesized that feedback aiming at improved foot strike angles or reduced vertical impact velocities reduces GRF magnitudes while feedback aiming at a reduction in knee valgus motion reduces the GRF moment arm to the knee joint center.
MATERIALS AND METHODS
Subjects
A total of forty-eight female high-level handball players were recruited. All played in the first, second or third Norwegian division. Prior to the commencement of the study, all players confirmed that they were free from any injuries or pain. Informed written consent was obtained from all players, and the study protocol received approval from the University Ethics Committee.
Testing
Each player was outfitted with a full-body marker set of 82 retro-reflective markers. The marker data were acquired using a system comprising 23 infrared cameras (Qualisys, Gothenburg, Sweden, 200 Hz). Additionally, GRF data were recorded using two floor-embedded force platforms (AMTI, Watertown, MA, USA; 600 x 1200 mm, 1000 Hz).
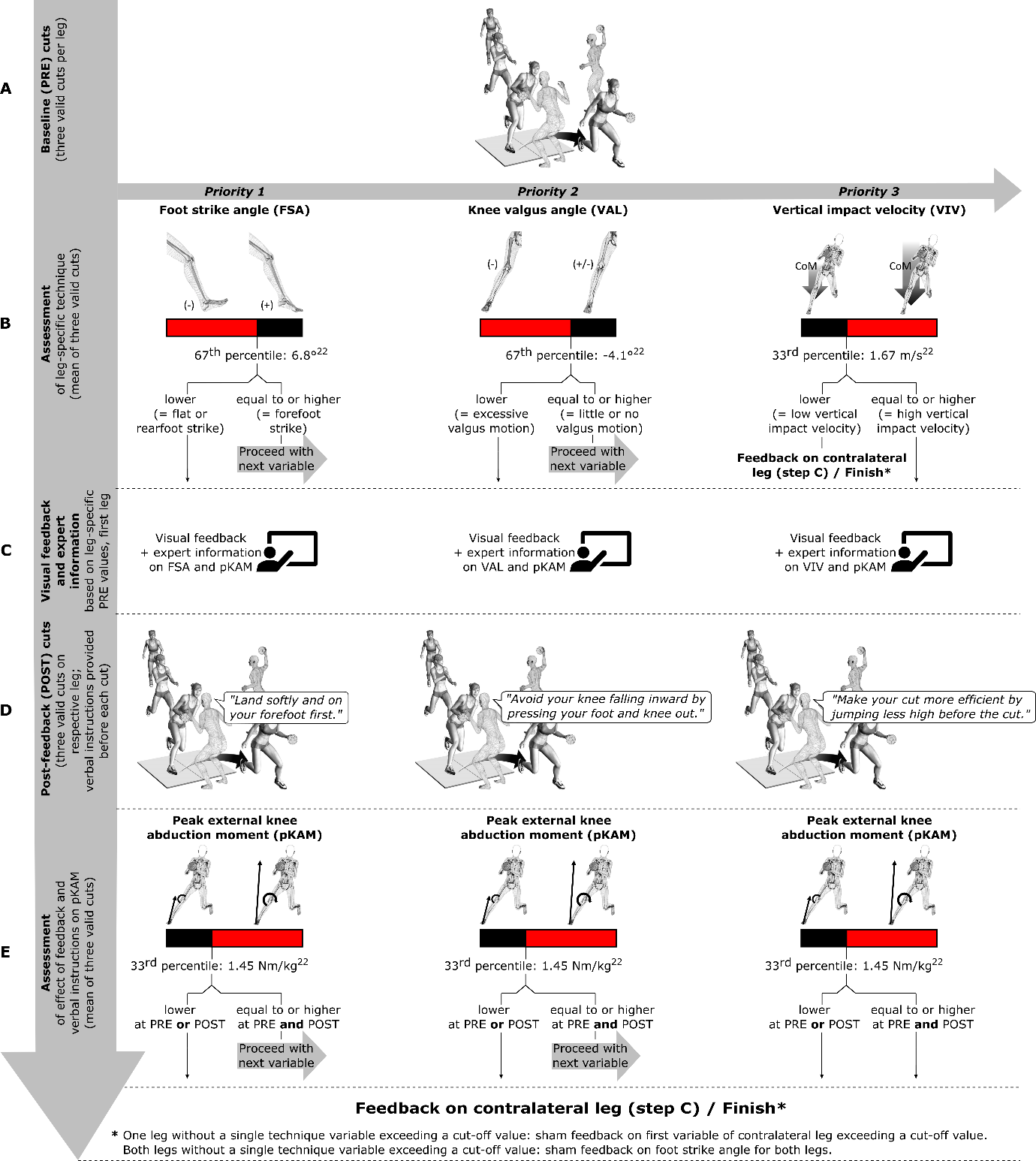
The players underwent a standardized warm-up and familiarization period. Subsequently, the players accelerated over a distance of six meters and approached the force platforms at an approximate angle of 35° to the longitudinal axis of the runway. The players received a pass from an experienced handball player during the penultimate step and subsequently executed a handball-specific sidestep cutting maneuver to pass a static human defender (Figure 1). Each player performed three valid cuts on each leg, which served as their individual baseline (PRE).

Following the completion of the PRE cuts, the players received personalized feedback regarding their individual pKAM and cutting technique for each leg (see Variable selection and feedback structure).
Feedback Component and Data Processing
The feedback component in this study was implemented using a custom MATLAB application (R2021b, The Mathworks Inc., Natick, Massachusetts, USA).14 The Automatic Identification of Markers (AIM) and Project Automation Framework (PAF) features, integrated into Qualisys Track Manager, were employed for automatic export of marker trajectories and GRF after each recorded trial. Concurrently, the MATLAB application continuously scanned the designated folder in the background to immediately process any newly recorded trial and plot results.
The joint centers of the ankle and knee were determined as the midpoint between the malleoli and epicondyle markers, respectively. The hip joint center was determined using the methodology described by Harrington et al.15 Segmental inertial properties were calculated based on regression equations from de Leva.16 The stance phase was defined as the period during which the unfiltered vertical GRF exceeded 30 N. All marker trajectories and GRF were filtered using a fourth-order low-pass Butterworth filter with a cut-off frequency of 20 Hz.17,18
To ensure the exclusion of invalid trials, a function was implemented to verify the accurate positioning of the foot within the boundaries of the force platform. After performing automated inverse dynamics calculations,19 pKAM normalized to body mass within the first 60 milliseconds of stance and technique variables at initial ground contact were computed. Following all calculations, essential kinematic and kinetic data were plotted and visible to the principal investigator to ensure data validity. The calculation and plotting of the results were completed within three seconds after each recording.
Variable Selection and Feedback Structure
Technique variables, i.e., foot strike angle (FSA), knee valgus angle (VAL), and vertical impact velocity of the center of mass (VIV), were chosen based on their established association with pKAM in female handball players.20,21 Cut-off values were set conservatively using a previously collected dataset.22 (Figure 1) Those cut-off values were:
-
Mean FSA ≤ 6.8° (67th percentile in previously collected dataset; a negative angle corresponds to a rearfoot strike),
-
Mean VAL ≤ -4.1° (67th percentile in previously collected dataset; a negative value corresponds to an increase in knee valgus at initial ground contact relative to the standing reference trial), and
-
Mean VIV ≥ 1.67 m/s (33rd percentile in previously collected dataset; a higher value corresponds to an increased vertical impact velocity of the center of mass).
As high within-player differences in pKAM and technique were evident during pilot testing between cuts performed with the left and right leg, feedback was provided leg-specific. Players received feedback on the first variable in the hierarchical order of 1) FSA, 2) VAL, and 3) VIV that exhibited values exceeding its cut-off. FSA served as the primary feedback variable due to its strong association with ACL injury and pKAM in various sports4,20,23–26 and its association with performance.27 Knee valgus angle served as the second priority despite its established association with pKAM and ACL injury4,20,26,28 due to its absent relationship with performance.27 While longer airtime might make the cuts less efficient, some athletes could rely on that technique to better execute a fake, however, sufficient data on this variable’s relationship with performance are lacking. Therefore, VIV feedback was the lowest priority in the feedback hierarchy (Figures 1 – 3).
Applying the same approach as for technique variables, a mean pKAM cut-off value of 1.45 Nm/kg was determined. This, along with the number of technique variables surpassing cut-off values at PRE, defined the maximum number of feedback cycles (see Communication to Players and Post-feedback Testing).
Communication to Players and Post-feedback Testing
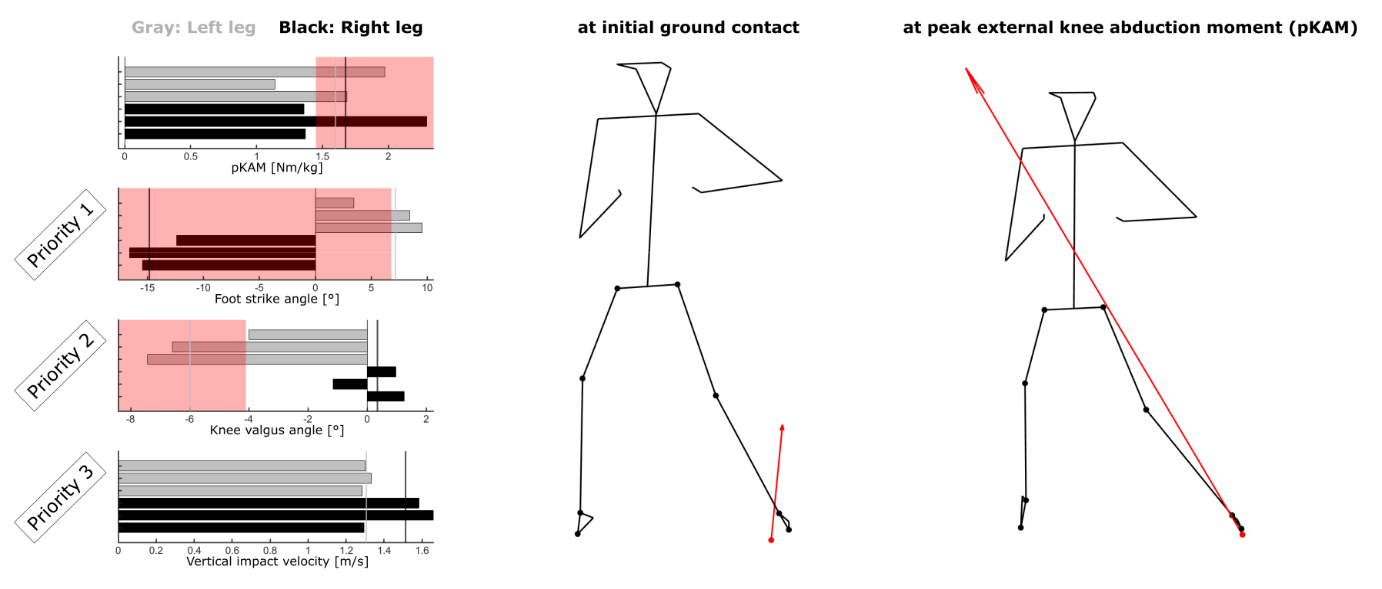
Players received instant visual feedback through bar graphs displaying the magnitude of pKAM and technique variables, along with stick figure representations of their movements including the GRF vector (Figure 2), displayed on a 65-inch screen. All players received standardized information on knee abduction moments and feedback (Table 1) on the first technique variable in the hierarchy exceeding a cut-off value. Subsequently, players performed three post-feedback (POST) cuts. Verbal instructions combining internally- and externally directed foci of attention were provided by the static human defender for each technique variable before each POST cut to guide technique modifications (Figure 1 and Table 1). Due to the previously reported relationship between approach speed and pKAM (20), a function in the custom MATLAB application rendered all POST trials performed with less than 90% of the mean PRE approach speed invalid. Following the POST cuts, outcomes were discussed. If pKAM was ≥ 1.45 Nm/kg at PRE and POST, and more than one technique variable exceeded its cut-off value at PRE, feedback on the next technique variable in the hierarchy exceeding its cut-off at PRE was provided. If PRE pKAM was < 1.45 Nm/kg or POST pKAM fell below that cut-off, or if only one technique variable exceeded its cut-off at PRE, the focus shifted to the other leg, and the same procedure consisting of PRE information and feedback as well as three POST cuts with verbal instructions was followed. For legs with no technique variable in excess of a cut-off value, sham feedback was provided on the first technique variable of the contralateral leg exceeding the cut-off. If no technique variable exceeded a cut-off in either leg, sham FSA feedback was provided for both legs (Figure 1). Hence, feedback was offered to all players after each leg. As the present study was an initial step in a comprehensive intervention study, this choice warranted uniform conditions for both intervention and control groups at the start of the program. Nevertheless, potential effects of sham feedback were disregarded in the analysis.
_cuts_per_leg.png)
Statistical analyses
POST values for technique variables (FSA, VAL, and VIV) and pKAM were compared to their respective PRE values. Additionally, to better understand the mechanisms through which feedback affects pKAM, the resultant GRF at pKAM and its frontal plane moment arm to the knee joint center were compared between PRE and POST.
Data normality was assessed, and Student t-tests and Wilcoxon signed-rank tests were performed for normally and non-normally distributed data, respectively. Effect sizes were calculated using Cohen’s d (for normally distributed data) and the rank biserial correlation coefficient, rrb (for non-normally distributed data). Significance was set at α = .05, and all statistical analyses were performed with JASP (Version 0.16.3, University of Amsterdam, Amsterdam, The Netherlands).
RESULTS
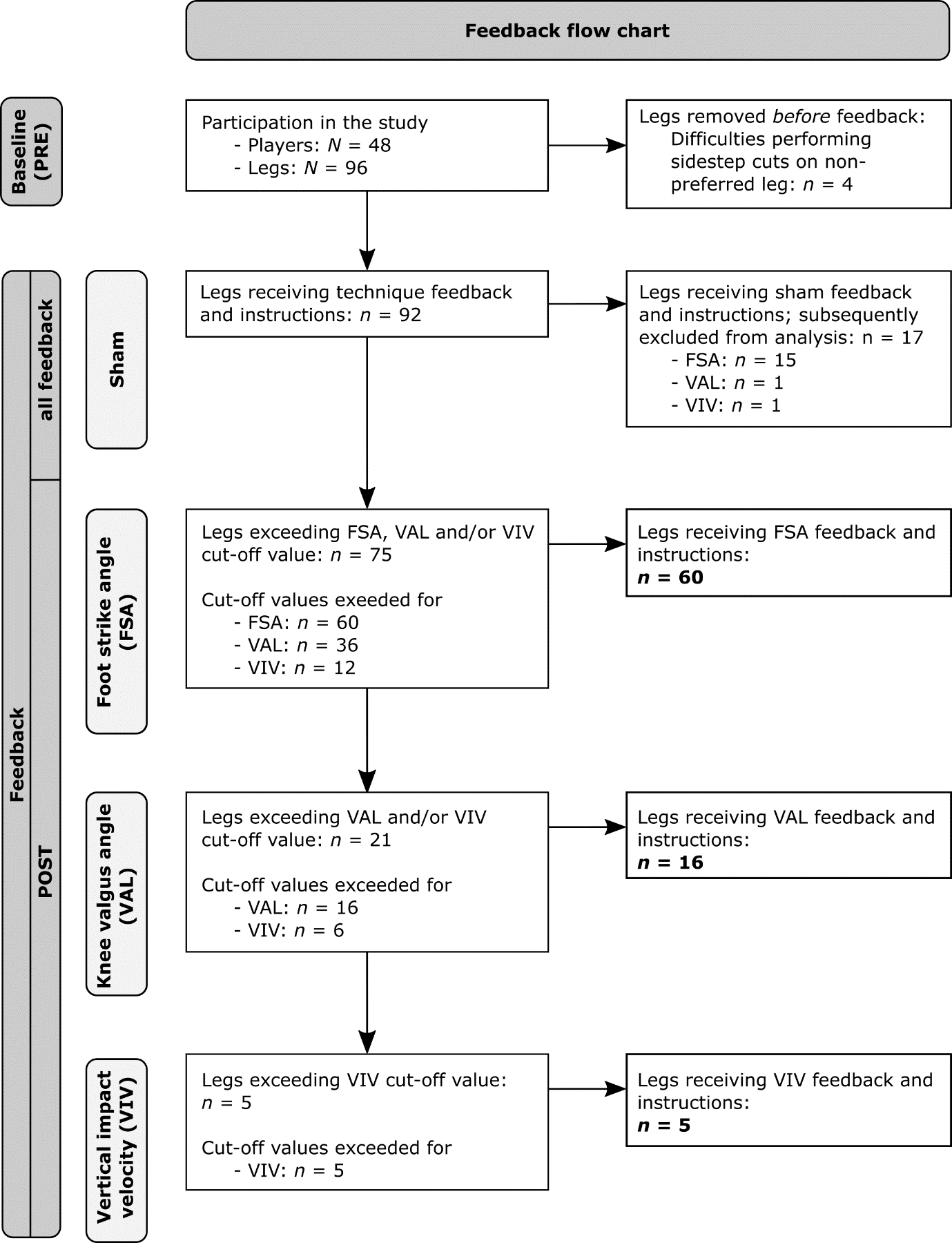
Forty-eight female high-level handball players (mean ± SD: 16.7 ± 0.9 years, height: 1.72 ± 0.06 m, weight: 68.7 ± 8.9 kg) voluntarily participated in this study. The players reported their weekly handball training, strength training, and active game minutes as 480 ± 121 minutes, 216 ± 65 minutes, and 42 ± 23 minutes, respectively. From the initial sample of 96 legs (48 players), four legs were excluded due to four players having difficulties performing sidestep cuts on the non-preferred leg. As a result, a final sample of 92 legs was considered for analysis. Among this refined sample, sham feedback was administered on 17 occasions, with sham FSA feedback being provided in 15 instances, and sham VAL and sham VIV feedback each provided once. These instances of sham feedback were subsequently excluded from the analysis. The final analysis comprised 75 legs (Figure 3).

Feedback distribution
In total, 29 legs exhibited pKAM ≥ 1.45 Nm/kg at PRE. Out of these 29 legs, 14 legs also displayed multiple technique variables exceeding their cut-off, thus rendering them eligible for multiple cycles of feedback. Of these 14 legs, eight legs went through a single cycle of feedback before falling below the pKAM cut-off of 1.45 Nm/kg, while six legs went through two cycles of feedback. No leg went through all three cycles of feedback.
FSA feedback was given a total of 60 times. While 36 legs were eligible for VAL feedback and 12 legs were eligible for VIV feedback (Figure 3), VAL and VIV feedback were provided only 16 and five times, respectively, due to the hierarchical feedback structure (Figure 1). In short, the 20 instances in which VAL feedback was not provided can be explained by 11 cases in which these legs also exhibited poor foot strike angles (≤ 6.8°) but low pKAM (< 1.45 Nm/kg) at PRE so that only feedback on the foot strike angle was provided. In the remaining nine cases, the legs also exhibited poor foot strike angles (≤ 6.8°) combined with high pKAM (≥ 1.45 Nm/kg) at PRE while successfully decreasing their pKAM below 1.45 Nm/kg at POST so that no feedback beyond the one targeting the foot strike angle was provided.
Feedback response
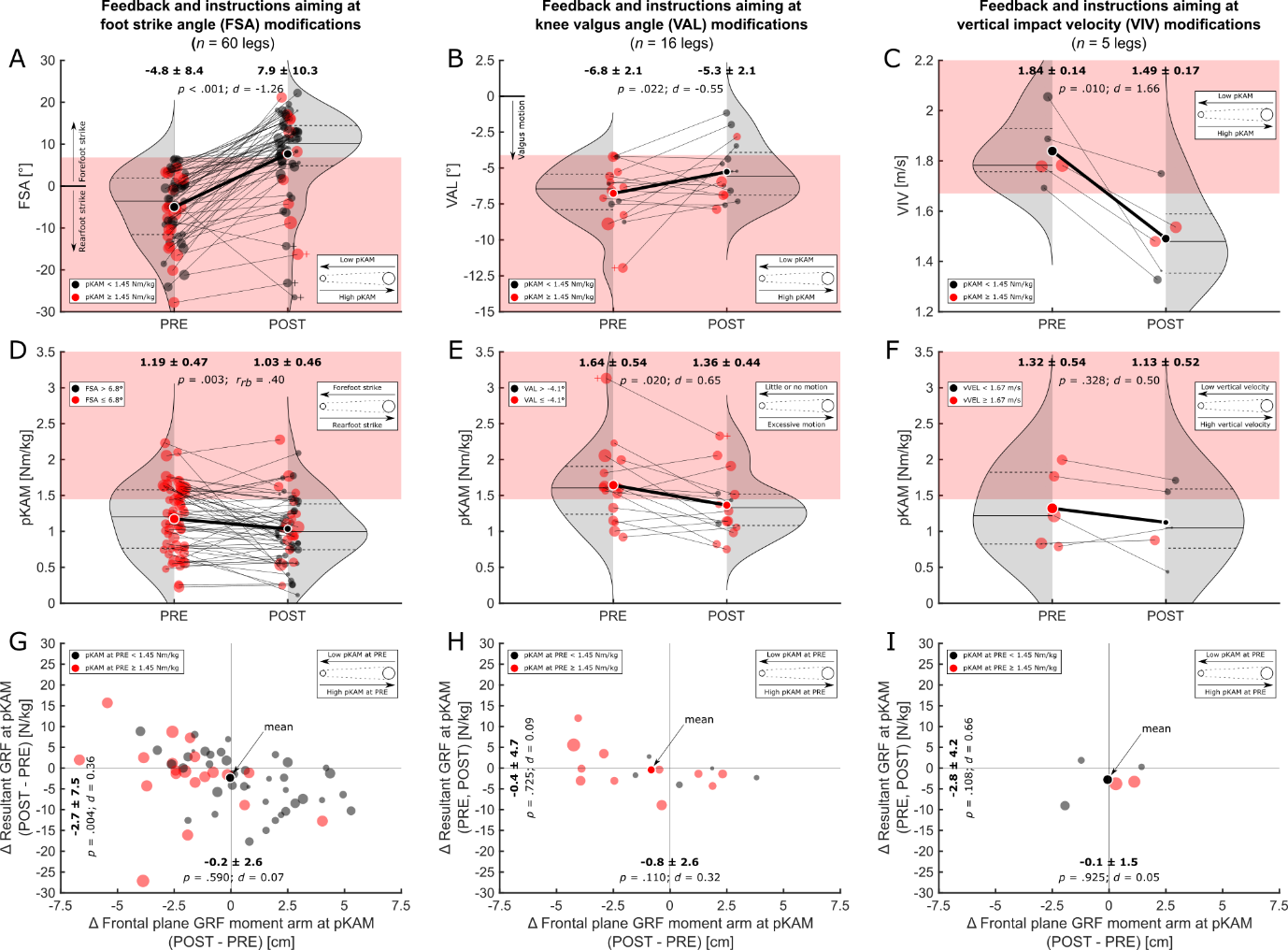
FSA feedback resulted in an improvement in foot strike angle of 12.7° (95% CI [10.5, inf]) on average (PRE vs. POST: -4.8 ± 8.4° vs. 7.9 ± 10.3°; p < 0.001, d = -1.26). Out of 60 legs, 41 legs (68.3%) showed improvements above the cut-off value of 6.8° at POST (Figure 4A). Importantly, FSA feedback resulted in a median reduction in pKAM of 0.14 Nm/kg (95% CI for Hodges-Lehmann Estimate [0.04, 0.24]) or 13.4% on average (PRE vs. POST: 1.19 ± 0.47 vs. 1.03 ± 0.46; p = 0.003, rrb = .40). Among the 20 legs with pKAM ≥ 1.45 Nm/kg at PRE, 14 legs (70%) improved to values below the cut-off at POST (Figure 4D). The resultant GRF at pKAM decreased by 2.7 N/kg (95% CI [1.0, inf]) or 13.8% on average (PRE vs. POST: 19.6 ± 6.2 N/kg vs. 16.9 ± 6.2; p = 0.004, d = 0.36). Changes in the frontal plane GRF moment arm to the knee joint center at pKAM (-0.2 cm, 95% CI [-0.9, 0.5], or -3.0%) were not statistically significantly different (PRE vs. POST: 6.6 ± 2.9 cm vs. 6.4 ± 2.7 cm; p = 0.590, d = 0.07) (Figure 4G).

VAL feedback resulted in a reduction in knee valgus angle of 1.5° (95% CI [0.3, inf]) on average (PRE vs. POST: -6.8 ± 2.1° vs. -5.3 ± 2.1°; p = 0.022, d = -0.55). Among the 16 legs, four legs (25%) successfully improved beyond the cut-off of -4.1° after VAL feedback (Figure 4B). Importantly, VAL feedback significantly reduced pKAM by 0.28 Nm/kg (95% CI [0.05, 0.51]) or 17.1% on average (PRE vs. POST: 1.64 ± 0.54 vs. 1.36 ± 0.44; p = 0.020, d = 0.65). Among the 11 legs with PRE pKAM ≥ 1.45 Nm/kg, six legs (54.5%) improved to values below the cut-off at POST (Figure 4E). Changes in the resultant GRF at pKAM (-0.43 N/kg, 95% CI [-3.0, 2.1], or -2.3%; PRE vs. POST: 17.4 ± 5.4 N/kg vs. 17.0 ± 7.0; p = 0.725, d = 0.09) and the frontal plane GRF moment arm to the knee joint center at pKAM (-0.8 cm, 95% CI [-inf, 0.3], or -8.2%; PRE vs. POST: 9.7 ± 1.2 cm vs. 8.9 ± 2.9 cm; p = 0.110, d = 0.32) were not statistically significantly different (Figure 4H).
VIV feedback significantly reduced the vertical impact velocity by 0.35 m/s (95% CI [0.15, inf]) or 19.0% on average (PRE vs. POST: 1.84 ± 0.14 m/s vs. 1.49 ± 0.17 m/s; p = 0.010, d = 1.66). Out of five legs, four legs (80%) achieved values below the cut-off of 1.67 m/s at POST (Figure 4C). Changes in pKAM (-0.20 Nm/kg, 95% CI [-0.68, 0.29], or -14.4%; PRE vs. POST: 1.32 ± 0.54 vs. 1.13 ± 0.52; p = 0.328, d = 0.50) were not statistically significantly different. None of the two legs with pKAM ≥ 1.45 Nm/kg at PRE improved to values below the cut-off at POST (Figure 4F). Changes in the resultant GRF at pKAM (-2.8 N/kg, 95% CI [-inf, 1.3], or -17.3%; PRE vs. POST: 16.2 ± 4.7 N/kg vs. 13.4 ± 4.2; p = 0.108, d = 0.66) and the frontal plane GRF moment arm to the knee joint center at pKAM (-0.1 cm, 95% CI [-1.9, 1.8], or -1.2%; PRE vs. POST: 8.4 ± 2.2 cm vs. 8.3 ± 2.7 cm; p = 0.925, d = 0.05) were not statistically significantly different (Figure 4I).
DISCUSSION
The primary objective of this study was to investigate the effect of individualized augmented feedback and instructions on cutting technique and pKAM during handball-specific sidestep cutting in female athletes. On average, all three targeted technique variables improved with medium to very strong effect sizes. Interestingly, despite large variations in both sample size and relative adherence to the instructions, all three targeted technique modifications yielded similar relative reductions in pKAM with medium effect sizes. This finding supports the high potential of feedback interventions addressing knee joint loading and suggests that even minor technique adjustments, as observed following VAL feedback, can lead to substantial reductions in pKAM. However, it is important to acknowledge the high inter-individual differences in technique and pKAM that persisted even after feedback and instructions. Adherence to the provided instructions did not consistently lead to reductions in pKAM, highlighting the complex nature of technique modifications and individual responses to feedback.
In scenarios where multiple variables exceeded their predefined cut-off value, the selection of the feedback variable was contingent upon PRE pKAM magnitudes and the variables’ performance-related relevance. Foot strike angle served as the primary feedback variable due to its strong association with ACL injury and pKAM in various sports4,20,23–26 and its positive effect on performance.27 Knee valgus angle was believed to be more challenging to modify instantaneously and seems to have no relationship with performance.27 It was therefore selected as the second priority for feedback despite its established association with pKAM and ACL injury.4,20,26,28 Spending more time airborne could reduce the efficiency of cuts, yet it might enable players to more effectively deceive or misdirect opponents. Therefore, VIV feedback was the last priority in the feedback hierarchy. The authors believe that reducing the vertical impact velocity might hold a distinct advantage over previously proposed variables such as the knee flexion angle or range of motion that are common targets for technique modifications.29–31 Increasing the knee flexion range of motion aims at dragging out the deceleration period to reduce the peak vertical GRF. By doing so, ground contact times might increase, and performance deteriorate.27 Lower vertical impact velocities reduce the need for high vertically-directed decelerating forces, thereby reducing the need for prolonged deceleration phases and increased contact times.
Knee valgus angle and vertical impact velocity have been previously shown to be consistently increased in handball players showing high pKAM across handball-specific sidestep cuts of varying complexity.21 The authors of that study therefore suggested these variables might be part of the players’ inherent movement strategy. In that same dataset, the same task complexity used in the present study was the only one that, on average, provoked a rearfoot strike and, additionally, produced the highest pKAM across differently complex cutting maneuvers. Other technique variables such as the width of the cut, cutting angle, and approach speed have been previously shown to explain a large proportion of the variance in pKAM.20 However, they did not differ between players showing consistently high and low pKAM across different sidestep cut complexities and are therefore potentially not part of a player’s automated motor program used across different game scenarios. Furthermore, changes to these variables might have detrimental effects on performance27 and might therefore be unattractive to players and coaches. Therefore, these variables were not part of the feedback variables of the present study. It is interesting to note that the foot strike angle (“toe landing”) and knee valgus angle were also significant predictors of pKAM in the study by Kristianslund and colleagues.20
Employing cut-off values as criteria for assessing technique improvements following feedback yielded improvements in 68.3%, 25%, and 80% of the cases following FSA, VAL, and VIV feedback, respectively. However, even slight improvements in technique might have substantial effects on pKAM as evident with VAL feedback. Using the cut-off values to assess technique enhancements resulted in the lowest percentage of improvement in that group, however, it demonstrated the highest pKAM at PRE and the highest relative (-17.1%) and absolute reductions in pKAM (-0.28 Nm/kg) at POST, highlighting the relationship between knee valgus angle and pKAM and the potential of the variable in reducing frontal plane knee joint loading. Looking at average changes in technique from PRE to POST and neglecting cut-off values, the vast majority of players were able to improve their technique. However, the response to technique modifications as measured by pKAM is highly individual and reductions in pKAM were not always achieved when players adhered to feedback. This highlights the complex interplay between feedback and technique variables and the potential to change whole-body dynamics. Yet, it seems that the selected variables show great potential in reducing pKAM, and the effect might be magnified when used in combination. Considering that female players between the age of 15 and 19 have the highest incidence rate of ACL injury,32 coaches should stress sound technique early in the playing career.
Only a limited number of studies have previously aimed at reducing pKAM following feedback on sidestep cutting technique.33,34 Benjaminse et al.33 investigated the immediate effects of verbal instructions compared to visual feedback on kinematics and kinetics at peak frontal plane knee joint moment during unanticipated sidestep cutting in males and females while also investigating the retention of the new technique over time. While the authors found that males are more responsive to visual feedback and able to retain improvements in technique over a four-week period, the authors concluded that females might prefer a combination of visual and verbal feedback, as used in the present study. Interestingly, frontal plane knee joint moments were unresponsive to either feedback strategy in both males and females. The results regarding the frontal plane knee joint loading are in contrast to those by Dempsey et al.34 who used a six-week technique modification program transitioning from closed- to open-skills practice in male team sport athletes. In their study, athletes received a combination of oral and visual feedback twice a week including reference videos of athletes demonstrating the desired sidestep cutting technique to bring the stance leg closer to the midline of the body while keeping the torso upright and facing in the direction of travel. Using this approach, the authors successfully decreased frontal plane knee joint moments in both planned and unplanned sidestep cuts.34
More research has focused on feedback interventions for jumping or landing tasks, with two systematic reviews shedding light on the topic.8,35 Armitano et al.35 and Neilson et al.8 synthesized the findings of these studies and reported that feedback can lead to reductions in vertical GRF and increases in knee flexion angles during various jump landing tasks. Furthermore, it has been observed that learning acquired through feedback can transfer to similar tasks.35 However, the transfer of newly acquired motor skills to sidestep cutting tasks has yielded conflicting results in the literature. In support of providing feedback specific to the movement that requires technique optimization, a study utilizing a combination of oral and video feedback found no transfer of learning from drop jumps to sidestep cutting tasks.36 This suggests that feedback should be tailored to the specific movement pattern in order to facilitate effective skill transfer and improvement which is further highlighted by poor correlations between pKAM in drop jumps and sidestep cuts.37 In contrast, another study demonstrated that improved jump landing technique could be transferred to sidestep cutting when incorporating an external attentional focus and self-controlled feedback.29 Nevertheless, it is important to acknowledge that these improvements related to increases in the range of motion of the knee flexion angle, which could potentially impact performance negatively.27
The secondary objective of the current study was to explore the underlying mechanisms responsible for changes in pKAM. FSA feedback significantly reduced the magnitude of the resultant GRF at pKAM, potentially due to the ankle plantar flexors acting as an additional damping element.28 Differences in the resultant GRF and the frontal plane moment arm to the knee joint center from PRE to POST were not statistically significant after VAL and VIV feedback. However, the medium effect size for changes in the resultant GRF after VIV feedback indicates potentially meaningful improvements. Interestingly, in total, there were only three instances where both the resultant GRF and frontal plane moment arm increased simultaneously, indicating that the feedback interventions generally resulted in positive changes in at least one component of pKAM (Figure 4G–I). However, it is important to note that the responsible mechanisms for pKAM changes showed high inter-individual variability. Future research might investigate whether the optimal feedback selection can be determined based on the main factor in driving pKAM alone, i.e., the resultant GRF or its frontal plane moment arm to the knee joint center.
Incorporating immediate feedback and outcome discussions with players within long-term interventions might hold potential for enhancing player motivation and adherence. For researchers, the implementation of immediate feedback and insights into the present state of the player serve as critical tools to verify the effectiveness of prescribed interventions, allowing for adjustments to be made in a timely manner to optimize outcomes. Moreover, the reliance on technology becomes indispensable in the identification of players at risk and the differentiation between kinematic and kinetic improvements. Feedback based on visual assessments might fall short in inducing changes in kinetics unless given by experts,38 underlining the necessity for advanced technological solutions. These solutions, however, must be user-friendly and efficient to accommodate the practical constraints of time, manpower, and equipment associated with the present approach. Transitioning from lab-based setups to portable and cost-effective technological systems that enable on-field assessments would enhance the practical applicability of feedback interventions. This would democratize access to advanced training aids across different levels of sport and foster more evidence-based approaches to injury prevention and performance optimization, ultimately bridging the gap between research findings and their application in real-world sports scenarios.
Although the overall results of the study demonstrate the positive effects of feedback interventions, it is important to acknowledge certain limitations. Firstly, the hierarchical structure used for selecting feedback variables led to a reduced number of players receiving comprehensive feedback across all variables. The cut-off values utilized to determine the need for feedback were selected arbitrarily, drawing from an existing dataset.22 It is important to clarify that these cut-offs were not intended to indicate injury risk levels, but rather, were conservatively chosen benchmarks aimed at evaluating the practicability of technique adjustments. Furthermore, the hierarchical structure for variable selection primarily stemmed from the relevance of technique variables to cutting performance.27 Nevertheless, it is worth noting that performance predominantly revolved around ground contact times or time to complete a task, which may not be of highest importance in a maneuver aimed at successful opponent passage. Instead, a more pertinent performance metric might be the successful deception of the opponent into perceiving a contrary direction of movement. Secondly, although previous research39 demonstrated good to excellent within-session and fair to good between-session reliability with three trials of the task, the optimal number of trials required to establish a stable movement pattern after feedback remains unclear. Thirdly, the risk of sustaining an ankle injury when modifying the foot strike angle remains unknown. While a recent systematic review suggests that ankle plantar flexion might not play a crucial role in the occurrence of lateral ankle sprains,40 a combination of ankle plantar flexion and inversion strains the anterior tibiofibular ligament and calcaneofibular ligament more than inversion alone.41 Therefore, caution is necessary when transitioning to a new cutting technique, especially for players with a history of lateral ankle sprains. It is possible that these players should focus on landing on the forefoot only during the early impact absorption phase while having the foot firmly planted during the main part of the cut. Alternatively, these players might benefit from other technique modifications. Next, the study did not investigate the long-term retention of the newly adopted technique or its transfer to unanticipated sidestep cutting scenarios. Although the knee valgus motion and vertical impact velocity have been proposed as components of a player’s inherent movement strategy during handball-specific sidestep cuts with varying complexity,21 it remains unclear whether training designed to alter cutting technique in preplanned cuts automatically translates to complex unplanned cuts. Lastly, it is important to acknowledge that the diverse nature of feedback approaches (visual, verbal, self-guided, expert, etc.) and instructions (internally- or externally directed) was not specifically investigated in the present study. The selection and combination of these feedback modalities and instruction types potentially impact the outcomes, however, exploring these factors was beyond the scope of the current study.
To the authors’ knowledge, the current study represents a pioneering effort in the field as it is the first to employ augmented feedback immediately following a sport-specific task known for its high incidence of non-contact ACL injury4 using an individualized approach while also uncovering individual responses and mechanisms responsible for reductions in frontal plane knee joint loading. Future investigations should aim to examine the long-term retention of feedback effects and transferability to unanticipated sidestep cutting scenarios. Furthermore, possibilities for on-filed assessments should be explored. Additionally, further research is needed to compare the effectiveness of individualized feedback approaches to generic approaches in optimizing technique and performance outcomes. Understanding the sustainability and generalizability of feedback interventions in different contexts will provide valuable insights for sports practitioners, coaches, and researchers.
CONCLUSION
Individualized augmented feedback interventions show great potential in improving sidestep cutting technique instantly. Consequently, these improvements contribute to a 13.4% to 17.1% reduction in knee joint loading associated with ACL injury, while the adherence to the instructions and the underlying mechanism responsible for pKAM reductions vary between targeted technique variables and players. Future studies may explore possibilities for individualized on-field technique feedback using low-cost equipment.