
INTRODUCTION
Chronic injuries are common in long-distance runners and are often associated with muscle weakness and inability to run. Proximal Hamstring Tendinopathy (PHT) involves deep pain located in the ischial tuberosity region. Acute lesions commonly result from rapid acceleration and deceleration movements and are often associated with activities such as soccer, skiing, and field hockey. Chronic injuries usually have an insidious onset and pain worsens during sports activities and prolonged sitting.1 There is limited literature on the diagnosis and clinical management of PHT.2 Diagnosis can be challenging, as PHT is one of several potential sources of symptoms in this region. Regarding PHT, it is believed that tendon compression and shear force at its insertion at the ischial tuberosity during hip flexion/adduction is a key etiology.3 Extrinsic factors related to the etiology include training errors including excessively rapid increase in volume or intensity, accelerations or decelerations, changes in direction, training on slopes. Authors of several case reports suggest that these training errors would precede PHT, since during these trainings the tension and compression load on the tendon may be excessive at the insertion due to the hip flexion angle.4 During running the hamstrings perform eccentric deceleration of knee extension with maximal force at the end of swing phase. Energy storage in the late swing cycle is associated with increased hamstring loads. Increased hip or trunk flexion (climbing slopes or trunk forward) can increase the energy storage load on the proximal hamstring insertion.5
Cook and Purdam6 proposed the continuum model of tendon pathology, where diffuse increase in cellularity and ground substance (reactive tendinopathy) precedes focal areas of collagen disorganization and neurovascular ingrowth, with progression over time to address a degenerative tendinopathy morphology. According to Lempainen et al.7 samples of pathological proximal hamstring tendon tissue show increased cellularity, accumulation of ground substance, collagen disorganization and neurovascular ingrowth, similar to what is seen in other tendinopathies such as Achilles and patellar tendinopathy.
Regarding the diagnosis of PHT, pain in the region of the ischial tuberosity, well localized, which after a few minutes of activity improves and then worsens, confirms the typical behavior of tendon pain.8 During activities involving increased hip flexion (prolonged sitting, bending down), the onset of pain is frequent. The occurrence of pain during activities that do not involve energy storage or compression is infrequent. Stiffness may occur in the morning or when starting to move after prolonged rest. Regarding the differential diagnosis, multiple pathologies that can cause symptoms in the ischial region should be considered, such as pathologies of lumbar, hip, sacroiliac regions, as well as radiculopathy or sciatic nerve involvement. Sometimes PHT can coexist with these pathologies, which makes diagnosis and clinical management difficult. According to Cushman and Rho,9 it is presumed that overuse, poor lumbopelvic stability, and relatively weak hamstring musculature contribute to the development of PHT. Excessive movement of the sagittal lumbopelvic plane (i.e., anterior tilt and hip flexion) has been linked to hamstring injury by causing increased hamstring origin tightness.10 This reasoning may support the inclusion of trunk stabilization/strengthening exercises, which have been used in the therapeutic management of PHT.4 An elevated stride length can potentially amplify the tensile load on the proximal hamstring tendon, whereas an increase in running cadence leads to a reduction in stride length, hip flexion, and an increase in gluteal activity during the terminal swing. Although this intervention holds promise in lessening the tensile load on the hamstring, the application of running gait retraining remains unexplored in the treatment of PHT.11
Case reports have linked hamstring weakness to long-term symptoms in athletes with PHT.8,12 Other kinetic chain deficits have the potential to increase hamstring stress concentration of origin. Gluteus maximus atrophy in PHT may contribute to hamstring overload, while gluteus medius weakness has been associated with PHT as a consequence of increased hip adduction and/or contralateral pelvic drop during monopedal stance.4,13,14 Several authors have explored the management of those with PHT.15–18 However, concerning clinical management, published case reports predominantly concentrate on manual therapy and exercise programs centered around eccentric activity. Notably, these reports have overlooked the role of programmed tendon load adaptation, no taking in consideration the increase in hip flexion as a criterion for progression of tensile load on the tendon. The key to the management of all tendinopathies is progressive loading, performed within a pain monitoring framework, to reduce pain and restore function.8
The intervention proposed in this case report was based on the progression of the exercises by monitoring the response of the injured tendon to the load, (with the recording of VAS after the daily load test performed at the same time daily) supported by the study of Mascaró et al.19 regarding treatment of patellar and Achilles tendinopathy. For PHT, intervention based on load progression and assessment of functionality by means of validated scales has been recommended by authors such as Goom et al.8 At present, there is no clear guidance from the literature on PHT rehabilitation. Weight-bearing exercises for PHT have not been investigated in randomized controlled trials. Limited case series and case presentations have been published demonstrating improvements in pain and function with conservative treatment, including hamstring strengthening. The results of these studies cannot be generalized, due to sample size, different diagnostic methods, and the use of adjunctive interventions along with exercise.
The aim of this case report was to analyze the effectiveness of an exercise protocol with progression of tendon load in PHT in an amateur runner, by assessing pain and functional capacity.
CASE DESCRIPTION
The subject, a 30-year-old healthy male recreational runner who had actively participated in marathons and mid-distance races for the prior decade. Following a 10km race, an insidious onset of deep buttock pain in the right ischial tuberosity occurred without any traumatic incident. The pain was exacerbated during run training on sloped roads and prolonged sitting on hard surfaces, particularly while driving. Using the Visual Analog Scale (VAS), the subject rated the pain as 7/10, with 0 indicating no pain and 10 being the worst imaginable pain. The VAS scale, spanning from 0 to 10 on a 10 cm straight horizontal line, has been described as a reliable measure for assessing pain intensity in subjects with similar conditions.20 A higher score on the scale denotes greater pain intensity, and the test has demonstrated reliability in subjects with chronic musculoskeletal pain.
The subject denied any referred pain, numbness, tingling, weakness, bowel or bladder function changes, medication usage, recent or prior trauma, prior hamstring injury, or prior history of stress fractures. He reported previous treatment during two manual therapy sessions, femoral biceps and semitendinosus dry needling and four weeks of eccentric hamstring exercise (Nordic Hamstring Exercise) without any significant relief.
EXAMINATION
The subject’s signs and symptoms through his treatment course are reported in Table 1. Subject clinical and anthropometric data were collected. Pain and function were evaluated with the Victorian Institute of Sport Assessment-proximal hamstring tendons (VISA-H) questionnaire21 which is a valid and reliabile outcome measure for subjects with PHT (Cronbach α coefficient=0.84 95%CI 0.77-0.89; ICC for non-surgical subjects=0.92). The questionnaire consists of eight items. Pain and function are evaluated from items 1 to 6. Items 7 and 8 evaluate sporting activity. Questions 1 to 7 are scored from 0 to 10 while question 8 is scored from 0 to 30. The maximum possible score is 100 (an asymptomatic person would score 100, whereas the worst possible score is 0 points). The subject presented with a VISA-H score of 23.
Throughout the physical examination, no pain was elicited during concentric and resistance contractions. However, discomfort was observed during the eccentric contraction of the right hamstring muscle. Despite this, no weakness was detected in the muscle during the manual muscle testing, and the reported pain was localized to the right ischial tuberosity.
The Puranen-Orave test (PO), bent-knee stretch test (BK stretch) and supine plank test were positive, in that pain was exacerbated in the affected area. The PO is a valid and reliable test (specificity= p=0.82; 95%CI=0.68-0.92).15 It is a standing test that actively stretches the hamstrings muscles in a standing position with the hip flexed at about 90º and the knee is extended fully, and the foot is on a support at 90º. BK stretch test is a validity and reliability test (specificity= p=0.87; 95%CI=0.73-0.95).15 It is performed in the supine position. The hip and knee of the affected leg are in a maximally flexed position. The examiner slowly straightens the knee till its maximally extended. To evaluate the supine plank test the participant was asked to sit down with the hands on the ground behind the hips, fingers pointing backwards and arms straight.22 The subject must push down with the heels and lift the pelvis in the air, creating a straight line from shoulders to ankles. The subject was asked to lift the non-sympotamic leg off the ground (with knee extended).
The SLUMP test yielded negative results. This neurodynamic test involves a progressive series of maneuvers designed to increase tension in the sciatic nerve. While the SLUMP test is validated for subjects with lumbar disc herniation (sensitivity=0.84, CI=0.74-0.90; specificity=0.83, CI=0.73-0.90), its applicability to subjects with PHT has not been specified.23
Musculoskeletal ultrasound conducted in the medical provider’s office revealed notable findings. The left (symptomatic) tendon exhibited increased thickness, measuring up to 1.6 cm (normal range: 0.6-0.7 cm). Additionally, there were indications of hypoanechogenicity and significant intratendon neoangiogenesis, suggestive of severe tendinopathy in an active phase and of long-standing duration. In contrast, the right leg (non-symptomatic) demonstrated a tendon thickness ranging from 0.8 to 0.9 cm, characterized as discrete thickening with hypoanechogenicity and an absence of neoangiogenesis.
INTERVENTION
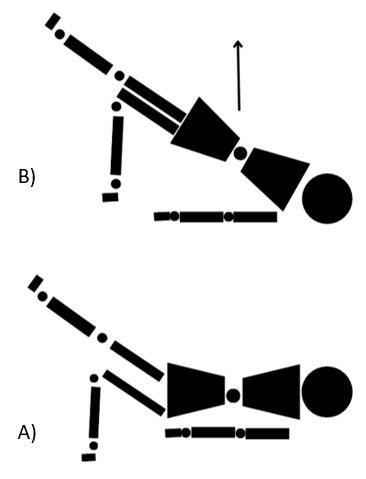
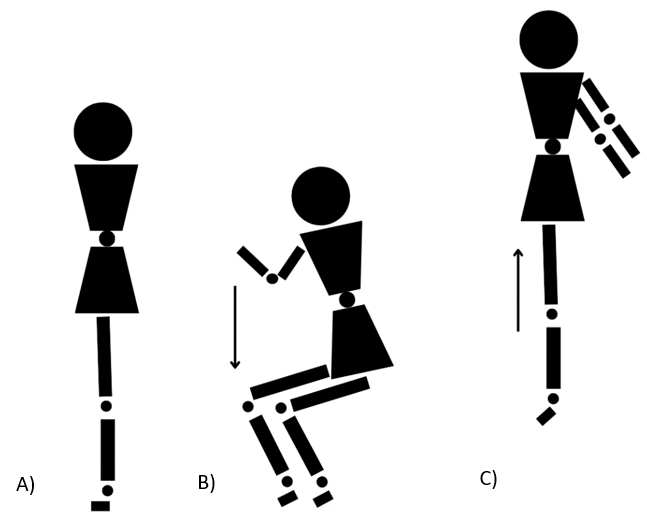
The intervention involved a progressive load exercise program structured into four phases. Advancement to the next phase was contingent upon the load test (Figure 1), registering ≤4 on the VAS, on two consecutive days. The evaluation was conducted consistently at the same hour each day and recorded.
.jpeg)
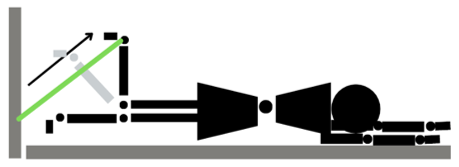
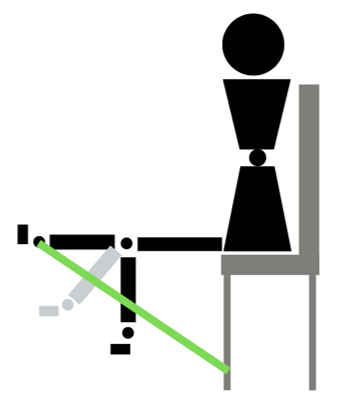
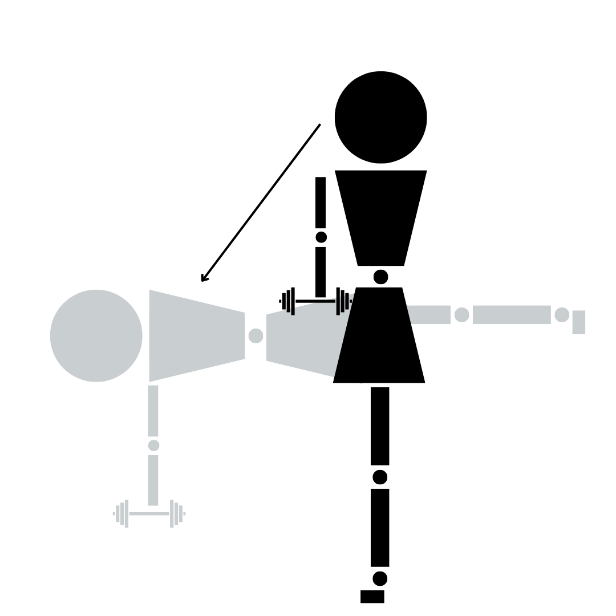
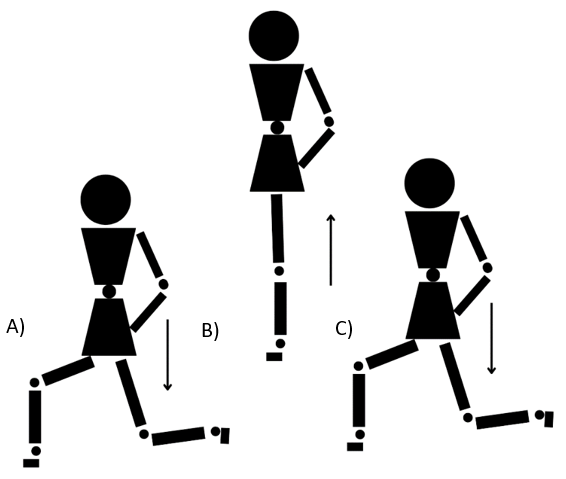
The exercise program implemented in this case study adhered to the regimen outlined by Goom et al8 for HT and the protocol detailed by Mascaró et al.19 which employs a safe load progression method to modify and enhance the structure of affected tendons in conditions like patellar and Achilles’ tendinopathy. Progression through the various phases was determined by the response to the exercise load on consecutive days rather than being dictated by specific time periods. The intervention lasted 12 weeks and measurements were taken at baseline (T1), at week 6 (T2) and at 12 weeks (T3) coinciding with the end of the intervention program. The exercises are described in Figures 2 to 7 and in Table 2.
_start_position__lying_on_the_back__one_leg_bent__and_the_other_leg_e.png)



_standing_position_(feet-shoulder_width_apart)_b)_ben.png)
_start_position__legs_split_with_one_leg_in_front_of_the_bod.png)
For return to running, the subject followed the protocol suggested by the authors, which is described in Table 3. He was instructed to run on alternate days and to remain at least two days at each level. If no pain was described, he could move on to the next level. Running intensity at all levels was at a gentle pace (65% of maximum speed).
OUTCOMES
After the first week of initiating the load exercise program, the subject observed a decrease in pain, enabling progression to the second phase, incorporating exercises with a higher tendon load. By the sixth week, his pain had reduced to 5/10. By week 9, the subject started combining the load exercise program with return to running program (Table 3). At the conclusion of the 12-week intervention, the pain had diminished to 1/10. Currently, the subject persists in performing the load exercise program and refrains from sloped running training. He reports training at the previous injury intensity and distance without experiencing any pain.
On physical examination (Table 1), the subject exhibited a notable reduction in tenderness to palpation of the proximal hamstring tendon, diminished pain with the mentioned provocative maneuvers, and reported a decreased intensity of pain during rest. At the nine-week mark after the initial examination, he commenced run training, and his VISA-H score improved. The subject maintained the same load exercise program throughout this period.
Six weeks after the commencement of the progressive load exercise program, ultrasound imaging was repeated in the medical providers office. The examination revealed that the left tendon showed no thickening and measured within the normal range (0.6-0.7 cm). This provided evidence of improvement in tissue quality.
DISCUSSION
In this case, the training progression for PHT tendon injury, supported by Goom et al.,8 was beneficial, emphasizing a gradual increase in hip flexion position from less to more. The progression suggested by Mascaró et al.19 for patellar and Achilles tendinopathy, based on isometric, concentric/eccentric and energy storage exercise was beneficial for this subject.
The observed improvement in this subject who used the approach compared to previous treatments may be attributed to the meticulous management of tendon load progression, prioritizing pain control. The inadequacy of past treatments, involving manual therapy and dry needling, or excessive load application like eccentric Nordic Hamstring exercises, underscores the importance of a carefully calibrated approach. While prior soft-tissue treatments may have contributed to a more rapid recovery for this subject, it is essential to highlight that the current methodology may have played a pivotal role in facilitating an even swifter recuperation than the previous treatment.
As pointed out by Goom et al.8 pain has to be a criteria to progress in the exercises program to adjust to the load that the tendon is capable of supporting at that moment. During this case, in order to make a comparison and contrast of the pain results throughout the process, the subject performed the same test (single leg arabesque) regardless of the training phase in which he was. Perhaps, in future studies, a test with less potential for irritability of the PHT, for example the single leg bridge, should be chosen to reduce required hip flexion during the test.
Other exercise treatment approaches as described by Cushman et al.9 in their case report, have proven beneficial. Rich et al.24 published a proposed crossover protocol for treatment of PHT using isometric/eccentric exercises. To enhance the robustness of future intervention protocols, it is crucial to investigate the proposed approach with greater number of subjects. The incorporation of isometric/eccentric exercises, along with the gradual introduction of hip flexion as recommended by Goom et al.8 should be considered as essential elements in the design of subsequent studies with larger sample sizes of those with PHT.
Functional questionnaires and pain assessments (VISA-H) during and after activity should serve as the primary outcome measures for evaluating tendon pathology. Numerous studies suggest that it is not solely the state of tendon structure but rather its inadequate adaptation to load that triggers the onset of symptoms.19,25–27 Futhermore, it would be interesting to include imaging studies in future research to evaluate the extent to which the state of the tendon structure contributes to the improvement of function and pain.
CONCLUSION
An exercise protocol focused upon load progression management for the treatment of PHT was beneficial to a male runner. Studies with a larger sample size and a more precise methodological design would be necessary to support this type of intervention in clinical practice.
Funding
This research received no specific grat from any funding agency in the public, commercial or not for profit sectors.
Conflicts of interest
The authors report no conflicts of interest.