
Introduction
Acetabular dysplasia (AD) is a hip joint condition that is characterized by incomplete development of the acetabulum leading to inadequate bony coverage of the femoral head,1 joint instability, and altered hip joint loading.2 AD leads to pain and decreased quality-of-life,2,3 decreased functional performance,4,5 and is a known risk factor for early-onset hip osteoarthritis (OA).6,7 Periacetabular osteotomy (PAO) is a hip preservation surgery for individuals with AD that aims to reposition the acetabulum to increase bony coverage of the femoral head with an overall goal of minimizing pain and improving function.8,9
The author team recently published a review that examined changes in pain intensity and physical activity (PA) levels in individuals with AD following PAO.10 This review reported that pain intensity decreased at six-months compared with pre-PAO levels across several studies,2,10–15 however, to authors’ knowledge, little evidence exists regarding pain recovery during the first six months following PAO. Our team further noted that self-reported PA levels in individuals with AD are negatively-impacted before PAO but improve one year following PAO.2,13–23 However, no previous studies have evaluated changes in PA prior to one year after PAO (i.e., during the first six months after PAO), and these previous studies primarily used self-reported PA measures (which have known risk of recall bias24),13–15,17–23 as opposed to a device-measured approach. Collectively, a comprehensive, longitudinal assessment of changes in pain intensity and PA levels in individuals with AD over the first six months after PAO could help guide decision-making regarding rehabilitation progression and return to sport or work following surgery.
The purpose of this study was to examine pain recovery and PA before and during the six months after PAO, in individuals with AD (i.e., lateral center edge angle “LCEA” of 20° or less25). The hypothesis was that individuals with AD would demonstrate significant improvements in pain intensity and PA levels over the first six months following PAO. Additionally, this study qualitatively examined differences in self-reported and device-measured PA levels.
Materials and Methods
The study followed a longitudinal cohort design. Potential participants were recruited (aged 14 to 49 years) with a confirmed diagnosis of AD who were scheduled for PAO with a single, fellowship-trained orthopaedic surgeon with a specialty in hip preservation (MKR). Diagnostic criteria of AD included a combination of the patient’s reported symptoms (e.g., intra-articular hip pain), radiological findings of AD (i.e., LCEA of 20° or less25), and no signs of significant hip joint degeneration (i.e., Tonnis grade of 1 or 026,27). Prior to PAO, all participants received hip arthroscopy to address intra-articular pathology, including labral tears, ligamentum teres tears, and cam deformities, as well as to confirm that articular cartilage quality was sufficient to proceed with a PAO. PAO surgical technique details are similar to previously-described techniques.9 Briefly, after standard supine positioning and preparation, an anterior-based incision provided access to the ischium, superior pubic ramus, and ilium. Cuts were made with fluoroscopic guidance around the acetabulum, while maintaining the continuity and integrity of the posterior column of the ilium. Once free, the acetabular fragment was rotated and positioned to optimally cover the femoral head. The fragment was stabilized with metal screws to allow bony healing.
After PAO, all participants followed a standardized rehabilitation program, including approximately six weeks of protected weightbearing (20%-foot flat partial weightbearing) with assistive devices. Active motion was limited until six weeks, and excessive hip flexion, extension, and external rotation were avoided. Weightbearing and strength progression began at week six, provided sufficient healing was noted on radiographs. Advanced strength training and running progressions began at approximately three months post-PAO, provided patients had sufficient motion, strength, no limp with walking, and continued progression of healing on radiographs. Full return-to-sport typically occurred between six to nine months post-PAO. Institutional review board approval (R-2024-1049) was granted, and all participants provided signed informed consent and/or assent and parental permission before participation.
Pain Intensity Evaluation Before and After PAO
A comprehensive hip-related pain evaluation was performed in individuals with AD before (mean=27 days; range=2-94 days) and at one week and one, three, and six months following PAO using: the Hip disability and Osteoarthritis Outcome Score pain subscale (HOOS-Pain)28 and the Numeric Pain Rating Scale (NPRS).29 The HOOS-pain is a 10-item valid and reliable hip pain measure that asks about hip-related pain in the last week.28,30,31 Each item is scored on a Likert scale from 0 to 4, and scores are transformed to a score of 0-100 (0=no pain and 100=worst pain).28 The NPRS is a numeric version of the visual analog scale, in which individuals select and mark a whole number ranging from 0 to 10 (0=no pain and 10= worst pain).29 The NPRS has been shown to demonstrate good validity and reliability in individuals with musculoskeletal pain.32,33 The NPRS was used to evaluate average pain over the prior week. Prior to and six months following PAO, pain evaluations were completed as a part of onsite study visits, whereas pain evaluations at one week, one month, and three months following PAO were completed remotely by participants.
Device-Measured Physical Activity Levels Before and After PAO
An accelerometer (ActiGraph; GT3X+; Pensacola, FL) was used to measure PA levels over a seven-day period, both before and again at six months after PAO. The accelerometer quantifies PA by capturing acceleration signals during movement, and motion outside normal human movement is band-pass filtered.34 The signal is then converted into activity counts using ActiGraph’s proprietary algorithm in sampling intervals (one-minute epochs in this study). This accelerometry approach is valid and reliable to quantify activity35 and has been used in several previous studies in individuals with AD before and/or after PAO.16,17 Participants were provided the accelerometer and were instructed to wear it during all waking hours, only removing it during water-based activities and prior to going to sleep. Participants wore the accelerometer around their waist and above the non-painful hip (pre-PAO) or the non-surgical hip (post-PAO), using an elastic belt and pouch. For the entire week, accelerometer-wear adherence was considered valid if wear-time was ≥8 hours per day and minimum of four valid days.34,36,37
Accelerometer data were downloaded and processed using ActiLife software (version 6.13.3). We computed minute-by-minute activity counts of data from valid days.34,38 PA variables of interest included average time (minutes) per day spent in sedentary behavior (SB; <100 activity counts/min),35 light PA (100–1,951 activity counts/min),35 and moderate-to-vigorous physical activity (MVPA; ≥1,952 activity counts/min),35 as well as average daily steps both before and six months after PAO, using uniaxial activity count cut-points developed in healthy adults.35,39
Self-Reported Physical Activity Levels Before and After PAO
The International Physical Activity Questionnaire short form (IPAQ-SF) was used to evaluate self-reported PA levels both before and 6 months after PAO.40 The IPAQ-SF is a valid and reliable PA measure,41,42 and is among the most widely-used self-reported measures of PA.43 It contains nine items that evaluate PA levels in various domains over the seven days prior to completion. The average time spent (minutes) in walking and in MVPA over the week prior to study visits before and six months after PAO were calculated.
Statistical Analyses
Percentages/frequencies were computed for categorical data and means/standard deviations for continuous data. A repeated-measures one-way analysis of variance (ANOVA) was used to examine changes in pain intensity across all time points (pre-PAO; one week after PAO; one, three, and six months after PAO). Paired t-tests were used to evaluate differences in device-measured PA levels (i.e., SB, light PA, MVPA, and daily steps) before and six months after PAO, as well as average accelerometer wear time before and after PAO. As secondary analyses, differences in self-reported PA variables were examined before and six months after PAO (average minutes of walking and MVPA) using paired t-tests as well as qualitatively summarized time spent in MVPA measured by accelerometers versus IPAQ-SF measures at each time point (before and six months after PAO). Effect sizes (Cohen’s d) were calculated where appropriate and interpreted these as: 0.2 small, 0.5 medium, 0.8 large.44 We set the statistical significance level a priori (α=0.05) for all statistical comparisons.
Results
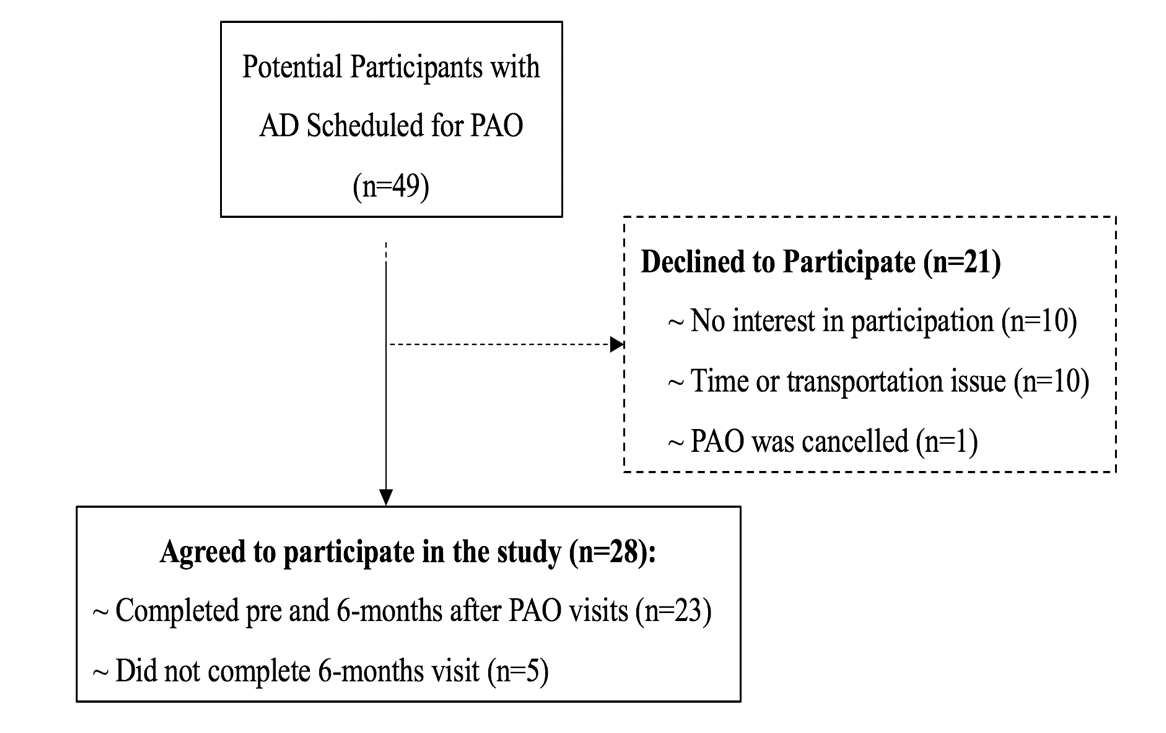
Twenty-three out of 28 individuals (82.1%) completed all study measures at both testing visits (Figure 1). Demographic and clinical data for the cohort are presented in Table 1.

HOOS-Pain Intensity Before and After PAO
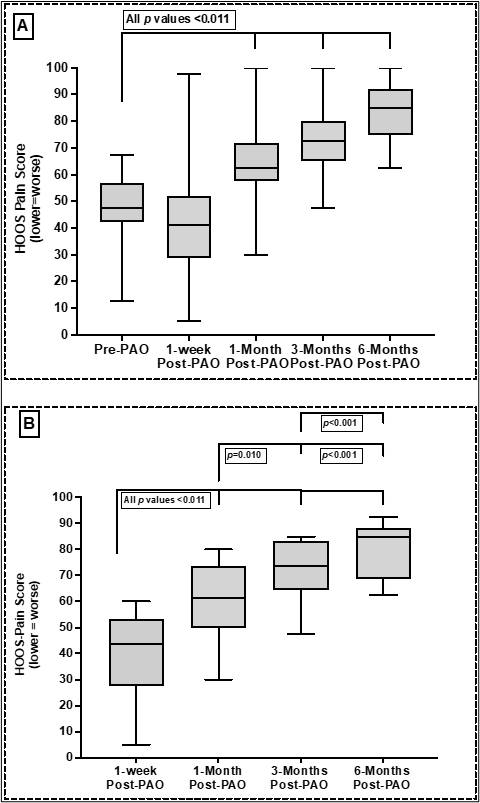
The average HOOS-Pain score was 48.3±12.5 before PAO, and 41.0±20.6, 63.0±15.0, 73.1±11.1, 82.5±10.9 at one week, one month, three months, and six months following PAO, respectively. For one-way repeated measures ANOVA testing, the assumption of sphericity was met (p=0.262). There were significant differences in pain intensity across time points following PAO (df=4, F=52.268, p<0.001). With post-hoc tests, significant improvements were observed in pain intensity at one month and onward following PAO compared with pain intensity before PAO (Figure 2A) and pain improvements at one month, three, and six months after PAO compared with pain intensity 1 week after PAO, as well as pain improvements at four and six months after PAO compared with pain intensity six months after PAO (Figure 2B).
_hoos_pain_comparisons_following_pao_compared_with_pre-pao_and_b)_hoos_pain_comparisons_.png)
NPRS-Pain Intensity Before and After PAO
The average NPRS score was 8.0±1.4 before PAO, and 8.3±1.9, 5.9±2.1, 4.5±1.8, 3.7±1.8 at one week, one month, three months, and six months following PAO, respectively. The sphericity assumption for one-way repeated measures ANOVA testing was met (p=0.346). There were significant differences in pain intensity across time points following PAO (df=4, F=35.764, p<0.001). With post-hoc tests, significant improvements were observed in pain intensity at one month and onward following PAO compared with pain intensity prior to PAO (Figure 3A) and pain improvements at one month, three, and six months after PAO compared with pain intensity one week after PAO, as well as pain improvements three and six months after PAO compared to pain intensity one month after PAO (Figure 3B).
_nprs_pain_comparisons_following_pao_compared_with_prior_to_pao_and_b)_nprs_pain_compari.png)
Device-Measured Physical Activity Levels Before and After PAO
There were no significant differences in mean time spent in SB, light PA, MVPA, or daily step counts between prior to and six months after PAO (Table 2). Additionally, mean wear time did not differ between prior to and six months after PAO. (Table 2).
Self-Reported Physical Activity Levels Before and After PAO
On average, individuals with AD reported that they spent 147.7±174.1 minutes per day before PAO and 204.0±210.0 minutes per day six-months following PAO in walking. On average, individuals with AD reported that they spent 71.9±156.6 minutes per day before PAO and 121.2±192.2 minutes per day six months following PAO in MVPA. There were no significant differences in time spent in both walking (p=0.262; d=0.3) and MVPA (p=0.169; d=0.3) between prior to and six months following PAO. A qualitative comparison between time average spent in device-measured and self-reported MVPA at each time point is shown in Table 3.
Discussion
In this longitudinal cohort study, pain recovery was examined in individuals with AD before and at multiple time points following PAO, and PA levels before and six months after PAO using both a device-measured approach and a self-reported PA measure. Additionally, time spent in device-measured and self-reported MVPA before and six months after PAO were qualitatively summarized and compared. The study’s hypothesis was partially supported in that individuals with AD reported significant, gradual decreases in pain at one month and onward following PAO, compared with pre-PAO pain intensity. However, device-measured and self-reported PA levels did not statistically change/improve in the six months following PAO, compared with pre-PAO PA levels. Interestingly, individuals with AD reported more time spent in MVPA measured by the IPAQ-SF compared with time spent measured by accelerometers, both before and six months after PAO. To authors’ knowledge, this is the first prospective cohort study to evaluate early and longitudinal pain recovery following PAO in individuals with AD as well as to evaluate PA levels during the first 6 months following PAO.
Significant reductions in pain intensity (HOOS-pain and NPRS) at one month, three, and six months following PAO, compared with pre-PAO pain intensity were observed (Figures 2 and 3). Additionally, significant reductions in pain intensity at multiple time points following PAO were observed including: i) One month, three, and six months following PAO compared with one week following PAO, ii) three and six months following PAO compared with one month following PAO, and lastly, iii) six months following PAO compared with three months following PAO (HOOS-Pain only). The majority of prior studies that have examined pain improvements following PAO have evaluated pain recovery only as early as six months and later following PAO.2,10–14,18,19,45 Generally, these studies reported that pain significantly decreased/improved at six months following PAO compared to before PAO.2,11–14,18,19,45 However, to authors’ knowledge, only one previous study has examined pain intensity earlier than six months following PAO, and reported no significant improvements in pain at four months following PAO compared with pre-PAO pain intensity.15 In this study, significant reduction in pain (across both the HOOS and NPRS) at one month and onward following PAO was found when compared to pre-PAO pain intensity.
In clinical practice, a 10-point change in the HOOS-Pain following PAO46 and ≥35% change in the NPRS following orthopaedic surgeries47 are considered as minimal clinically important difference (MCID) values. In this study, participants reported more than a 10-point improvement in HOOS-Pain scores at one month and onward (Figure 2) as we well as greater than a 35% reduction in NPRS at three months (Figure 3) following PAO, compared with pre-PAO pain intensity. Altogether, the comprehensive, longitudinal pain evaluation (HOOS and NPRS) showed that pain gradually decreased as early as one month following PAO, with the greatest degree of pain reductions occurring between one-week and one month and between one month and three months after surgery. Additionally, these improvements were clinically significant (exceeding MCID) at latest follow-up (six months following PAO).
To authors’ knowledge, there are no previous studies reporting PA estimates at six months following PAO. When examining differences in device-measured and self-reported PA levels before and six months after PAO, we found no significant differences in the PA variables. Two previous prospective studies examined changes in device-measured PA levels in individuals with AD following PAO.15,17 The first study (n=77) evaluated PA levels over seven days, both before and one year after PAO using a thigh-worn accelerometer.17 Similar to the current results, that study reported no significant improvements in time spent in very low-, low-, moderate-, and high-intensity activity one year after PAO compared to pre-PAO.17 The second study (n=23) measured PA levels over five days, both four months and one year after PAO (no baseline/pre-surgical PA data reported) using a thigh-worn accelerometer.15 That study reported no significant improvements in time spent in standing, walking, running, or sit-to-stand tasks one year after PAO compared with time spent in the same activities 4 months after PAO.15 Notably, in the self-reported PA-related findings, individuals with AD reported spending ~56.3 more minutes in walking and ~49.3 more minutes in MVPA six months after PAO compared with pre-PAO levels (both small-to-medium effect size; no statistically-significant differences were observed). Five prospective2,13–15,17 and three retrospective18–20 previously-published studies have examined changes in self-reported PA levels before PAO and at four months and up to five years following PAO. Whereas these studies used different self-reported measures than used in our study (the HAGOS and UCLA), across all previously published studies, self-reported PA levels significantly improved at one year after PAO. Importantly, our relatively small sample size may have limited our power and ability to detect differences in PA levels between pre-surgery and six months following PAO.
As described above, a significant decrease in pain intensity six months following PAO compared with pre-PAO pain intensity was observed in the current cohort (Figures 2 and 3). Previous work has shown that pre-PAO pain correlates with functional limitations following PAO.48 Thus, decreases in pain intensity at six months following PAO could be an important factor associated with a person’s ability to engage in increased PA following PAO. However, there were no statistically significant improvements in any PA variable in this cohort. In this study, the participants did not start weightbearing on their surgical limb and walking without assistive devices until six weeks, on average (range 2-12 weeks) after PAO. Thus, given the relatively short timeframe between post-operative weight-bearing onset and their follow-up PA data collection at six months, there may have been insufficient time to appreciate statistically significant improvements in PA levels. As mentioned previously, this study likely was underpowered to detect differences in PA levels between pre-surgery and six months following PAO. Despite not finding a statistically significant improvements, evaluating and improving PA engagement following PAO is likely critical for long-term joint health and overall health. Clinicians working with patients with AD undergoing PAO may consider monitoring PA levels at multiple time points following PAO using commercially available devices (e.g., Fitbit) as it may provide unique device-measured data related to recovery and return to prior level of function following surgery. Alternatively, PAO and subsequent rehabilitation might not be sufficient to change/improve PA engagement in individuals following PAO, and other unique interventions (such as targeted behavioral change PA programs) may be needed to improve activity participation in this patient population.
When qualitatively summarizing time spent in MVPA measured by accelerometers versus the IPAQ-SF, a large difference between the two measures was observed, both before and six months after PAO. Before PAO, individuals with AD reported more than triple the time spent in MVPA on the IPAQ-SF (73.3 mins/day), compared with the time spent in MVPA that was measured by the accelerometers (22.6 mins/day). At six months following PAO, individuals with AD similarly reported more than triple the time spent in MVPA via the IPAQ-SF (121.2 mins/day) compared with the time spent in MVPA measured by accelerometers (25.0 mins/day). Although both the IPAQ-SF and accelerometers report MVPA in minutes/day, it is important to note that these approaches differ in the specific activity-related constructs they measure. The IPAQ is a self-reported PA measure that recalls salient activities, whereas accelerometers capture accelerations related to all ambulatory movement.34 Taken together, these findings indicate that the IPAQ-SF may overestimate time spent in MVPA in individuals with AD, both before and six months after PAO. Potentially, these differences and the tendency for self-reported PA measures to overestimate PA levels may be accounted for by recall bias.41 On the other hand, and because patients with AD often report hip instability and pain2,3 that could influence gait performance, energy expenditure, and/or exercise capacity, there may be a need for AD/PAO-specific accelerometer processing cut-points to better evaluate activity volume in this patient population.
Limitations
The current study has several limitations to recognize. Firstly, the sample size was relatively small (n=23). However, due to the epidemiological nature of AD, the prevalence of AD is considered low (1-3% of the general population) when compared with similar intra-articular hip pain conditions (femoroacetabular impingement syndrome or hip OA).2,49–51 Secondly, the sample was predominantly females (22 females). This was to be expected, as epidemiological data show that 80% or more of AD diagnoses are in females.2,49–51 Thirdly, because PAO is a major orthopaedic procedure requiring subspecialty training, our coauthor (MKR), is one of only a few hip surgeons in the region in which the study was conducted that performs this procedure, and thus subjects were only recruited from a single institution. In light of this, the current findings may not be generalizable to other PAO patients of a different demographic makeup, those with varied surgical technique, those treated elsewhere, or those undergoing varying rehabilitation approaches. Lastly, it is important to not neglect limitations related to PA evaluation in this study. Specifically, participants may have had difficulty describing their PA behavior when completing the IPAQ-SF. Prior research reported that individuals completing the IPAQ-SF often had challenges understanding terms used in the questionnaire, potentially leading to errors in the collection of self-reported PA data.52 Additionally, patients with AD in the current study may have altered their activity behavior in ways not measured by the accelerometers. For example, whereas lower limb/walking-related activity might have been reduced, upper body activity might have been performed relatively more frequently but may not have been captured by accelerometers worn on the hip/waist. Future studies should include a larger sample of individuals with AD undergoing PAO and examine PA levels changes over time following PAO and examine the potential impact of baseline factors associated with increased PA participation in this patient population. Secondly, future studies could further examine individuals changes in pain and PA over time, as well as examining potential trajectories of pain and PA recovery in those with AD following PAO. Thirdly, evaluating changes in the participation in specific type of PA (as opposed to just volume and intensity of activity measures by the accelerometer) might have provided additional insight into activity-related recovery following PAO. Lastly, despite the lack of improvement in PA from prior to six months after PAO, future research could examine whether the patient’s experience during activity (e.g., pain or self-efficacy) might have improved over time.
Conclusion
Compared to pre-PAO, individuals with AD reported pain reduction as early as one month following PAO and the reduction in pain continued over the entire six month period. By comparison, PA levels remained the same six months after PAO. There was a large difference in time spent in MVPA between accelerometry-based and self-reported PA measures, both before and six months after PAO.
Conflict of interest
The authors declare no conflicts of interest related to this work.
Acknowledgment
The author extends the appreciation to the Deanship of Postgraduate Studies and Scientific Research at Majmaah University for funding this research work through the project number (R-2024-1049). We would also like to thank our clinical collaborators at the Hip Center at Andrews Sports Medicine and Orthopaedic Center, Kirby Kelley and Hannah Harrity, for their assistance in recruiting participants for this study. Additionally, we would like to thank Hadeel Alghanim for her assistance in data collection for some of the included participants in this study.
Funding
This work was funded by the NIH National Rehabilitation Research Resource to Enhance Clinical Trials REACT Scholar Award. The author extends the appreciation to the Deanship of Postgraduate Studies and Scientific Research at Majmaah University for funding this research work through the project number (R-2024-1049).