


INTRODUCTION
An estimated 200,000 people suffer an anterior cruciate ligament (ACL) injury each year1,2 with a higher injury rate in females than males.3 While many people will undergo an ACL reconstruction (ACLR) and/or perform physical rehabilitation, evidence suggests that only 70% will return to their previous level of function.4 For those that do return to sport, approximately 30% will be at risk of suffering a subsequent ACL injury to either the contralateral limb or ipsilateral limb.5
Previous authors have shown that deficits of muscular strength, particularly in the quadriceps,6–8 hamstrings,8,9 hip abductors,4,10,11 hip extensors,12–14 and hip rotators15 of the involved side exist and may persist for many years after injury16 and contribute to poor long-term outcomes by allowing for reduced knee joint stability, altered biomechanics, and a diminished ability to adequately dampen impact forces during different weightbearing and landing activities.4,6,17 Additionally, muscular strength deficits and asymmetries between the involved side and the uninvolved side are a risk factor for primary18 and secondary19 ACL injury. Therefore, identifying muscular strength deficits may be a critical component for secondary and tertiary injury risk reduction efforts.
Limb symmetry index (LSI) is one of the most common methods for identifying muscular strength deficits in those who have suffered a prior ACL injury.20 LSI is calculated by dividing the strength of the involved limb by the strength of the uninvolved limb and multiplying that by 100 to get a percentage, equation provided below in (1).21 While using the LSI has become standard practice, sports medicine professionals and researchers have raised concerns about using the uninvolved limb as a reference, as negative strength adaptations may occur in both limbs after ACL injury.20,22–26 Furthermore, after ACLR, people often demonstrate muscle strength deficits in both the involved and uninvolved limbs when compared to their uninjured peers.23,27 Since the uninvolved limb in those with an ACLR appears to be weaker than their uninjured peers, this calls into question the appropriateness of using the uninvolved limb as the standard for comparison after an ACL injury.
LSI=[ Injured Limb Uninvolved Limb ]×100
Research on the strength of the uninvolved limb in individuals with ACL injury compared to healthy individuals is more extensively available for the quadriceps8,15,23,28 and hamstrings,3,8,23,28 and less so, for the gluteus medius,8,15 gluteus maximus,8,15,29 hip external rotators,15 and hip internal rotators.15 However, interpretation of this research is challenging due to variations in populations studied, including age,30 sport,19,30 and athletic level,19,30 small sample sizes,4,8,26,31 inconsistent testing times after injury,8,28,32,33 limited muscle groups tested,32–34 and differences in testing parameters such as muscle contraction type15,30,35 and speed.28,30,35
Thus, it is not clear if muscular strength in the uninvolved limb of those with ACL injury history is reduced compared to those with no prior ACL injury. Therefore, the primary purpose of this study was to compare the strength of key lower extremity muscles of the uninvolved limb in those with history of ACL injury (ACL-I) to the dominant limb in individuals with no history of ACL injury (control). These key muscles include: the quadriceps, hamstrings, gluteus medius, gluteus maximus, hip external rotators, and hip internal rotators. The hypothesis was that the uninvolved (UNINV) limb in the ACL-I group would demonstrate muscle strength deficits in all muscle groups when compared to the dominant (DOM) limb of the control group. While the study design did not allow for control of every potential confounding factor in the interpretation mentioned previously, the methods employed are believed to enhance the clinical significance of the findings within the defined scope of this study.
METHODS
This study uses data from the 2005-2009 years of enrollment in the JUMP-ACL (Joint Undertaking to Monitor and Prevent ACL Injury) study, a prospective cohort study of biomechanical risk factors for ACL injury. Participants were included if they recorded successful trials of the six muscle groups of interest. This paper represents a cross-sectional analysis of the baseline data collected at the time of enrollment to describe the strength difference of six muscle groups between the UNINV limb in the ACL-I group compared to the DOM limb of the control group.
Participants
A total of 5,908 cadets and midshipmen at the United States (U.S.) Air Force, Military and Naval Academies participated in the study and performed initial biomechanical testing during their initial summer of training (Figure 1). Informed consent was obtained from each participant in accordance with each institution’s review board. At the time of data collection, participants without a current musculoskeletal injury and were able to perform the study tasks were included. Participants were identified as having an ACL injury history (ACL-I group) or no prior ACL injury (control group) via self-report on the baseline questionnaire administered at the time of informed consent. Those in the ACL-I group had to receive a medical waiver through the Department of Defense Medical Evaluation Review Board and were deemed fit to participate in the physically demanding military training program at the U.S. Service Academies and had no physical activity restrictions at the time of consent. Additionally, from the original dataset, only participants who performed all strength tests were included in this study’s data analysis.

Muscle Strength
Isometric strength of the quadriceps, hamstrings, gluteus medius, gluteus maximus, hip external rotators, and hip internal rotators were assessed using a hand-held dynamometer (NexGen Ergonomics, Quebec, Canada). At the time of data collection, the testing was carried out by a team of Certified Athletic Trainer Research Assistants, each of whom underwent a standardized training regimen and successfully passed a comprehensive validation assessment to ensure their competence. Previous studies have shown their intra-rater reliability (ICC2,k) for the testing positions (Figure 2) to range from 0.73 to 0.98.36 These specific testing positions were selected to minimize participant movement while ensuring efficient assessment of strength, given that strength testing was integrated into the procedures of a large-scale data collection. In the control group, the DOM limb, defined as the preferred leg to kick a ball, was used for testing while the UNINV limb was tested in the ACL-I group. In the control group, the DOM limb was selected to undergo testing as it has been demonstrated to be as strong or stronger than the non-dominant limb.37,38 This decision ensures that the ACL-I group’s UNINV limb would be compared to the highest standard. Participants were asked to push into the dynamometer as hard as they could for five seconds (Supplemental File 1). The mean force measurements across two 5-second trials were averaged together. All strength values were converted to torque by multiplying the recorded force (N) by the participant’s lever arm length (m), which was measured as the distance from the lateral femoral epicondyle to the location of the dynamometer for the quadriceps and hamstrings and from the superior aspect of the greater trochanter to the location of the dynamometer for the gluteus medius and gluteus maximus. All torque values were then normalized to the participant’s body mass, as seen in (2).
Normalized Torque = Newton × meter kilogram

Data Processing
The primary outcome variable of interest was the average mean isometric muscular strength of six different muscle groups between the uninvolved (UNINV) limb in those with a history of ACL injury who had returned to unrestricted activities (ACL-I group) to the dominant (DOM) limb in individuals with no history of ACL injury (control group). Each group’s strength variables were graphically analyzed for normality. Additionally, the strength variables underwent several data cleaning steps, including 1) winsorizing outliers that were ± 3 SD above and below the mean (<1% of variables for each muscle group for the control group and 0% for the ACL-I group), and 2) removal of rows with missing data. Missingness accounted for <1.6% of the dataset, given the large sample size it is a reasonable strategy to opt for removal as a means for handling missing data.39
Data Analysis
All analyses were completed using RStudio Version 1.3.1073. Data were analyzed by conducting separate two-way analyses of variance (ANOVA) considering sex (female, male) and limb (UNINV in ACL-I group, DOM limb in the control group) for each of the six muscle groups tested using a priori alpha level of 0.05. To complement the p-values, effect sizes using Cohen’s d (d) were calculated for the main effects of sex and limb strength to provide a more comprehensive characterization of differences between groups. Effect size magnitude was interpreted as trivial (0-0.19), small (0.20-0.49), medium (0.50-0.79) and large (>0.8).40 Polarity of the effect sizes were adjusted so that positive effect sizes indicated increased strength in the UNINV limb compared to the DOM limb or increased male muscular strength compared to females. Negative effect sizes indicated reduced strength in the UNINV limb compared to the DOM limb or increased female muscular strength compared to males.
RESULTS
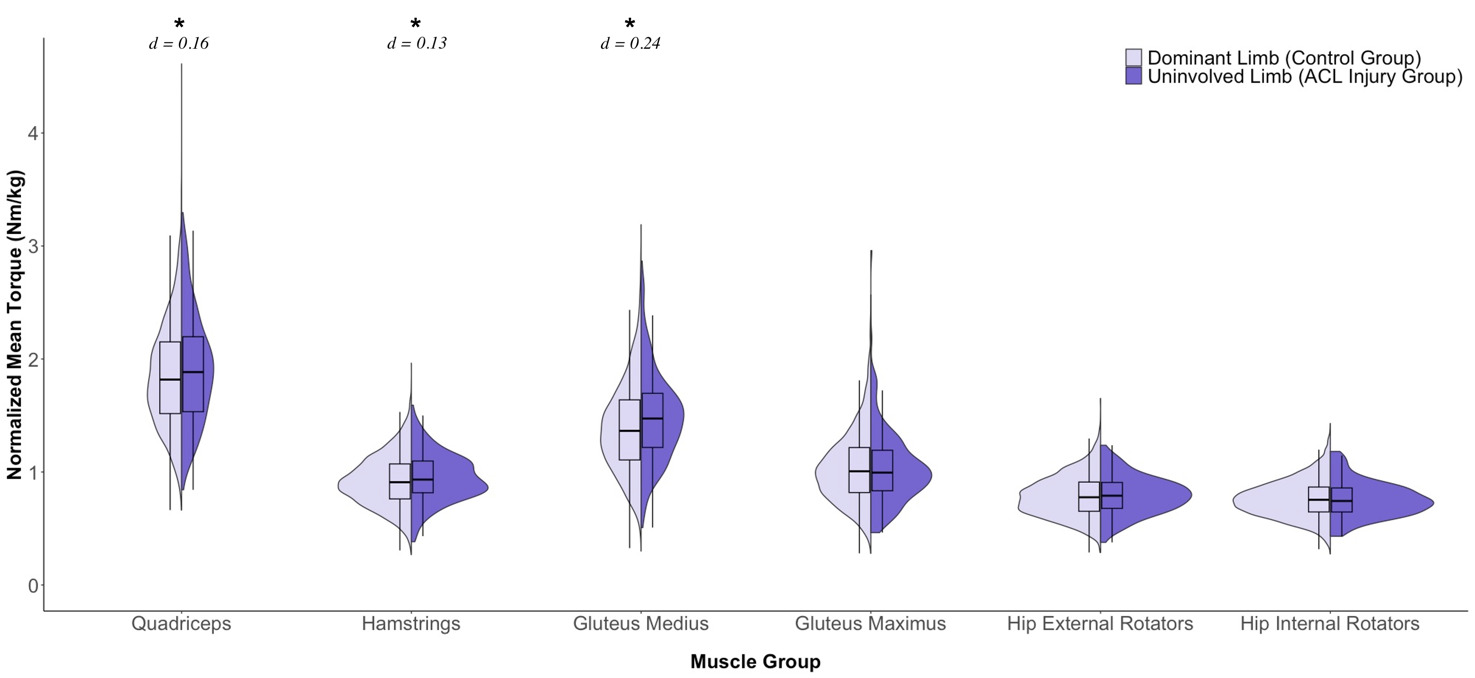
Baseline demographic information for each group at the time of enrollment is presented in Table 1 and the observed strength values for each limb (DOM, UNINV) by sex (females, males) are presented in Table 2. The results indicate significant main effects for limb, with the UNINV limb being stronger in the quadriceps (F1,5723 = 7.926, p = 0.005), hamstrings (F1,5723 = 4.256, p = 0.039), and gluteus medius (F1,5723 = 12.520, p <0.001), but not for the gluteus maximus (F1,5723 = 0.244, p = 0.621), hip external rotators (F1,5723 = 0.674, p = 0.412), or the hip internal rotators (F1,5723 = 0.075, p = 0.784) (Figure 3). Limb differences in strength showed trivial to small effect sizes (d) were present for the of the quadriceps (d = 0.16, 95% CI: 0.02-0.30), hamstrings (d = 0.13, 95% CI: -0.01-0.27), gluteus medius (d = 0.24, 95% CI: 0.10-0.38), gluteus maximus (d = -0.04, 95% CI: -0.18-0.10), hip external rotators (d = 0.04, 95% CI: -0.10-0.18), and hip internal rotators (d = -0.02, 95% CI: -0.16-0.12).
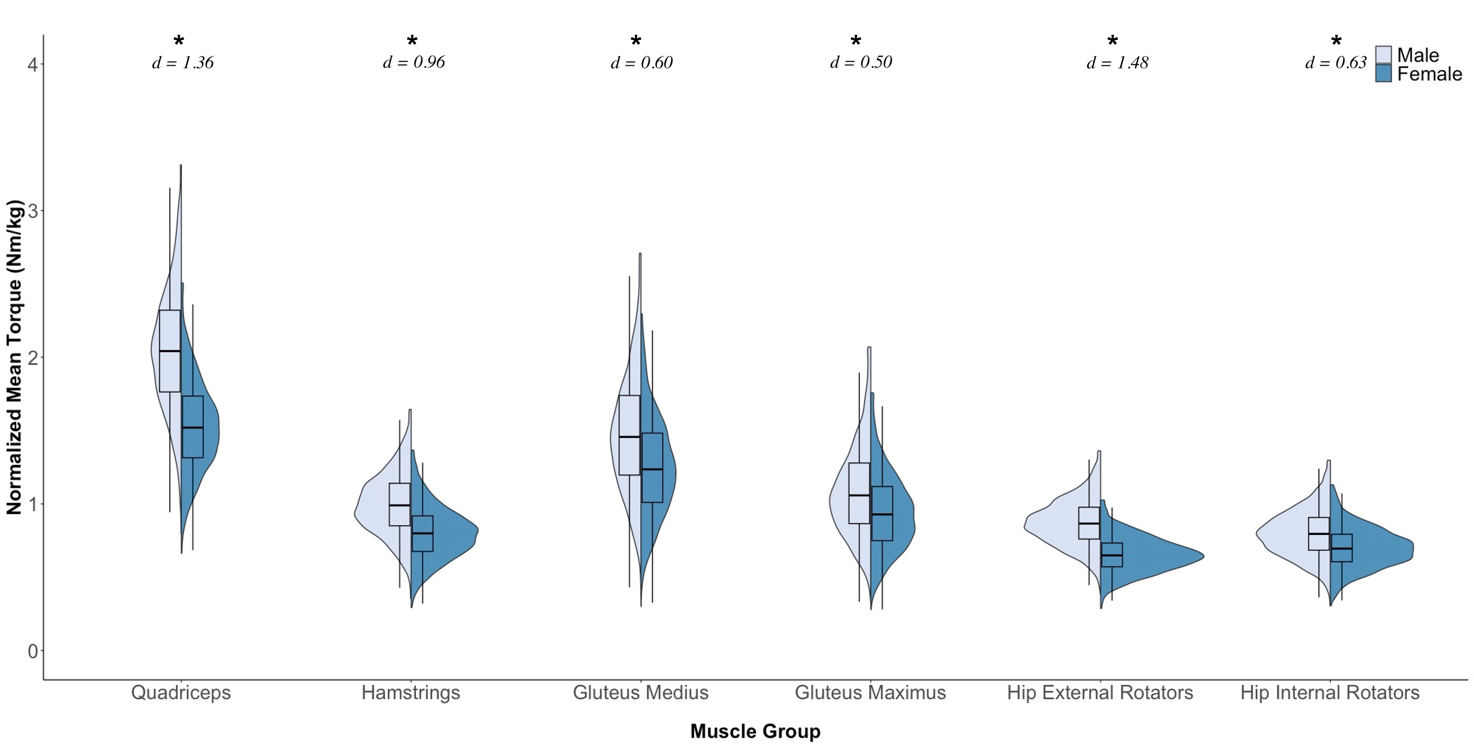
Significant main effects for sex were observed, with males demonstrating greater strength in the quadriceps (F1,5723 = 2519.699, p <0.001), hamstrings (F1,5723 = 1251.848, p <0.001), gluteus medius (F1,5723 = 492.309, p <0.001), gluteus maximus (F1,5723 = 335.107, p <0.001), hip external rotators (F1,5723 = 2968.519, p <0.001), and hip internal rotators (F1,5723 = 545.594, p <0.001) (Figure 4). Effect sizes ranged from small to large for the sex differences in strength of the quadriceps (d = 1.36, 95% CI: 1.30 -1.42), hamstrings (d = 0.96, 95% CI: 0.90-1.01), gluteus medius (d = 0.60, 95% CI: 0.55-0.66), gluteus maximus (d = 0.50, 95% CI: 0.44-0.55), hip external rotators (d = 1.48, 95% CI: 1.42 -1.54), and hip internal rotators (d = 0.63, 95% CI: 0.58-0.69).
_and_fema.png)
There were no limb-by-sex interactions observed for the quadriceps (F1,5723 = 0.008, p = 0.927), hamstrings (F1,5723 = 0.416, p = 0.519), gluteus medius (F1,5723 = 1.034, p = 0.309), gluteus maximus (F1,5723 = 2.830, p = 0.093), hip external rotators (F1,5723 = 0.520, p = 0.471), or hip internal rotators (F1,5723 = 3.695, p = 0.055) (Table 2). The lack of a significant limb-by-sex interaction indicates that the observed differences in strength between limbs was similar for males and females.
DISCUSSION
The primary purpose of this study was to compare the muscular strength of the uninvolved (UNINV) limb in those with a history of ACL injury who had returned to unrestricted activities (ACL-I group) to the dominant (DOM) limb in individuals with no history of ACL injury (control group). The most important finding was that there was no clinically meaningful evidence (effect size, d < 0.25) of strength deficits in the UNINV limb for the quadriceps, hamstrings, gluteus medius, gluteus maximus, hip external rotators, or hip internal rotators muscle groups. While the UNINV limb in the ACL-I group displayed statistically higher strength values for the quadriceps, hamstrings, and gluteus medius muscle groups when compared to the DOM limb of the control group. This may be secondary to compensatory movement patterns and/or neuromuscular control changes developed after injury, resulting in more load on the uninvolved limb, which has been shown in other literature.41–45 Given the small effect sizes, it is important to interpret the significance of the findings with caution as they might not be clinically meaningful. Take into consideration that larger sample sizes used in studies can increase the likelihood of detecting statistically significant differences (p-value < 0.05) even when the effect size is negligible, resulting in type I errors or false positives. Therefore, the results indicate that in those who have returned to unrestricted activities after ACLR, the UNINV limb’s strength can be used as a benchmark for determining if the individual has sufficient strength by comparing it to their involved limb.
The sample included in this study was substantial, with 5,519 participants in the control group and 208 participants in the ACL-I group, which represents the largest study examining lower extremity strength profiles to the best knowledge of the authors. Although there were statistically significant main effects for limb with greater strength in the UNINV limb in those with ACL injury history for the quadriceps, hamstrings, and gluteus medius in this sample, their respective effects sizes were small (d < 0.25). Consequently, while the results may be statistically significant, they may not be clinically relevant. There were no limb-by-sex interactions meaning the differences in muscle strength between the UNINV limb (ACL-I group) and the dominant limb (control group) were consistent across both sexes. Therefore, these results suggest that sports medicine professionals may use limb symmetry for muscle strength assessment in patients who have been cleared to participate in all activities after an ACL injury without concerns about strength deficits in the UNINV limb.
Maximal Isometric Muscle Strength
Although previously suggested mechanisms for muscle weakness in the UNINV limb after injury exist including prolonged arthrogenic inhibition,26,46 deconditioning,23 or lack of re-conditioning,23 the findings of the current study showed no difference in UNINV muscular strength compared to the DOM limb of healthy controls at the time of testing.
Although previously suggested mechanisms for muscle weakness in the uninvolved (UNINV) limb after injury, such as prolonged arthrogenic inhibition,26,46 deconditioning,23 or lack of re-conditioning,23 this study’s findings present a nuanced picture. While small statistically significant differences in three of the muscle groups were observed between the UNINV and dominant (DOM) limbs of healthy controls, the associated effect sizes were consistently small to trivial, suggesting that, from a clinical perspective, the observed differences may not be practically significant. In essence, although there were statistical differences in muscle strength, the limited impact on a practical level implies that the UNINV limb can be considered a reliable surrogate for comparison to the DOM limb. This reinforces the notion that, despite subtle statistical variations, the UNINV limb remains a valuable benchmark for assessing muscle strength in individuals with a history of ACL injury who have returned to unrestricted activities.
Knee Strength
Previous studies examining quadriceps and hamstrings strength in those with a history of an ACL injury and those with no prior ACL injury individuals have produced conflicting results. The present study supports previous research reporting no clinically significant differences in the UNINV limb strength of the quadriceps19,33–35,47–51 and hamstrings8,19,26,33,35,50,52,53 for individuals with ACLR compared to healthy controls after approximately six months. However, other studies have reported both increased8 and decreased23,26,54,55 quadriceps strength and decreased hamstrings23 strength in the UNINV limb after ACL injury when compared to those with no prior ACL injury. The reason for the discrepancies in these findings is unclear, but factors such as time since injury/reconstruction,15,23,35,47,48 graft type,35,51 patient population characteristics (age,19,23,34 sex breakdown,19 and fitness level19,34), and strength assessment methods19,23,52 may play roles. This study aimed to mitigate the potential impact of these factors through the inclusion/exclusion criteria focusing in on a relatively homogenous participant group in terms of age and fitness level and focused in on one aspect of strength isometric testing. The conflicting results highlight the need for future research to clarify the relationship between strength in individuals with a history of ACL injury and strength in individuals with no prior ACL injury across multiple time points, both acutely and chronically.
Hip Strength
The results of the current study, indicating a small effect but likely not clinically meaningful discernible difference in gluteus medius strength between the UNINV limb in the ACL-I group and the DOM limb in the healthy control group, align with findings in recreational athletes acutely,26 when cleared to return to play,8,11,34 and several years after ACLR.56 Of note, while weaker hip abduction muscle strength has been linked to potential knee injury positions10,57 and decreased gluteus medius strength in the involved limb after a knee injury,10,58 to the best of the authors’ knowledge, no studies have reported a decrease in gluteus medius of the UNINV limb after an ACL injury.
The majority of previous research investigating gluteus maximus strength supports the current study’s findings that demonstrate no discernable differences in gluteus maximus strength between the UNINV limb in those with a history of ACL injury and the DOM limb in those with no prior ACL injury.8,26,29 Conversely, Tate et al. identified weakness in the UNINV limb’s gluteus maximus after ACLR compared to the DOM limb in healthy controls.4 The difference may be explained by their participants’ lower fitness level, as they were only recreationally active at least 2x/week for 30 minutes and engaged in jumping or cutting activities at least 1x/month. That activity level would be relatively low compared to the activity level of the military cadets in this study. Interestingly, Bell et al. observed that individuals with weaker quadriceps strength in the UNINV limb after ACLR demonstrated an increase in gluteus maximus strength in the UNINV limb compared to healthy controls, possibly as a compensatory mechanism.15 However, they found no differences in the UNINV limb’s gluteus maximus strength in participants with high quadriceps strength in the UNINV limb compared to healthy controls. Notably, the average time from surgery for the ACLR group was approximately two to three years in their study, which represents a period of having returned to unrestricted activity. While the current study did not ask when the ACL injury occurred, all participants had been cleared for unrestricted activity.
No differences were observed in hip external or internal rotator strength between the UNINV limb in individuals with ACL-I and the DOM limb in the healthy control group. Previous hip external rotator strength findings are mixed.15,34 Discrepancies between the two studies may be attributed to the age discrepancy between the two cohorts (~14 vs. ~18 years old) and the fact that research demonstrating reduced hip external rotator strength in the UNINV limb solely focused on female athletes.34 Only one study was identified examining hip internal rotation strength, which also reported no discernible differences in strength between the UNINV limb in individuals with a history of ACL injury and the DOM limb in those without prior ACL injury.15 In summary, the results of this study lend support to findings indicating that strength of the gluteus maximus, gluteus medius, hip internal rotators, and external rotators of the UNINV limb does not appear to be decreased in military cadets who have returned to unrestricted activity after ACL injury.
Sex Differences
While there was no evidence of reduced strength in the UNINV limb for both sexes, males were statistically stronger than females in all muscle groups. The statistically significant differences were accompanied by small to large effect sizes indicating meaningful differences (Figure 4). These findings are consistent with previous research on young athletic populations, which also showed that males were stronger than females.59,60 Therefore, when designing rehabilitation programs, sports medicine professionals should consider sex differences in lower extremity muscular strength. Additionally, future research should establish normative values using sex-specific lower extremity muscular strength standards.
Clinical Application
Sports medicine professionals may use this study’s findings to assess and monitor strength deficits in patients with a history of ACL injury who have returned to unrestricted activities. By using the uninvolved limb’s strength in individuals with a history of ACL injury as a proxy for the dominant limb in those without prior ACL injury when utilizing the limb symmetry index, clinicians can develop individualized and effective rehabilitation protocols, including strength training programs, to restore muscle symmetry and optimize functional outcomes. This study also highlights the importance of accounting for sex differences in lower extremity muscular strength when establishing normative values for future research. Using the uninvolved limb as a benchmark for comparison, sports medicine professionals can make more informed clinical decisions, design effective rehabilitation programs, and improve musculoskeletal injury risk screenings for individuals with a history of ACL injury.
It should be noted that while this study has a large sample size and provides valuable insights into using the uninvolved limb as an appropriate benchmark, it’s important to acknowledge that all participants had been medically cleared for physical activity at the time of the study. Therefore, they do not represent individuals in the early or sub-acute phases post-surgery, where the use of the non-injured limb as a reference for LSI might be less applicable. Additionally, practitioners should proceed with caution if attempting to compare the average strength values with those reported in previous studies. The variations in testing positions and the equipment used pose a challenge for direct comparisons. For example, research indicates that maximal isometric strength values obtained from hand-held dynamometers are often lower than those measured by isokinetic dynamometers.61 This discrepancy underscores the challenges in comparing strength measures across different methodologies. Furthermore, while isometric strength assessments provide a measure of muscle force generation, they might not comprehensively reflect the intricate dynamics of neuromuscular control that influence functional movement. This is an important consideration as persistent neuromuscular deficits, even in the presence of observed isometric strength symmetry, could impact movement quality and elevate the risk of secondary injuries.41–45
Despite these considerations, this study’s findings support the practice among sports medicine professionals of using the uninvolved limb as an appropriate benchmark for assessing and monitoring strength deficits in individuals with a history of an ACL injury who have resumed unrestricted activities.
Limitations and Strengths
Several limitations to this study should be noted. First, only the uninvolved limb in those with a history of an ACL injury was tested as that was the protocol at the time of testing. Therefore, while there is no specific information about the involved limb, the findings of this study does support that the UNINV limb is not weaker than the dominant limb of healthy controls.
Second, while participants were all cleared to return to unrestricted activity at the time of enrollment, the time interval between injury and testing was not standardized. Previous research has shown that the muscle strength comparison between previously injured individuals and healthy controls may differ in terms of symmetry depending on the timing of testing, with most strength values being asymmetrical early and then normalizing around seven months.8,11,19 With most athletes being given clearance to return to activity between 6-12 months,62–64 the majority of those in this study’s ACL-I group are most likely greater than seven months post-injury meaning that their strength may have normalized to that of healthy controls. The exact timing of when the muscular strength becomes symmetrical should be explored in future research.
Third, for those participants with an ACLR, the graft type was not specified, thus limiting the ability to determine if graft type may influence the appropriateness of using the UNINV limb after an ACL injury as the benchmark for comparison of muscular strength and symmetry. However, previous research has suggested that muscle strength differences between graft types may only be clinically relevant during the early phases of rehabilitation after ACLR.65 Since this study’s patient population was in the later phases and cleared to return to unrestrictive activity, this limitation may not be significant.
Fourth, the participants examined in this study were first-year military cadets at different academies. As such, they may have greater physical fitness and/or motivation compared to a typical population.
Fifth, the strength symmetry between the UNINV limb in those with a history of ACL injury and the DOM limb in those with no prior ACL injury may only be specific to the type of muscle strength testing and the muscle testing positions used in this study. It is unclear if similar findings would be observed in different testing positions or under different testing conditions, such as concentric or eccentric contractions during isokinetic testing or when assessing different strength parameters such as peak force or rate of force development.
Finally, while this study supports using the UNINV limb in those with a history of an ACL injury as a surrogate for the DOM limb of healthy controls, it does not provide information on all the lower extremity muscles such as the soleus or adductors, or the absolute magnitude of muscular strength or strength symmetry required for reducing secondary injury risk. Although potentially not clinically significant, the implications of the observed small differences in muscular strength, particularly during injury mechanisms in the context of reinjury or contralateral injury risk, deserve focused attention in future research endeavors. Future studies should address these identified gaps.
Despite these limitations, the current study contributes valuable insights into the muscular strength of individuals with a history of ACL injury, particularly after clearance to return to unrestricted activity. By supporting the use of the UNINV limb as a surrogate for the DOM limb of healthy controls, these findings offer a practical benchmark for clinicians. The large sample size, including both males and females and ACL-injured and healthy individuals, enhances the robustness and applicability of the results. Moreover, the comprehensive examination of various lower extremity muscles provides a foundation for future research to build upon, addressing several research gaps identified in this study.
CONCLUSION
In this investigation, there was no conclusive evidence of reduced muscular strength in the uninvolved (UNINV) limb in those with a history of ACL injury compared to the dominant (DOM) limb in those with no prior ACL injury, regardless of sex. Despite detecting a slight increase in muscular strength in three of the six muscle groups of the UNINV limb in individuals with a history of an ACL injury compared to the DOM limb of healthy controls, the small effect sizes (d < 0.25) caution against overemphasizing these differences as clinically significant. These findings suggest that after an individual with a history of ACL injury has been cleared for unrestrictive activities, using the uninvolved limb as a standard for comparison for sufficient strength, such as when using the LSI, appears appropriate. This study shows that isometric muscle strength values in the uninvolved limb of individuals with ACL injury are equivalent or stronger than those of the dominant limb in individuals with no prior ACL injury, supporting the use of the uninvolved limb as a reliable benchmark for assessing muscular strength in those with a history of ACL injury.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
Thank you to all that made the JUMP-ACL testing possible.