INTRODUCTION
It has been well documented that the female athlete is at an increased risk of sustaining knee injuries such as patellofemoral pain (PFP)1 and anterior cruciate ligament (ACL) ruptures.2,3 Currently, two biomechanical patterns have been linked to knee injury risk: dynamic knee valgus (DKV) (adduction and internal rotation of the hip, knee abduction and rotation of the tibia) and reduced knee flexion.2,4 Females have been shown to demonstrate more knee valgus, less knee flexion and more femoral adduction when performing ‘at risk’ activities such as landing or cutting which could predispose them to a higher risk of injury.5–8 A plethora of research has focused on the influence of the kinetic chain on lower extremity biomechanics, with much of the research focusing on the hip,9–12 but there is a growing body of evidence linking decreased ankle dorsiflexion range of motion (DFROM) to these ‘at risk’ movement patterns.13–19 These kinetic chain patterns can be identified as the top-down approach (hip and trunk) and the bottom-up approach (ankle).20
Decreased DFROM is a common problem among athletes, especially after LAS, that has been shown to affect sagittal plane movement which may result in compensatory frontal and transverse plane motion and loading, especially at the knee. Individuals with DFROM limitations have been shown to have greater knee flexion displacement, increase knee valgus and greater ground reaction forces during bilateral and unilateral squatting,21,22 landing tasks,16,23,24 and change of direction tasks25 which have been linked to an increase in injury risk, especially in the female athlete. Furthermore, females have been shown to be more one-leg dominant in comparison to males and are more likely to injure their non-dominant limb.26–28 Therefore, understanding the effect of sex and leg dominance on DFROM may be useful to help inform future sex-specific prevention and rehabilitation strategies. Currently, the plethora of research which has investigated the effect of sex, limb dominance and LAS history on DFROM has found no effect of sex on DFROM29–32 in a variety of different sports and levels. Miller at al.29 and Senanayake et al.32 report a significant effect of previous ankle injury on DFROM but did not provide analysis on sex differences and so there exists a gap in the current evidence which will be explored further in this study.
Unilateral restrictions in DFROM may lead to asymmetrical loading and result in interlimb asymmetries which may influence lower extremity biomechanics. Current evidence is conflicting regarding the extent of asymmetries in DFROM. It has been previously suggested that a threshold of 10-15% asymmetry may increase risk of injury but the literature to support this focusses on return to sport after ACL reconstruction.33 This has since been challenged and no clear evidence which supports asymmetry and increased risk of injury,34,35 Furthermore the use of an arbitrary asymmetry threshold has limitations and it has been argued that asymmetry should be based on the metric, task, population, and muscle group studied in order to be useful.36 It has also been suggested that practitioners should monitor magnitude (% difference between dominant and non-dominant limbs) alongside direction of asymmetry (whether dominant or non-dominant limb had the larger DFROM) over several testing sessions as these have been to vary considerably over several test sessions using the same test. However, where data has only been collected during one single testing session, an inter-participant threshold can be established to determine what can be considered as a true asymmetry.37 To date there is no known study which investigates sex differences and LAS history on DFROM asymmetry. Normative data from Hoch and McKeon38 report interlimb asymmetries of 1-2cm in 35 healthy participants and Rabin et al.39 found asymmetries of 10° in 23% of male military recruits. Arede et al.40 and Işın et al.41 report frequent asymmetries of over 10% in male soccer players but argue that differences occur due to the functional demands of the sport. However, in comparison, other authors have found no asymmetry in DFROM,42,43 but this could be due to methodological differences between the studies and how asymmetry has been calculated. There is a dearth of literature on DFROM asymmetry in the female athlete. As DFROM has been postulated as a predisposing factor to influence lower extremity biomechanics, an understanding of between limb differences in DFROM is required to determine population and task specific asymmetry thresholds for asymmetry. Therefore, the aims of this study were to 1) to determine the effect of sex, leg dominance and LAS history on DFROM, 2) to determine the effect of sex and LAS history on magnitude of DFROM symmetry and 3) to examine the association of sex on direction (whether dominant or non-dominant limb had the higher DFROM) of symmetry.
MATERIALS AND METHODS
Participants
One hundred and five participants (68 females, 37 females) from recreational multidirectional sports volunteered for the study. All participants self-reported to be physically active and were participating in at least one training session and one match per week. All participants provided written, informed consent in the spirit of the Helsinki Declaration. Prior to testing, all participants completed an injury history questionnaire to assess previous lateral ankle injury on each leg, and leg dominance. Dominant leg was defined as the preferred leg for kicking a ball44 and LAS history was defined as at least one episode of an ankle sprain.45 Participants were excluded if they had a history of lower extremity surgery, any health conditions that may have influenced foot and ankle function, or a previous history of lower extremity injury in the prior six months. The participants were instructed to maintain their regular training regimens but were told not to exercise 48 hours prior to the day of testing. Ethical clearance was obtained by the institutional ethics review panel.
Procedure
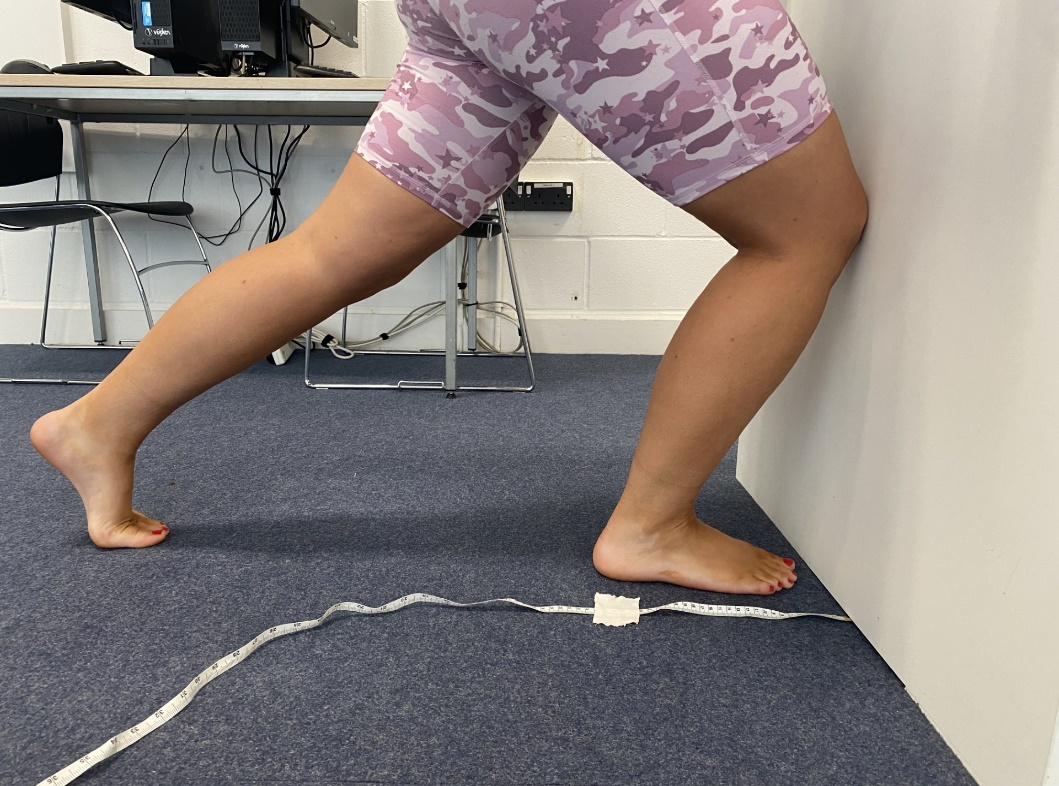
DFROM measurements were obtained using the weight bearing lunge test (WBLT) where the back foot (BF) heel was raised off the floor.46 This method has been shown to have excellent intra-rater reliability.46 Participants were instructed to position themselves in a tandem stance position in front of a wall. The big toe and midline of the heel of both feet were maintained perpendicular to the wall and each participant was instructed to keep the BF knee straight during each test position. Their BF heel was raised off the floor so that the participant was on their toes. Participants were asked to place their hands against the wall in front so that their hands were flat, and no gripping was allowed. Measurements were taken using a tape measure (to the nearest 0.1cm) from the big toe to the wall (Figure 1). Once participants were able to maintain the position with the knee touching the wall, the test foot was then progressed away from the wall in 1cm increments until their reach their maximum range of dorsiflexion.38 The examiner ensured that front heel contact was made throughout the testing using manual contact alongside verbal instructions but did not control either pronation or supination of the foot during testing. The BF was maintained in the same position throughout the test. No warmup was performed prior to testing and all testing took place in the same place using the same instruments by the same examiner to standardize testing conditions. The WBLT was completed three times for each leg and the mean of the three measurements was used for analysis. Leg order was randomly selected prior to the testing session.

Data Analysis
The mean of the three attempts were used for statistical analysis.47 For the first study aim, a three-way mixed ANOVA (IBM SPSS, version 29) was conducted to compare the effects of two between subject variables; lateral ankle sprain history (yes, no) sex (male or female) and a within subject’s variable: leg dominance (dominant or non-dominant) on DFROM. The assumption of normality for the data was checked using the Kolmogorov-Smirnov test with normative data obtained for all DFROM measurements (p>0.05). There was homogeneity of variances for dominant limb (p=0.90) and non-dominant limb (p=0.43) as assessed by the Levene’s test for equality of variances.
To determine interlimb asymmetry the calculation 100/(max value) x (min value) x -1 + 100 was used.48 To determine the direction of asymmetry (which ankle has higher DFROM) an ‘IF function’ was added to the end of the above formula: *IF(dominant <non-dominant,1,-1).49 An asymmetry threshold (AT%) was calculated for DFROM all participants and this was used to determine whether a participant can be considered as having a true asymmetry. This threshold was based on the population mean + smallest worthwhile change (SWC) using the calculation AT% = magnitude of asymmetry mean% + (0.2 x SD).50 The SD is the standard deviation of the mean magnitude of asymmetry. A high asymmetry threshold (HAT%) was calculated using population mean + (1.0 x between subject SD) for all participants.50 The assumption of normality for the data was checked for asymmetry data using the Kolmogorov Smirnov test and it was not normally distributed (p<0.05). There was homogeneity of variances as assessed by Levene’s test for equality of variances p=0.19). A two-way ANOVA was conducted to compare sex (male or female) and LAS history (yes or no) on magnitude of asymmetry (%). A Chi Square test of independence was conducted to determine whether there was an association between sex and direction of asymmetry.
RESULTS
One hundred and five participants (68 males, 37 females, age:27.8 ± 7.7 y, stature:175.5±9.4 cm, body mass:84.2± 17.4 kg, R dominant: n=92, L dominant: n=13) participated in the study. The descriptive statistics for all measurements for both dominant and non-dominant limb are presented in Table 1. Ninety-two (87.6%) participants (57 males, 35 females) reported their right leg to be their dominant leg while 13 (12.4%) participants (11 males, 2 females) reported their left leg to be the dominant leg. Seventy (66.6%) of participants reported a history of LAS in comparison to 35 (33.3%) of participants who reported no history of LAS.
There was no interaction between sex, LAS history, and leg dominance on DFROM (F(1,101) = 0.21, p = 0.65, η2 = 0.00) and no 2-way interactions between sex and leg dominance (p=0.82, η2=0.00), leg dominance and LAS history (p=0.94, η2= 0.00), or sex and LAS history (p=0.33, η2= 0.01). Significant main effects were found for sex (p=0.04, η2=0.43) and LAS history (p=<0.00, η2=0.10). No significant main effects were found for leg dominance (p=0.66, η2=0.00).
Magnitude of asymmetry values (%) are shown in Table 2. There was no interaction between sex and LAS history on magnitude of asymmetry F(1, 101)= .03, p=0.88, η2=0.00) and no main effects were found for sex (p=0.25, η2=0.00) or LAS history (p=0.82, η2=0.00).
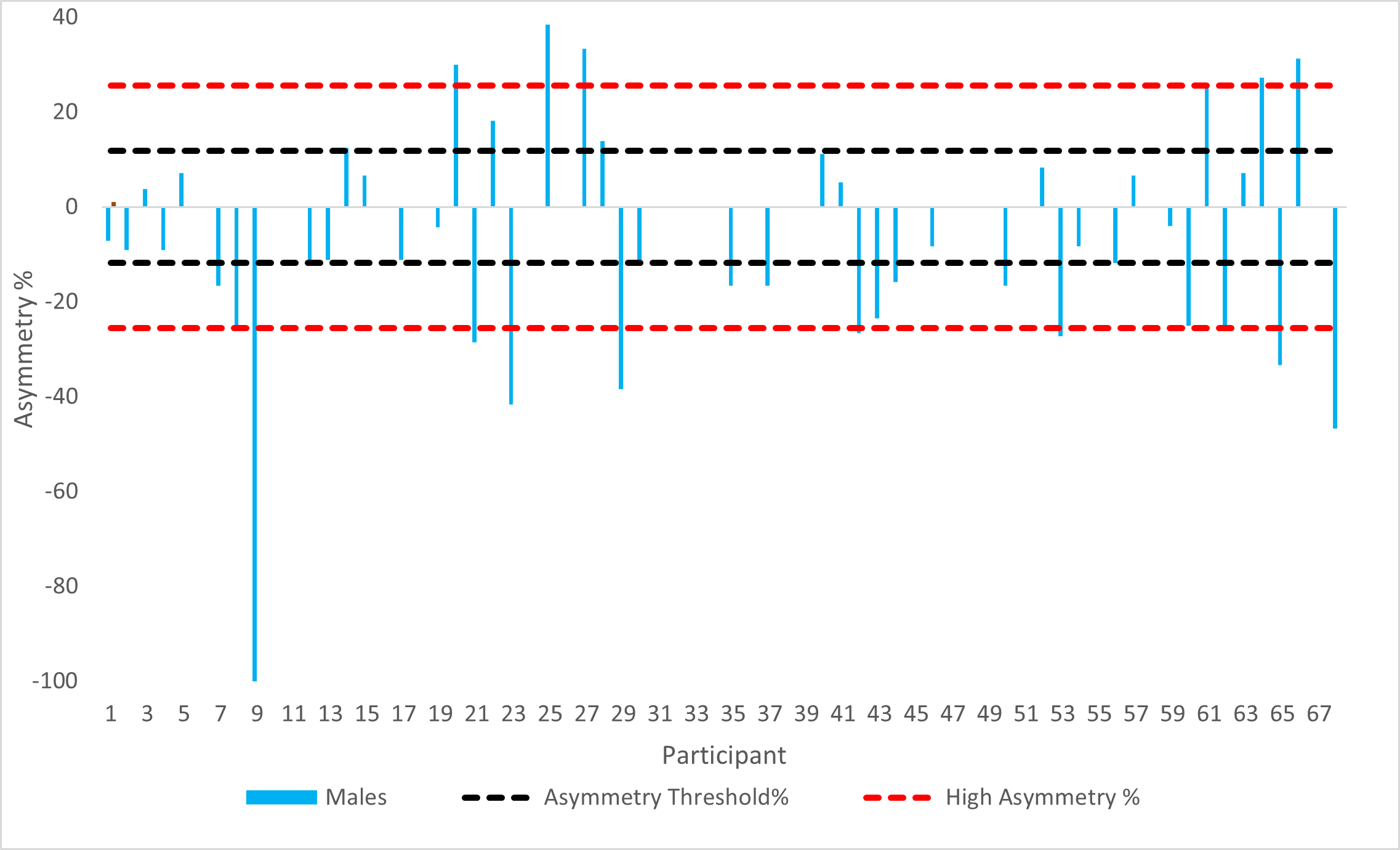
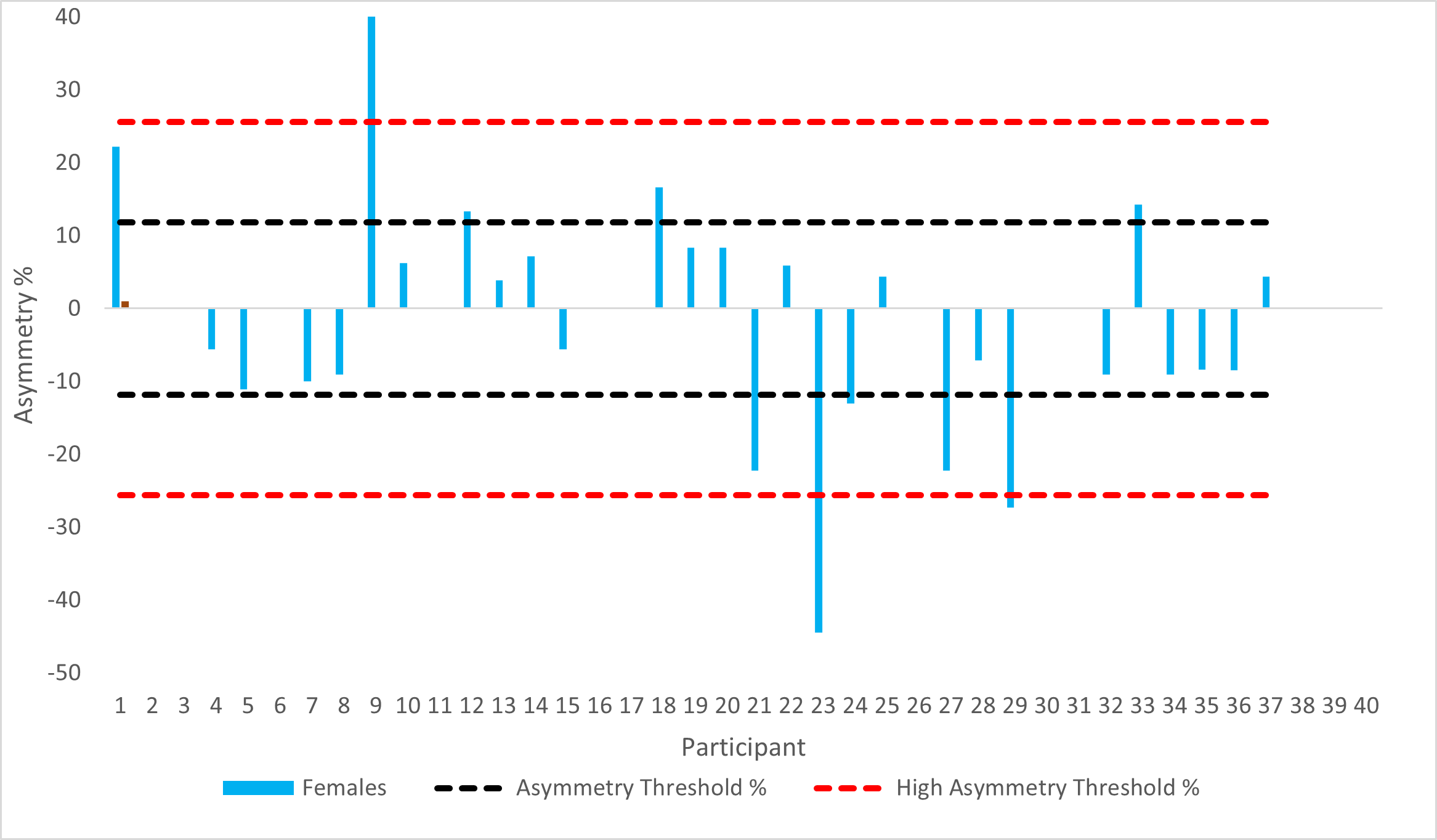
The asymmetry threshold was calculated as 11.8%. Twenty-six (24.7%) males (11 males LAS history, 15 no LAS history) 10 (9.5%) females (7 LAS history, 3 no LAS history) exhibited DFROM asymmetry magnitudes above the AT%. The HAT% was calculated as 25.6%. Twelve (11.4%) of males (6 LAS history, 6 no LAS history) and 3 (2.8%) females (2 LAS history, 1 no LAS history) exhibited asymmetry above the HAT%.

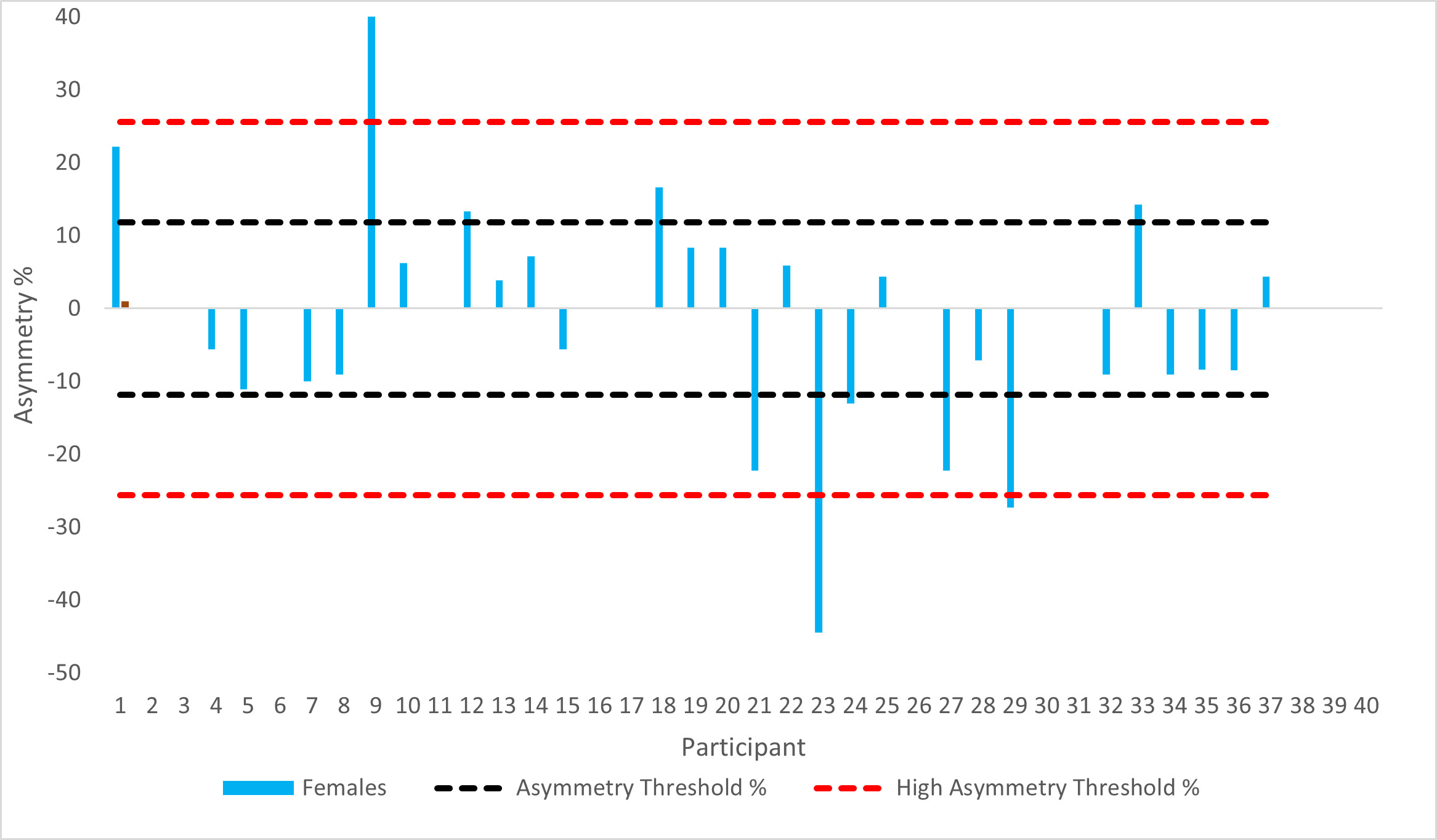
A chi-square test for independence was conducted between sex and direction of asymmetry (positive or negative). There were statistically significant association between sex and whether asymmetry favoured the dominant or non-dominant limb (χ2(1) = 11.26, p = .00). Sixty-five-point two percent of males were shown to have higher DFROM in their non-dominant limb compared to 75% of females who were shown to have higher DFROM in their dominant limb.
DISCUSSION
No statistically significant interactions existed between sex, leg dominance and LAS history and DFROM (F(1,101) = 0.21, p = 0.65, η2 = 0.00). Furthermore, there were no significant interactions found for sex and LAS history and DFROM, however, significant main effects were reported individually for sex (p=0.04, η2=0.43) and LAS history (p=0.00, η2=0.10) on DFROM. As this is the first known study to investigate the effect of sex, LAS history, and leg dominance on DFROM using the WBLT, these results cannot be compared to any previous published findings. The significant main effect of sex suggests that males demonstrated less DFROM (9.82cm) than females (10.91cm). It has been argued that females are shown to exhibit greater range of motion (ROM) due to lower muscle stiffness that allows a higher tolerance of muscle stretch,51 however, the findings from this study contradict Miller et al.29 and Llurda-Almuzara30 who found no significant effect of sex on DFROM in a group of elite level gymnasts and soccer players respectively. Differences between the studies could be attributed to the population tested as the athletes in this study were all recreational athletes from a range of multidirectional sports compared to elite athletes from a specific sport. Decreased DFROM has been linked to changes in lower extremity biomechanics which may increase risk of injury of non-contact ACL injuries especially in the female athlete. This study reported a significant difference in DFROM between males and females which may suggest that males may be more at risk of developing lower extremity biomechanics that may predispose them to injury, however, the difference was reported as 1.09cm (males 9.82cm, females 10.91cm) and it is unclear whether this is clinically relevant. More research is required to understand whether sex specific thresholds exist for DFROM, and how they influence lower extremity biomechanics or predispose an athlete to an increased risk of injury.
The results of this study indicate a significant main effect of LAS history on DFROM with those athletes with a history of LAS demonstrating less DFROM (LAS history 9.48cm, no LAS history 11.25cm, p=0.00). This supports findings from Miller et al.29 who reported similar findings in elite level gymnasts. However, Denegar et al.52 found no differences in DFROM in those with LAS history, but DFROM was measured passively in the prone position using an inclinometer which has been shown to be less reliable. These findings suggest that those with previous LAS history have less DFROM which may predispose them injury. However, there is a need to understand what constitutes decreased DFROM and whether there is a specific DFROM or threshold of loss that may predispose an individual to adverse lower extremity biomechanics.
The results of this study indicated that sex or LAS did not affect magnitude of asymmetry for DFROM. The mean magnitude of asymmetry ranged from 13.3%-13.5% in males and 9.2% -10.4% in females (males: LAS history: 13.6%±18.2%, No LAS history: 13.3%±13.7%; Females: LAS history: 10.4%±11.9%; No LAS history: 9.2%±8.6%). Magnitude of asymmetry values reported in this study are much higher compared to Madruga–Parera et al.53 who reported asymmetry of 5.88% ± 3.42 and Gonzalo Skok et al25 who reported asymmetry 9.6% in fifteen youth elite male basketball players, however they are consistent with findings from Arede et al.40 and Işın et al.41 who reported magnitude of asymmetries over 10% in semi-professional male soccer players. Large SDs have been reported in this study which indicates a large inter-individual variation however, this is a common finding in most asymmetry related research and may explain why relationships between asymmetry and performance are often insignificant.54 The AT% for this study population of recreational athletes was calculated as 11.8%. Of the 105 athletes tested 28 (41.17%) of the males (16.17% LAS history and 22.05% no LAS history) and 13 (35.13%) of the females (27.02% LAS history and 8.10% no LAS history) exhibited DFROM asymmetries which exceeded the AT%. Furthermore, 12 (17.6%) males and only 3 (8.1%) females exhibited asymmetry values above HAT%. This suggests that symmetries are present in males and females and supports findings from Hoch and McKeon,38 Rabin et al.,39 Howe et al.,42 and Arede et al.40 who all reported differences in DFROM between dominant and non-dominant limbs in healthy populations. Therefore, clinicians should exercise caution when using bilateral comparisons during injury assessment. However, in the current study true asymmetries (above the AT% for that population) were only seen in 41.17% of males and 35.13% of females and high asymmetry in 17.6% of males and 8.1% of females. It is important to recognise that these values are only specific to this population for this specific testing period and should not be used as a threshold for other studies as asymmetry has been shown to be metric, population, and test specific.52 Furthermore, it is not known how DFROM asymmetry influences lower extremity biomechanics and more research is needed in this area.
An interesting finding of the current study is that there was a significant association between sex and direction of asymmetry (χ2(1) = 11.26, p = 0.00). Sixty-five-point two percent of males were shown to have higher DFROM in their non-dominant limb compared to 75% of females who were more likely to have higher ROM in their dominant limb. It has been argued that athletes should have greater DFROM in their non-dominant (stance) limb as this limb needs to provide stability and balance when cutting and landing which is needed in sports requiring frequent change of direction,40 but this needs to be explored further. It is not known how direction and magnitude of asymmetry affects lower extremity biomechanics during specific activities as previous research has only investigated performance measures.53 Females have been shown to favour one limb more than another (leg dominance) in sports compared to males who have been shown to have less reliance on one limb which may predispose them to injury risk,2 and several studies have found that females are a higher risk of injury of injuring their non-dominant limb which suggests that leg dominance is a factor.26–28
This study is not without its limitations, although a large sample size was used for this study (n=105), the athletes used were from a variety of different university and recreational level multidirectional sports which required changes of direction and athletes were participating at different levels. Previous research54–57 shows that asymmetry differs depending on both sport, level, task, and population studied and therefore it is not known whether these sex differences would be seen if the tested on one sport and from athletes participating at the same level. Furthermore, the data from this study was collected during one single data collection point and caution must be taken when interpreting this data as both magnitude and direction has been shown to vary considerably across several testing sessions. This study also did not measure the effect of DFROM asymmetry on a specific performance variable and so it is not known how asymmetries may influence a variety of difference sports specific activities.
CONCLUSION
The results of this study indicate no significant interaction between sex, leg dominance and LAS history on DFROM in university and recreational level athletes from a range of multidirectional sports. However, females were had significantly higher DFROM values compared to males. Furthermore, those with LAS history had less DFROM compared to those without. This study reported interlimb asymmetry, however this was not affected by sex or LAS history. There was a difference in association of sex on direction of asymmetry as females were shown to have direction in favor of their dominant limb compared to males which favored the non-dominant limb. Caution should be exercised in interpreting these results as thresholds for asymmetry are metric, population, and test specific. Future research would be useful to determine the sex differences in magnitude and direction of asymmetry in DFROM while performing specific sports specific maneuvers. Further investigations of sex differences in the magnitude and direction of asymmetry on lower extremity biomechanics may help inform sex specific rehabilitation and prevention strategies.
Conflict of interest
The authors report no conflict of interest.