







INTRODUCTION
Low back pain (LBP) is a widespread musculoskeletal condition that affects up to 80% of individuals throughout their lifetime.1 It is considered the most common disorder in gymnastics, football, volleyball, and tennis athletes, accounting for 20% of sports injuries involving the spine.2,3 LBP is typically categorized as mechanical, rheumatic, infectious, tumoral, or mental, with mechanical LBP being the most common, around 90% of cases.4 Various factors may contribute to LBP incidence, including age, smoking, genetics, weight (gain), improper weightlifting, nutritional disorders, decreased flexibility and hydration, acute injuries, chronic stress, and poor physical conditions.5,6
The evaluation of patients with LBP, including conducting functional evaluations, is crucial in the clinical field.7 Several tools are used to assess patients with LBP, such as the Back Pain Functional Score, Oswestry Disability Index (ODI), Numerical Rating Scale (NRS), Pain Self-Efficacy Questionnaire (PSEQ), Patient-specific Functional Scale (PSFS), and the Functional Movement Screen™ (FMS™).8
The FMS™ assesses movement patterns and identifies restrictions and compensations. The primary objective of the FMS™ is to evaluate an individual’s ability to perform various movements, including those related to flexibility, range of motion, muscle strength, coordination, balance, and proprioception. It consists of seven component movements; the deep squat, hurdle step, inline lunge, shoulder mobility, active straight leg raise, push-up, and rotational stability movements. Several of these movements are performed bilaterally and when tests are performed bilaterally, the lower of the two scores is used for analysis.The assessment is carried out through standardized verbal instructions and visual inspection. FMS™ scores are assigned based on task performance, including movement conditions with or without pain and symmetry.9,10 The score for each movement ranges from 0 to 3, with a total cumulative score ranging from 0 to 21 points.11,12 Lower scores (≤14) on the FMS™ indicate impaired functional movements associated with the potential for a higher risk of injury.13
The purpose of this systematic review and meta-analysis is to examine functional movement scores among patients with low back pain (LBP) and healthy subjects with no LBP and review the validity of the FMS™ tool for screening functional movement among LBP patients.
METHODOLOGY
This systematic review complied with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria.14
The systematic review and meta-analysis were conducted through a thorough literature search of PubMed, Medline, Ovid, Scopus, and Central research databases using the keywords Functional movement screen AND low back pain. Studies published from 2003 to 2023 were screened to select studies that matched the inclusion/ exclusion criteria. Furthermore, selected study references were reviewed manually to identify similar studies. Only studies that compared the FMS™ between patients with chronic LBP and healthy control subjects were incorporated in the meta-analysis.
Inclusion and exclusion criteria
Papers assessing functional movement among adult patients with LBP (>18 years old) with FMS™ and published from 2003 to 2023 were included. Studies published in languages other than English were excluded. Narrative reviews, systematic reviews, consensus reports, case reports, case series, duplicated studies, published before 2003, studies with insufficient data or findings regarding FMSTM score, studies with irrelevant findings, studies that used other functional movement tools or assessed patients with another type of pain, and studies for which full text was unavailable were also excluded. Only studies that compared the FMS™ between patients with chronic LBP and healthy control subjects were incorporated in the meta-analysis.
Screening and data extraction
First, title and abstract screening was performed by the authors. Relevant full-text papers and evaluated the research for inclusion criteria were examined by one author. After articles were selected for inclusion, data were extracted and entered in a Microsoft Excel spreadsheet. Extracted data included authors, year of publication, objective, study design, sample size, gender, age, intervention, assessment tool, results, and outcome. Further data for the meta-analyses included total FMS™ score, in addition to scores of the seven FMS™ composite tests were extracted from the articles included in this systematic review.
Risk-of-Bias Assessment
The risk of bias in the incorporated papers was evaluated using the Cochrane Risk of Bias 2 (ROB 2) tool. The ROB 2 tool offers a structured, standardized, and flexible approach to assessing the risk of bias in randomized trials and non-randomized studies of interventions.15 The tool assesses quality based on five major domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. Each domain has a set of signaling questions that inform the risk of bias judgment for that domain. Based on the responses to each domain, the options for a domain-level risk-of-bias judgment are ‘Low’, ‘High’, or ‘Unclear’ risk of bias. A total or overall risk of bias score for each article was not determined.
Statistical analysis
Review Manager, version 5.4 (The Cochrane Collaboration, Oxford, England) was used for data entry and analysis. The standard deviation (SD) of the means were estimated from CI limits or standard mean difference (if not provided). The size of the continuous outcomes effect was reported as standard mean difference (SMD), and the precision of effect size was also reported as a 95% confidence interval (CI). DerSimonian and Laird’s random-effects model was used to compute SMD.16 Cochrane Q tests and Leave one out (I²) statistics were used to evaluate the heterogeneity and inconsistency across the studies. Leave one out meta-analysis was used for sensitivity analysis to recognize that the overall effect (against which heterogeneity is measured) changes each time an influential study is excluded.17 Statistical significance was set at p < 0.01 for Cochrane Q tests. If a high heterogeneity was detected, a leave-one-out test (removing studies one by one) was performed.
RESULTS
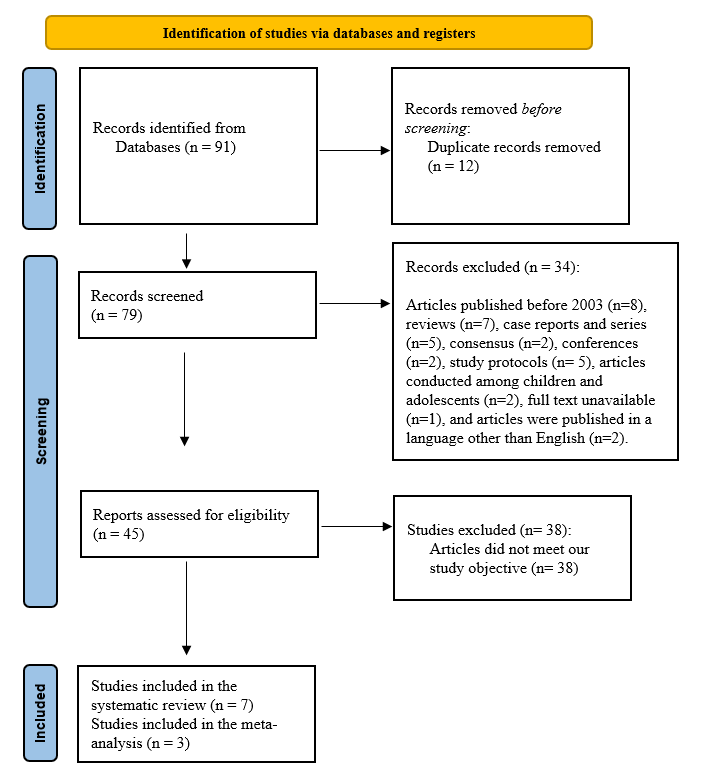
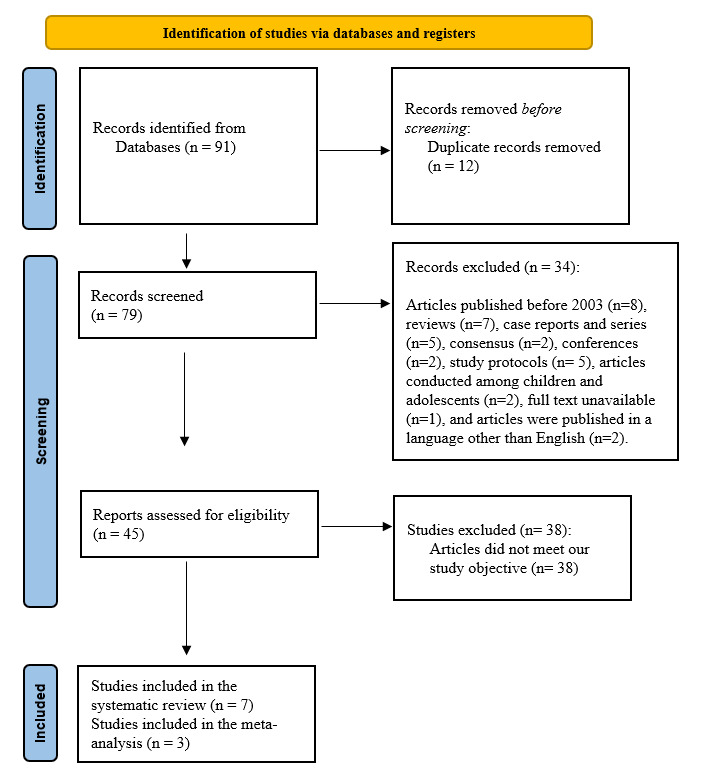
The initial search strategy provided 91 papers, of which 12 were omitted as duplicates. Regarding the remaining 79 articles, 34 were excluded because they did not match the inclusion criteria. Following screening and assessment, 38 additional articles were excluded because they did not match the study’s objective. Seven studies were considered suitable for and included in this systematic review (Figure 1).
Overview of the included studies
In terms of the seven included papers, all were published between 2016 and 2023 (Table 1). The articles included 272 adult subjects with an age range of 18-65 years old. The study subjects were patients with LBP, and either athletes, or healthy controls without LBP. The study design varied among the articles; one study was a double-blinded randomized clinical trial,18 one was a reliability and validity study,19 one was a cross-sectional study,20 and Four were prospective studies.7,21–23 Some studies included either males or females, and others included both genders. All included studies assessed LBP using the FMSTM, but one study also used the Numeric Pain Rating Scale (NPRS) and Oswestry Low Back Pain Disability Questionnaire (OSW).18 Only one study used intervention which included spinal stabilization exercises (SSEs) and general exercises (GEs).18
Overview of Studies’ Risk of Bias
Table 2 shows a representation of the risk of bias assessment.
Regarding sequence generation and allocation concealment, six studies had a low risk of bias and an unclear risk of bias. In blinding of participants and personnel and blinding of outcome assessment, two studies had a high risk of bias, one study had a low risk of bias, and four studies had an unclear risk of bias. Moreover, five studies showed an unclear risk of bias, and two studies had a high risk of bias regarding the incomplete outcome data section. All studies had a high risk of bias in the selective reporting section. However, regarding other sources of bias, five studies had a high risk of bias, while two had an unclear risk of bias. Overall, the included studies should be considered to have low to unclear risk of bias.
Meta-analysis results
FMS total score among LBP patients and control group
The total score of FMS™ among LBP patients and the control group was available in three papers (144 patients).7,19,21 The analysis revealed that the LBP group had a significantly lower total FMS™ score than the control group by 1.81 (95% CI (-3.02, -0.59), p=0.004). In addition, a significantly high heterogeneity was found (I2= 89%, p<0.001).

Individual FMSTM movement patterns
Three studies7,19,21 (144 patients) reported the scores of the seven FMS™ movement patterns between the patients with LBP and the control group. Of note, when tests are performed bilaterally (hurdle step, in line lunge, shoulder mobility, active straight leg raise, trunk stability push up, and rotary stability), the lower of the two scores is used for analysis, resulting in a single score for those tests.
Deep squat score
There was a significant difference between the patients with LBP control group scores with SMD -1.11 (95% CI (-1.59, -0.62), p< 0.00). Low heterogeneity was found (I2= 46%, p= 0.16).

Hurdle step score
The hurdle step mean score was significantly lower in the LBP group when compared to the control group by 1.41 (95% CI (-2.01, -0.81), p< 0.001). High heterogeneity was found (I2= 85%, p<0.001). A leave-one-out test was done, the Alhathaml et al. study was removed, and the heterogeneity became (I2= 45%, p= 0.18).

Inline lunge score
Regarding the inline lunge score, the patients with LBP had significantly lower scores than the control group, with SMD -0.41 (95% CI (- 0.74, -0.08), p=0.02). No heterogeneity was found (I2= 0%, p= 0.54).

Shoulder mobility score
There was a non-significant difference in the shoulder mobility score among LBP patients and the control group, with SMD -0.39 (95% CI (-1.03, 0.25), p=0.23). Significant heterogeneity was found (I2= 73%, p-value= 0.03). A leave-one-out test was done, the Khohroo et al. study was removed, and the heterogeneity became (I2= 0%, p=0.77), and SMD became -0.06 (95% CI (-0.49, 0.37), p= 0.78).

Active straight-leg raise scores
There was a significant difference between the LBP group and the controls, by SMD -0.75 (95% CI (-1.09, -0.41), p< 0.00). Furthermore, no heterogeneity was found (I2= 0%, p= 0.81).

Trunk Stability Push-up score
The LBP patients reported a significantly lower score in trunk stability push-up screening than the control by SMD -1.05 (95% CI (-1.88, -0.21), p=0.01). A significant high heterogeneity was found (I2= 81%, p=0.00). A leave-one-out test was done, the Khohroo et al. study was removed, and the heterogeneity became (I2= 0%, p=1.0), and SMD became -0.62 (95% CI (-1.06, -0.18), p= 0.00).

Rotatory stability score
Regarding rotatory stability, a significant difference was revealed between the scores of the patients with LBP and the control group with SMD -0.82 (95% CI (-1.56, -0.08), p=0.03). Significant heterogeneity was found (I2= 78%, p=0.01). A leave-one-out test was done, the Ko et al. study was removed, and the heterogeneity became (I2= 53%, p=0.14), and SMD became -0.48 (95% CI (-1.06, 0.09), p= 0.1).

DISCUSSION
Functional movement proficiency and examining movement patterns could demonstrate the foundation for lifelong physical activity. While the FMS™ is considered a fundamental screening tool for assessing functional movement, previous research has been primarily focused on the application of FMS™ among athletes.24 This is the first systematic review and meta-analysis using the FMS™ to compare the functional movement scores among adult patients with LBP and healthy subjects. In addition, this study reviews the validity of the FMS™ tool for screening the functional movement abilities of LBP patients.
FMS™ total score
The FMS™ is a commonly utilized screening tool for evaluating functional movement, supported by experimental research conducted and synthesized to date. This research encompasses diverse populations, including youth athletes and adults of both sexes.25,26
According to the screened studies in this systematic review, the mean total score of the FMS™ among LBP patients ranged from 10.95 to 14.1.7,19,21 The mean FMS™ scores for control groups ranged from 14.40 to 16.2. The meta-analysis found that LBP patients had a significantly lower total FMS™ score than the control group by 1.81 (p-value= 0.004). These findings support the literature and suggest that LBP patients generally exhibit lower functional movement capabilities than individuals without LBP, as evidenced by their lower FMS™ scores, supporting the validity of the screening tool. These lower scores are due to these FMSTM tasks being accompanied by lower or upper extremity movement, and some patients with LBP have difficulty in properly recruiting certain muscles, such as trunk stability muscles, and often display limited hip joint mobility. This could be reflected in lower scores seen in those with LBP on the deep squat, hurdle step, ASLR, and rotary stability movements.
Individual FMS™ movement patterns scores
Deep squat score
LBP patients often demonstrate limited range of hip mobility, which may induce compensation in the lumbopelvic region during lower limb movement. According to observations, individuals with and without LBP showed unique movement patterns during forward bending.27 This observation further supports the existence of a biomechanical correlation between low back disorders and the functioning of other joints during dynamic tasks. Activities involving manual material handling and lifting have been linked to LBP.28 Among the techniques associated with these activities is the squat technique, which involves lifting with flexed knees.29 Squatting is fundamental to routine activities such as sitting down and standing up.30
In the present meta-analysis, there was a profound difference between the LBP patients and the control group by -1.11 regarding the deep squat score in the FMS™ (p< 0.00). Furthermore, the scores of the LBP patients regarding the deep squat movements ranged from 1.26 to 1.9 out of 3, which was lower than the control group, which scored from 2.16 to 2.5 out of 3. Accordingly, these findings indicate that the FMS™ can detect the deficiency in the deep squat movement among LBP patients.
Hurdle step score
The hurdle step requires appropriate stability and coordination between the hips and torso during the stepping motion. It was revealed that individuals with CLBP would demonstrate deficiencies in this movement pattern.9
The meta-analysis results found that the mean score of hurdle steps in the FMS™ was significantly lower in the LBP group compared to the control group by 1.41 (p < 0.001). Moreover, the hurdle step scores among patients with LBP had lower scores (mostly less than 2 points) ranging from 1.7, 1.95, and 2.45 out of 3 points. In comparison, the scores among control individuals ranged from 2.16, 2.3, and 2.45 (more than 2 points) out of 3 points.
The low hurdle step scores that LBP patients received highlight how restricted hip and spine mobility which may occur in LBP patients may affect this movement. In addition, these findings reveal that FMS™ is an appropriate mechanism to assess the hurdle step among LBP patients.
Inline lunge score
The inline lunge test requires ankle, knee, and hip stability in the stepping leg and controlled closed kinetic chain hip flexion. Additionally, mobility is required in hip abduction, ankle dorsiflexion, and rectus femoris flexibility of the stepping leg.
Poor performance in this test can be caused due to various factors. First, there may not be enough hip mobility in the stance or step leg. Second, the knee or ankle stability in the stance leg may be insufficient while performing the lunge. Last, in one or both hips, an imbalance between relative adductor weakness and abductor tightness OR abductor weakness and adductor tightness might contribute to poor test performance.9
The meta-analysis of the incorporated papers found that the inline lunge score in FMS™ among patients with LBP patients was significantly lower than the control group by 0.41 (p=0.02). Despite the statistical difference between the two groups, the value of the difference in score is less than 1 which clinically could be very minute. Moreover, the scores of patients with LBP on the inline lunge were somewhat similar to the control subjects’ scores (1.83 to 2.5 versus 2.1 to 2.6, respectively).
Shoulder mobility scores
According to the included studies, there was no significant difference in the score of shoulder mobility among patients with LBP and the control group by -0.06 (p=0.78). However, the negative results mean the mean score of patients with LBP is lower than control group, no significant difference was found. Furthermore the included studies, patients with LBP scored similar or lower in the shoulder mobility movement than the control group.
Active straight-leg raise score
The straight leg raise test is widely used to assess the active hamstring and gastro-soleus flexibility while preserving stability in the torso.31 Sciatica is discomfort that radiates from the buttocks to the legs and is commonly associated with LBP.32 LBP is among the most common indications for the use of the straight leg raise test.33
According to the present findings, the patients with LBP reported a score ranging from 1.85 to 2.23 out of 3, while the control group scored 2.5 to 2.77 out of 3. Moreover, there was a significant difference between the LBP group and the control one, by SMD -0.75, favoring healthy control cases (p< 0.00). However, the difference between the two groups is very low, which clinically could be very minute and may not impact the ability to distinguish adults with LBP from those without LBP.
Push-up score
The push-up movement test is commonly used to investigate upper-limb muscular fitness, especially among young people.33.34 Low fitness in the trunk stability push-up test correlates with low back dysfunction and pain among middle-aged individuals.34
In this meta-analysis, the patients with LBP had lower push-up screening scores than the control scores by 1.05 (p=0.01). In the included studies, the LBP patients reported relatively low scores in the push-up screening, ranging from 0.83 to 1.3 out of 3. Low fitness in the modified push-up test has been associated with poor perceived health, low back dysfunction, and pain among middle-aged subjects. Also, poor endurance in the back musculature has been reported to be a risk factor for LBP.35
Rotatory stability score
The rotatory stability test is performed with either lower or upper extremity movement. Shoulder flexion stimulates anterior displacement of the center of mass, placing greater demands on the trunk muscles to keep the center of mass over the base of support. Thus, trunk stability is required to sustain a neutral position. It was revealed that LBP patients have burdens that require proper recruitment of the trunk stability muscles before moving the limbs.5 Thus, compensation may occur among LBP patients during rotary stability tests due to inappropriate recruitment of the trunk stability muscles. This may lead to lower scores among LBP patients compared to healthy individuals.35–37
In this meta-analysis, there was a significant difference between the scores of the patients with LBP and the control groups by 0.82 (p-value= 0.03). However, this difference between the two groups is less than 1, which clinically could be very minute.
Limitations
This systematic review is limited to the few included studies that compare FMS™ among patients with LBP control groups. Furthermore, the review primarily focuses on adult subjects, and the generalizability of the findings to other populations, such as highly competitive and youth athletes, may be limited. Additionally, the review does not consider potential confounding factors such as pain or the influence of specific interventions or treatments on FMS™ scores. Further research is needed to assess the association of cofounders, such as age, gender, and body mass index, with the FMS™ score among LBP patients and the control group.
CONCLUSION
Low to unclear risk of bias studies included in this systematic review and meta-analysis provide valuable insights for clinicians and healthcare professionals while evaluating and treating patients with LBP. Lower scores on the FMS™ tool are associated with impaired functional movement and increased injury risk among LBP patients. Further well-designed research may be more specific in the targeted population and include FMS™ in LBP within one of its various subcategories, such as acute, chronic, and non-specific cases.
Acknowledgment
The authors would like to thank the Deanship of Scientific Research at Shaqra University for supporting this work.
Conflict of interest
All authors report no conflicts of interest.