
INTRODUCTION
Stretching programs typically focus on mechanically increasing the extensibility of the target tissue through deformation (i.e., plastic and viscoelastic), increased sarcomeres in series, neuromuscular relaxation, or modification of sensory perception.1 The use of active and passive stretching techniques may increase the stretch tolerance in patients rather than fostering a physiological change in the mechanical properties of the muscle.1–3 Despite the lack of evidence to support a permanent deformation of musculoskeletal tissue as a result of progressive stretching, clinicians frequently incorporate stretching as part of an injury prevention or rehabilitation protocol.4–7
The application of Proprioceptive Neuromuscular Facilitation (PNF), Static Stretching (SS), and Dynamic Stretching (DS) techniques are thought to influence the target tissue (e.g., hamstring musculature) extensibility. However, these techniques produce little effect on the musculoskeletal soft tissue restriction as the interventions may negatively influence adjacent structures or neighboring joint mobility. In the hamstring, for example, stretching programs designed to optimize muscle lengthening could alter or inhibit adjacent structures, such as lumbar or pelvic postural stabilizers, resulting in a perceived change in hamstring length.8 As a result, stretching protocols may produce limited mechanical lengthening at the site of tissue restriction, but instead increase range of motion (ROM) through a series of postural and motor control changes up and down the kinetic chain. Long-term stretching protocols have been shown to produce suboptimal movement patterns, structural malalignment and inhibit neuromuscular control, which develop in response to musculoskeletal imbalances and localized tissue adaptions.9–11
Conflicting evidence suggests that short-term or acute changes in hamstring extensibility using traditional stretching techniques are achievable but physiological elongation of the target tissue is unrealistic.3,4,12–15 Focusing on impairments from other body regions or systems, regardless of the proximity to the musculoskeletal dysfunction, rather than treating with a local intervention targeting the perceived impaired tissue produces a greater impact on the patient’s primary complaint.8,9 A novel treatment approach, such as Total Motion Release® (TMR®), which attempts to restore mobility of surrounding structures and reduce adjacent soft tissue restriction has demonstrated greater benefits than traditional stretching for improving ROM. Restoring movement symmetry of surrounding structures that influence target tissue to improve joint mobility, such as in a regional interdependence approach, could produce long-lasting benefits in restricted tissue.
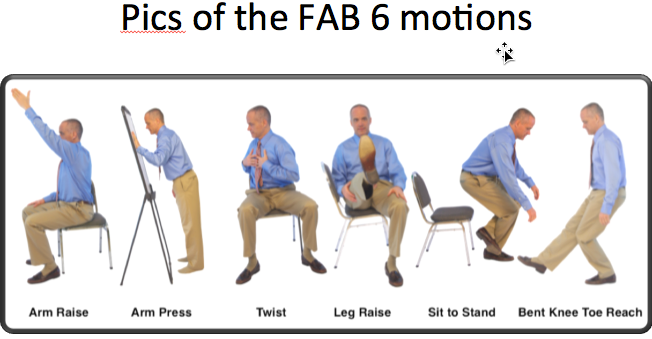
TMR® is a manual treatment technique developed by Tom Dalonzo-Baker which identifies body asymmetries to assess and treat dysfunction.16 The technique uses a regional interdependence approach to increase mobility and decrease pain and restriction within the musculoskeletal system.17 The Level one TMR® treatment technique includes a movement assessment which incorporates six bilateral movements (referred to as the “Fab 6”) performed across the upper body, trunk, and lower body (Figure 1).18 Following each movement, the patient rates the motion on a subjective scale from 1 (no dysfunction, pain, asymmetry) to 100 (complete dysfunction, pain, asymmetry).19 The upper body, trunk, and lower body motions with the greatest dysfunction are treated by repeating the TMR® Fab 6 movement using the patient’s “good side.” Recent research suggests that TMR® is effective in treating soft-tissue restriction of both the upper and lower extremities. Gamma et al19,20 demonstrated significant increases in shoulder internal and external rotation of healthy baseball pitchers using the TMR® trunk-twist and arm raise movements compared to a traditional static and dynamic warm-up. Baker et al.16 also demonstrated a significant increase of 31.5° bilaterally in the active straight leg raise (ASLR) following one week of TMR® combined with instrument assisted soft-tissue mobilization.

To date, no studies evaluating the efficacy of the TMR® Fab 6 protocol on lower extremity hamstring muscle extensibility could be identified. Therefore, the purpose of this exploratory observational study was to determine the effectiveness of the TMR® Fab 6 assessment and treatment to increase hamstring flexibility in healthy participants following one session of TMR®. The authors hypothesized that restoring movement symmetry utilizing the TMR® Fab 6 would result in a greater increase in hamstring flexibility as measured by the Active Knee Extension Test (AKET) and the Passive Straight Leg Raise Test (PSLR) when compared to a control group.
MATERIALS AND METHODS
Design
An observational study approach was used to evaluate independent group variables (i.e., TMR and control) and limb (i.e., preferred leg and non-preferred leg). The non-preferred leg was considered the extremity with the least amount of flexibility at baseline while the preferred leg was considered the extremity with the greatest amount of flexibility at baseline. This protocol was determined to be most appropriate because TMR® is designed to treat movement asymmetry throughout the body rather than target a specific tissue dysfunction. The terms “preferred” and “non-preferred” were used to avoid the need to operationalize dominance because, unlike the upper extremity, there is no consensus when defining lower extremity dominance. In some cases, lower extremity dominance is determined by asking the patient which leg they prefer to kick a ball.21 However, this definition assumes that the limb used to kick a ball would be the same as the limb with greatest strength, the limb used to “brake” after being pushed, the limb used to jump, and the limb used to spontaneously land following a step-up task.22 In addition, there has been no association found between self-identified preferred kicking leg and preferred landing leg in athletes and non-athletes, therefore, lower extremity dominance has no impact when analyzing movement asymmetries.21,23,24 The dependent variables were AKET range of motion and PSLR range of motion at baseline, post treatment, and 24 hour follow up.
Participants
A convenience sample of 20 healthy participants were recruited from three separate institutions (two colleges, one high school). All participants were high school or college athletes who remained physically active but had not engaged in an organized team or individual sport within the previous six months. Participants were randomly assigned to either the TMR® group or the control group.
Participants were excluded from the study if they had a history of hamstring pathology that prevented full knee or hip range of motion, a lumbo-pelvic pathology limitation which prohibited participation in the PSLR, ongoing musculoskeletal, neuromuscular or functional limitations, history of paresthesia, motor abnormality, a knee flexion angle greater than 70 degrees while performing the AKET, or if the participant was involved in a systematic stretching program within the last month. The institutional review board from each facility approved this study in the spirit of the Helsinki Declaration, and all participants provided written informed consent including minor participant assent and parental consent. Prior to baseline evaluation, all participants were asked to refrain from pre-activity warm-up or stretching within the two hours preceding assessment and treatment.
Assessments & Measurements
Total Motion Release® Fab 6 Treatment Group
The TMR® treatment group subjectively compared the Fab 6 movements bilaterally to determine the side and/or motion of greatest restriction. The six movements include: seated shoulder flexion or arm raise (AR), bent arm wall push-up or arm press (AP), seated trunk rotation (TR), seated hip flexion with knee extension or leg raise (LR), single leg sit to stand (STS) and unilateral standing toe touch (TT).18 Following each movement, a visual scoring scale (Table 1) was used to identify the “good side” (lower score) and “bad side” (higher score) related to participant reported pain, tightness, ROM, strength, and ease of motion. The most asymmetrical upper body movement (i.e., shoulder flexion or wall push-up), lower body movement (i.e., straight leg raise, toe touch, or sit-to-stand) and trunk movement (i.e., rotation right or rotation left) were selected and treated. A standard provocative movement (e.g., standing hip flexion) was also established to assess patient reported subjective hamstring restriction. The standard provocative movement was utilized throughout the testing procedure to assess the impact of the TMR® Fab 6 treatment on perceived hamstring tightness.
Control Group
The control group performed the same baseline testing and standard provocative movement (standing hip flexion). Following intake and ROM measurements, participants were instructed to perform one repetition of standing active hip flexion with both knees in full extension, held for 2 seconds and repeated every 30 seconds for 15 minutes. The sham treatment was created to ensure a temperature increase in the target tissue and provide results similar to a dynamic warm-up.
Clinical tests
Active Knee Extension Test. The AKET was performed with the participant in a supine position inside a homemade AKET device (Figure 2) with the non-test leg secured to the table in a pelvic neutral position using a mobilization belt across the mid-portion of the anterior thigh. The TiltMeter smartphone app (Carlos Hernandez) was placed on the participant’s anterior thigh, 10 cm proximal to the superior pole of the patella of the tested leg. The participant’s thigh was passively flexed to 90 degrees and maintained in that position using the horizontal bar of the homemade AKET device.25 The participant was then asked to actively extend the knee until reaching the maximal tolerable stretch of the hamstring muscles.26,27 The examiner placed the TiltMeter smartphone app on the anterior tibia halfway between the inferior pole of the patella and distal tibia with the screen facing away from midline to blind the participant.26 Measurements were recorded as the distance from 180 degrees of knee extension. Prior to data collection, interrater reliability was established using a sample of 11 healthy participants independently recruited for this portion of the study. Interrater reliability assessment for AKET and PSLR was assessed using a two-way mixed intraclass correlation coefficient (ICC3,1). Active knee extension testing was reliable between raters for the right leg (ICC3,1 = 0.952, p<.0001, 95% CI: 0.90, 0.99, SEM 3.32) and the left leg AKET (ICC3,1 = 0.97 (p<0.001, 95% CI: 0.93, 0.99, SEM 3.06) for the three raters. Interrater reliability results are consistent with other researchers who found an ICC2,1 value of 0.93 for the AKET.28 Reliability for each rater was also assessed, and also indicated excellent intra-rater reliability with values ranging from 0.94-0.97 (p<.0001, 95%CI: 0.74, 0.99). Standard error of measurement (SEM=SD* √ 1-test reliability) was calculated for test-retest reliability of the AKET with measurements ranging from 1.50-3.72.

Passive Straight Leg Raise Test. Hip flexion was assessed bilaterally using the PSLR test. The participant was positioned supine with both legs extended and the non-test leg secured to the table in a pelvic neutral position using a mobilization belt across the mid-portion of the anterior thigh. Participants were also instructed to relax the ankle in a slightly plantarflexed position.25 The TiltMeter smartphone app was placed on the anterior tibia halfway between the inferior pole of the patella and the distal tibia with the screen facing away from the midline to blind the participant. The hip was passively flexed until the participant identified a strong but tolerable stretch in the hamstring and measurements were recorded. A reliability testing session revealed that interrater reliability for the passive straight leg raise test was excellent for the right leg (ICC3,1 = 0.97, p<0.001, 95%CI: 0.93, 0.99, SEM 2.58) and the left leg PSLR (ICC3,1 = 0.98, p<0.001, 95% CI: 0.96, 0.99, SEM 2.27), which was consistent with the existing literature.28 Intrarater reliability was found to be 0.94-0.97 (p<.0001, 95%CI: 0.70, 0.99) for the PSLR across the three raters. Lastly, standard error of measurement was calculated for PSLR test-retest reliability, which ranged from 1.74-3.45.
TMR® Treatment Group
The TMR® treatment group utilized the “good side,” performing the unilateral motion described during the FAB 6 evaluation. Of the three previously identified body regions (e.g., upper body, lower body and trunk twist), the most asymmetrical movement was performed first by having the participant complete two sets of 10 repetitions (one round) of an isotonic motion to the end range. For example, if shoulder flexion was considered the most asymmetrical motion, the participant performed 2 sets of 10 repetitions of shoulder flexion to the end range using the “good side” with 30-seconds rest between sets. Following the first round, the participant was instructed to retest the same movement (e.g., shoulder flexion) on the “bad side” and re-score on the visual scoring scale. At this time, the participant also retested and rescored bilateral standing hip flexion (provocative motion) to establish if the previously identified hamstring restriction had changed. Traditional TMR® protocol governed the progression of TMR® following round one, but the rules were modified for subsequent rounds to establish consistency across three examiners (Table 2). Rounds of the identified TMR® movement continued based on the the established rules matrix until the participant identified a 5 or less on the visual scoring scale before moving on to the next body region. This process continued until a score of 5 or less was recorded in all three body regions.
Procedures
Participant intake and baseline evaluation were completed and included a medical history to verify exclusion criteria along with demographic information. After intake, each participant performed a 5-minute warm-up on the stationary bike at a moderate intensity (80-90 RPMs) followed immediately by the bilateral ROM evaluations on the right and left lower extremities in order from AKET to PSLR. Following baseline measurements, participants were randomly placed in the TMR® group or the control group. Upon completion of treatment, control and TMR® intervention groups were immediately re-evaluated using the AKET and the PSLR in the same order and fashion as baseline testing. Participants were asked to return in 24-hours for the same objective measurements as previously described. All participants were instructed to refrain from supplemental stretching and physical activity in which the heart rate was elevated for more than 15-minutes over the 24-hour period.
Statistical Analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS, Inc., Armonk, NY, USA) version 23.0. The results are expressed as mean ± standard deviation. Normality of distribution and equality of variance were assessed using Levene’s test. An independent samples t-test was used to assess group differences at baseline on the AKET and PLSR. A mixed-model ANOVA, with one between (group) and one within (time) factor, was used to determine any main effects, using the multivariate criterion of Wilks’ Lambda (λ), or interactions across time for each outcome measure across groups. The alpha level was set a priori at p< 0.05 for all analyses. If a significant ANOVA was found, an independent t-test was used to compare the changes between groups across the time points (e.g., baseline to post-intervention, post-intervention to 24hr follow-up, and baseline to 24hr follow-up). Post-hoc t-tests were corrected for type I error using the Bonferroni technique (αadjusted = .05/3) and the adjusted alpha level was set a priori at p ≤ .017. Effect size was calculated using Cohen’s d ([M1 – M2] /standard deviation(pooled)) and a large effect size was set a priori at d ≥ .08.29
RESULTS
Preliminary Data Analysis
A total of 20 participants (10 males and 10 females, mean age = 17.8±1.2 years, mean height = 175.0±10.2 cm, mean weight = 74.5±17.1 kg) were included, all met study criteria and completed all testing portions of the study. Significant differences between groups were not found on the demographic variables after group allocation (Table 3). Significant group differences between groups were also not found on baseline performances of the AKET or PSLR on either the PL or NPL (Table 3). ROM across all three timepoints between groups can be found in Table 4.
Active Knee Extension Test Analysis of the Non-Preferred Leg
A significant difference for time (F2,17 = 179.91, p ≤ 0.001, partialƞ2 = .955, power = 1.0) and time by group interaction (F2,17 = 57.38, p ≤ 0.001, partialƞ2 = .871, power = 1.0) were found in the AKET on the non-preferred leg. Immediately following the intervention, the TMR® group (mean change = 12.15° ± 2.94) experienced an improvement on the AKET that was significantly better (mean difference = 5.00°, p ≤ 0.001, Cohen’s d = 2.12, 95% CI 2.78, 7.22) than the improvement experienced by the control group (mean change = 7.15° ± 1.56). From the post-treatment measure to the 24hr follow-up measure, the TMR group (mean change = -2.85° ± 1.36) maintained significantly more (mean difference = 3.90°, p ≤ 0.001, Cohen’s d = 2.74, 95% CI 0.63, 2.57) of the improvement than the control group (mean change = -6.75° ± 1.48). From the baseline measure to the 24hr follow-up measure, the TMR group (mean change = 9.30° ± 2.10) displayed significantly improved (mean difference = 8.90°, p ≤ 0.001, Cohen’s d = 4.36, 95% CI 6.98, 10.81) AKET values compared to the control group (mean change = 0.40° ± 1.98).
Active Knee Extension Test Analysis of the Preferred Leg
A significant difference for time (F2,17 = 154.60, p ≤ 0.001, partialƞ2 = .948, power = 1.0) and time by group interaction (F2,17 = 20.14, p ≤ 0.001, partialƞ2 = .703, power = 1.0) were found in the AKET on the PL. Immediately following the intervention, the TMR group (mean change 12.15° ± 3.05) experienced an improvement on the AKET that was significantly better (mean difference 4.15°, p ≤ 0.002, Cohen’s d = 1.61, 95% CI 1.72, 6.57) than the improvement experienced by the control group (mean change = 8.00° ± 2.00). From post-treatment measure to 24hr follow-up measure, the TMR group (mean change = -3.45° ± 1.61) maintained significantly more (mean difference = 4.45 p ≤ 0.001, Cohen’s d = 1.77, 95% CI 2.09, 6.81) of the improvement than the control group (man change = -7.90° ± 3.16). From baseline measure to 24hr follow-up measure, the TMR group (mean change = 8.70° ± 3.62) displayed significantly improved (mean difference = 8.60°, p ≤ 0.001, Cohen’s d = 2.94, 95% CI 5.82, 11.37) AKET values compared to the control group (mean change = 0.10° ± 2.07).
Passive Straight Leg Raise Analysis of the Non-Preferred Leg
A significant difference for time (F2,17 = 112.86, p ≤ 0.001, partialƞ2 = .930, power = 1.0) and time by group interaction (F2,17 = 33.21, p ≤ 0.001, partialƞ2 = .797, power = 1.0) were found in the PSLR on the non-preferred leg. Immediately following the intervention, the TMR group (mean change = 12.95° ± 3.10) experienced an improvement on the PSLR that was significantly better (mean difference = 6.95°, p ≤ 0.001, Cohen’s d = 2.53, 95% CI 4.37, 9.53) than the improvement experienced by the control group (mean change = 6.00° ± 2.33). From the post-treatment measure to the 24hr follow-up measure, the TMR group (mean change = -2.70° ± 1.03) maintained significantly more (mean difference = 2.35°, p ≤ 0.001, Cohen’s d = 1.09, 95% CI 0.32, 4.37) of the improvement than the control group (mean change = -5.05° ± 2.87). From the baseline measure to the 24hr follow-up measure, the TMR group (mean change = 10.25° ± 2.97) displayed significantly improved (mean difference = 9.30, p ≤ 0.001, Cohen’s d = 3.76, 95% CI 6.97, 11.62) PSLR values compared to the control group (mean change = 0.95° ± 1.85).
Passive Straight Leg Raise Analysis of the Preferred Leg
A significant difference for time (F2,17 = 85.11, p ≤ 0.001, partialƞ2 = .909, power = 1.0) and time by group interaction (F2,17 = 27.11, p ≤ 0.001, partialƞ2 = .761, power = 1.0) were found in the PSLR on the PL. Immediately following the intervention, the TMR group (mean change = 13.70° ± 3.38) experienced an improvement on the PSLR that was significantly better (mean difference = 8.60°, p ≤ 0.001, Cohen’s d = 2.70, 95% CI 5.60, 11.60) than the improvement experienced by the control group (mean change = 5.10° ± 2.98). From post-treatment measure to 24hr follow-up measure, the TMR group (mean change = -3.80° ± 2.31) maintained more (mean difference = 2.35°, p ≤ 0.090, Cohen’s d = 0.80, 95% CI -0.40, 5.10) of the improvement than the control group (mean change = -6.15° ± 3.44) but this difference was not statistically significant. From baseline measure to 24hr follow-up measure, the TMR group (mean change = 9.90° ± 4.43) displayed significantly improved (mean difference = 10.95°, p ≤ 0.001, Cohen’s d = 2.63, 95% CI 7.79, 14.11) PSLR values compared to the control group (mean change = -1.05° ± 1.72).
DISCUSSION
The purpose of this study was to determine the effect of a single bout of the TMR® Fab 6 assessment and treatment to increase hamstring flexibility in healthy participants as measured by the AKET and PSLR tests. The results suggest that both the control group and the TMR® group demonstrated immediate post-intervention change in hamstring flexibility, however, the increase experienced by the TMR® group was significantly greater than the change experienced by the control group. Further, only the TMR® group experienced a significant change in flexibility over the 24-hour period, denoting the application of TMR® was more effective at producing longer lasting improvements. The large effect sizes (i.e., Cohen’s d) reported across all measures of AKET and PSLR demonstrates a practical significance denoting increased confidence that the difference between the TMR® and control groups is meaningful to clinicians. The results of this exploratory observational study indicate the use of TMR® is more effective for acutely improving measures of hamstring flexibility and maintaining those changes at a 24-hour follow-up than the control group. The magnitude of difference between the TMR® and control groups suggests that a regionally interdependent approach to the treatment of restricted tissue leads to better patient outcomes.
Among researchers, a consensus has not been established for the most effective and efficient method to increase hamstring flexibility. Both PNF and SS have been shown to significantly increase ROM.12,30–33 but the lasting effect of these techniques remains inconclusive.4,34 Depino et al.,34 utilized a standing static hamstring stretching protocol and evaluated ROM using the AKET and found a significant increase in hamstring extensibility at one- and three-minutes post intervention but returned to baseline after six minutes. In contrast, DeWeijer et al.4 used static stretching with and without an active warm-up and saw a significant increase in AKET ROM which was maintained for a 24-hour period. Unlike traditional stretching methods which produce a positional sensitivity in the golgi tendon organs by affecting the series elastic component of the muscle,4 TMR® promotes the restoration of symmetry and a reduction in restriction throughout the body, resulting in more efficient movement. The current results benefit from a regional interdependence-informed treatment protocol which may produce changes in the passive mechanical properties of the hamstring without intentionally attempting to lengthen the target tissue. It should be acknowledged that recent literature has questioned the impact of asymmetry on movement dysfunction hypothesizing that asymmetry may not be clinically relevant and is considered a normal part of human structure and function.35,36 Treatment paradigms that target bilateral asymmetries may have little to no effect on sport performance or reduction of injury.35
Findings of the present study support previous investigations using the TMR® treatment protocol for increasing ROM. Gamma et al.19,20 found significant increases in shoulder internal and external ROM in baseball players when comparing the TMR® trunk twist and arm raise to a traditional baseball warm-up. Similarly, Dexter et al.37 observed significant increases in internal and external hip ROM in overhead athletes utilizing the TMR forward flexion trunk twist combined with the seated straight leg raise. Unlike the previous TMR® research, the treatment protocol used in the current study involved the application of TMR® across all three sections of the body (i.e., upper extremity, trunk/core, and lower extremity). The authors conclude that the application of the TMR® protocol may only need to occur at the areas of the body with the greatest movement impairment and dysfunction. Additionally, the current results, when combined with previous TMR® research, indicate that statistically significant increases in ROM are possible without the need for utilizing an intervention (e.g., stretching) that targets “tight” tissue to improve flexibility and ROM. Thus, changes in hip ROM and hamstring extensibility may be attributed to a reduction of restriction throughout the entire body as opposed to being the result of “tight” or “shortened” muscles that need to be stretched.
Previous researchers have speculated that the positive effects of TMR® may be attributed to neuro-physiological adaptions associated with the increase motor output from spinal neurons.16,37,38 Mechanisms such as neural coupling39 and cross education40 influence the fascial and muscular tissue via integrated central and peripheral nervous system feedback, promoting accommodations in joint ROM and muscular flexibility.37 Using a treatment paradigm focused on the “good” side has been shown to produce bilateral improvements while avoiding the need to increase tension on a target muscle or reinforce a dysfunctional pattern.41
Limitations are present for generalizing the results outside of the study population. Because the research design included only healthy subjects with a mean age of 17.8±1.2 years of age, the results of the current study may not be observed in individuals with hamstring or lumbar pathology, or those who are outside of this age range. Similarly, there are numerous stretching techniques and we only compared the TMR® application to the control group. Additionally, the authors did not collect more long-term follow-up measurements (e.g., 72 hours) or assess other functional measures (e.g., Functional Movement Screen™, EMG analysis) to determine the long-term results of application or examine potential mechanisms of action for the effect of the TMR® protocol.
Future research should examine the use of TMR® as a soft-tissue treatment protocol and compare it to the use of other common stretching techniques (e.g., SS, PNF stretching) utilized by practicing clinicians to improve hamstring extensibility and ROM. The long-term benefits of TMR®, as well as the effects of TMR® on other soft tissue restrictions throughout the body, should be considered in future research. It may also be beneficial to assess the effects of multiple TMR® treatment applications, as well as collect other variables (e.g., EMG data) to assess the potential mechanism of action and determine overall effectiveness of TMR® as a therapeutic intervention.
CONCLUSION
The results of the current study demonstrate that a single bout of TMR® using one identified lower extremity, one upper extremity, and a trunk twist movement significantly increased measures of hamstring length in healthy participants. Improvements found immediately post-intervention were maintained for the 24-hour follow-up without any direct treatment to the soft tissue of the hamstring. The results of the study suggest that utilizing a regional interdependence approach and balancing the asymmetries in the musculoskeletal system may result in improvements in hamstring extensibility and hip ROM.
Corresponding Author
Rich D. Patterson DAT, LAT, ATC
Department of Exercise, Health & Sport Sciences
Pennsylvania Western University
California PA, 15419
Rpatterson@pennwest.edu
Conflicts of Interest
The authors report no conflicts of interest.