
Introduction
Rotator cuff tears are a prevalent source of debilitating shoulder pain and reduced mobility, often leading to irreversible damage of the glenohumeral joint.1 They constitute a significant portion of shoulder-related disabilities in the United States, accounting for 30% to 70% of shoulder pain cases and representing a primary reason for over 4.5 million annual medical consultations.2–4 The progression of these tears typically initiates with partial-thickness damage and can advance to complete tendon rupture due to various pathological or traumatic factors. Symptoms commonly include nocturnal pain, shoulder weakness, and difficulty performing overhead activities.
The infraspinatus muscle, integral to the rotator cuff, frequently sustains injury in both athletic and general populations. The infraspinatus plays a primary role in facilitating external rotation motion. Equally important, the infraspinatus serves as a stabilizer of the glenohumeral joint. Together with other rotator cuff muscles, the infraspinatus reinforces the inherently fragile glenohumeral capsule, ensuring the humeral head remains securely positioned within the scapular glenoid cavity.
Disorders affecting the infraspinatus can significantly impair shoulder function and are commonly encountered in clinical practice. Accurate assessment of rotator cuff pathology is essential for effective management. Historically, contrast arthrography was pivotal in diagnosing full-thickness tears, yet its utility in assessing tear size and detecting partial-thickness tears is limited.5,6 Magnetic resonance imaging (MRI), though widely accepted, faces challenges in reliably distinguishing between tear types and cuff degeneration.6 Recently, musculoskeletal ultrasound (MSK-US) has gained prominence for its real-time imaging capabilities, safety profile, and cost-effectiveness in diagnosing infraspinatus tendon and muscle conditions.7 This article examines the role of MSK-US in the comprehensive evaluation of these structures, particularly relevant to rehabilitation professionals.
Anatomy of the Infraspinatus
A comprehensive understanding of anatomy is essential for precise MSK-US evaluation, facilitating the identification of pathological alterations and the formulation of effective rehabilitation protocols. Situated beneath the scapular spine within the infraspinatus fossa, the infraspinatus muscle originates from this fossa and inserts into the greater tubercle of the humerus. Its fibers extend towards the glenohumeral joint, attaching just inferior to the supraspinatus insertion. Primarily responsible for external rotation, horizontal abduction, and abduction of the humerus, the infraspinatus muscle collaborates with other rotator cuff muscles to stabilize the humeral head within the glenoid cavity. Innervated by the suprascapular nerve and predominantly vascularized by branches from the posterior humeral circumflex and suprascapular arteries, it exhibits comparatively robust vascular support, potentially reducing the incidence of pathology and degenerative changes. Patients experiencing an infraspinatus tear often report pain during resisted external rotation and active elevation movements.
Benefits of MSK-US
MSK-US offers several advantages over other imaging modalities in the assessment of the infraspinatus muscle and tendon. These include:
-
Real-time Imaging: Allows for dynamic assessment during motion and muscle activation. This ability is crucial for identifying subtle dysfunctions that occur during movement, which are often missed by static imaging techniques.
-
Cost-Effectiveness: MSK-US is generally more affordable than MRI or CT scans, making it accessible for routine clinical use.
-
Non-Invasive: The procedure is non-invasive and well-tolerated by patients, reducing the need for anesthesia or contrast agents.
-
High Resolution: Detailed visualization of soft tissue structures is possible at a higher resolution than MRI in some cases.
-
Immediate Results: MSK-US provides immediate feedback, allowing for quicker clinical decision-making. The immediate feedback and interactive nature of the ultrasound examination also facilitate enhanced patient-clinician communication.
-
Accessibility and Safety: MSK-US is a patient-friendly option, avoiding the discomfort and contraindications associated with ionizing radiation and magnetic fields.
Limitations and Considerations
Despite its benefits, MSK-US also presents several limitations:
-
Operator Dependency: The accuracy of MSK-US is highly dependent on the skill and experience of the operator.
-
Limited Field of View: While excellent for soft tissues, MSK-US may not be as effective for evaluating bony structures.
-
Artifact Presence: Artifacts can sometimes obscure the view and complicate the interpretation of images.
MSK-US Technique for Evaluating the Infraspinatus
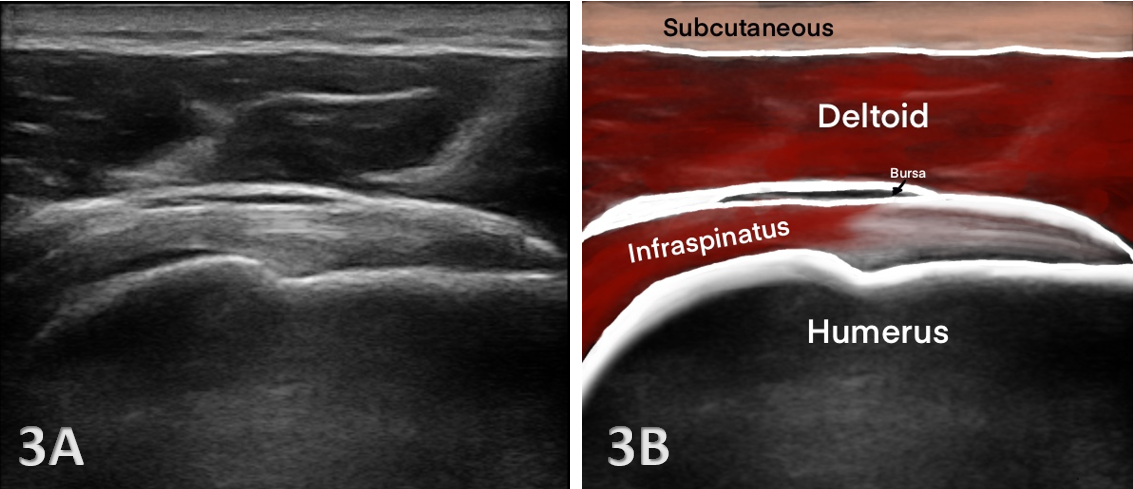
The examination of the infraspinatus muscle and tendon via MSK-US requires precise technique. Proper patient positioning and transducer placement are crucial to obtain accurate and reproducible images. The patient is typically positioned in a sitting posture with the back exposed and the arm in internal rotation to maximize infraspinatus visibility. The transducer is placed in a longitudinal and transverse orientation along the course of the muscle and tendon to assess for any structural abnormalities, such as tears, tendinopathy, or atrophy. Special attention is paid to the echogenicity and texture of the tendon, signs of inflammation, and the presence of bursal fluid.
Equipment and Setup
-
Transducer: A high-frequency linear transducer (7–15 MHz) is typically used for evaluating the infraspinatus.
-
Patient Positioning: The patient is usually seated position with the shoulder in slight abduction and internal rotation to optimize visualization of the infraspinatus.
-
Scanning Technique:
-
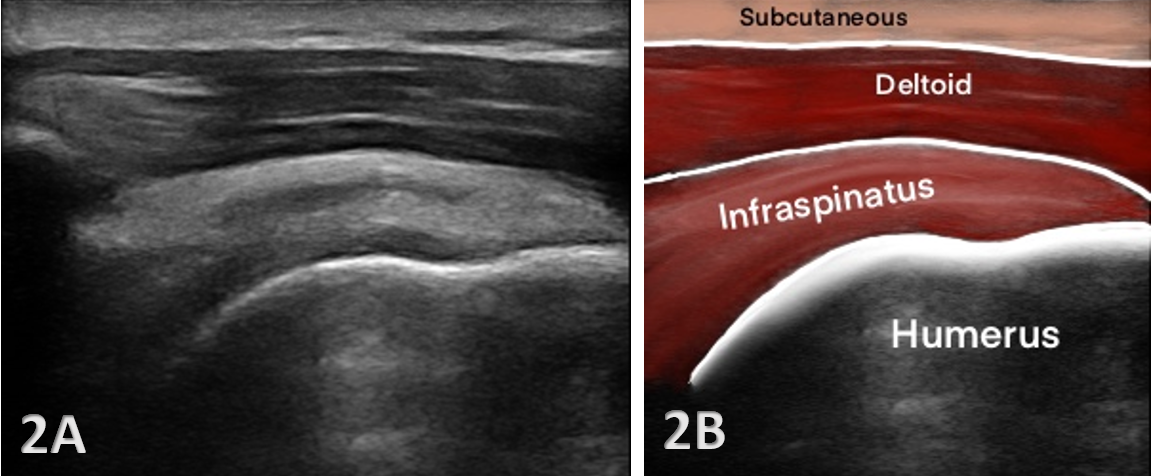
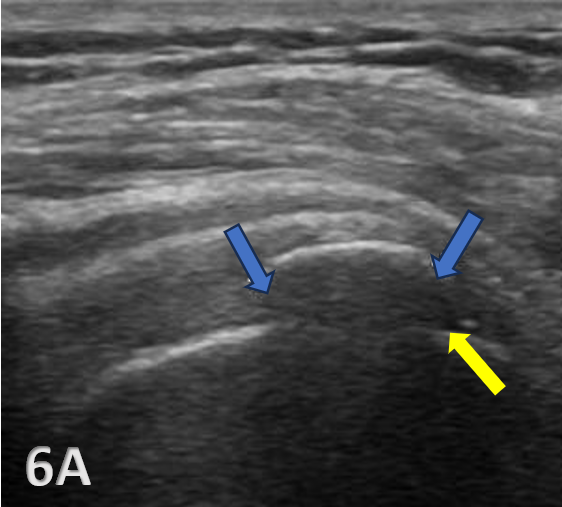
Transverse Scans: Begin with transverse scans to identify the spine of the scapula and follow the muscle belly towards its insertion on the humerus. The transducer is transversely placed inferiorly and slightly laterally from the scapular spine. Passive internal and external rotation of the patient’s arm may be helpful in visualization of the tendon. The infraspinatus tendon appears as a beak-shaped soft-tissue structure that progressively thins as it approaches its attachment to the posterior aspect of the greater tuberosity.6 Additional structures seen at this level are the posterior glenoid labrum, imaged as a hyperechoic triangular structure and the hypoechoic articular cartilage of the humerus.
-
Longitudinal Scans: Longitudinal scans help in assessing the tendon and its attachment to the greater tubercle of the humerus.
-
Key Findings
Ultrasound imaging of the infraspinatus must be carefully interpreted. Normal anatomy appears as a fibrillar pattern with uniform echotexture. Pathological findings may include:
-
Muscle Atrophy: Reduced muscle bulk can indicate chronic rotator cuff pathology.
-
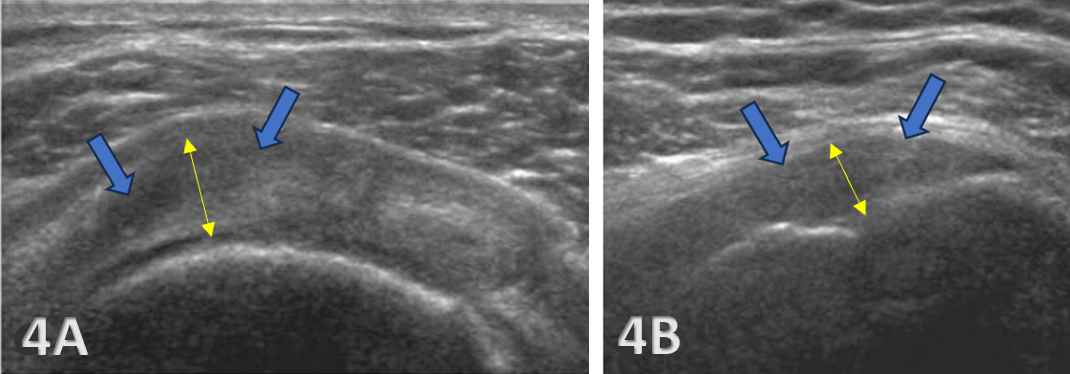
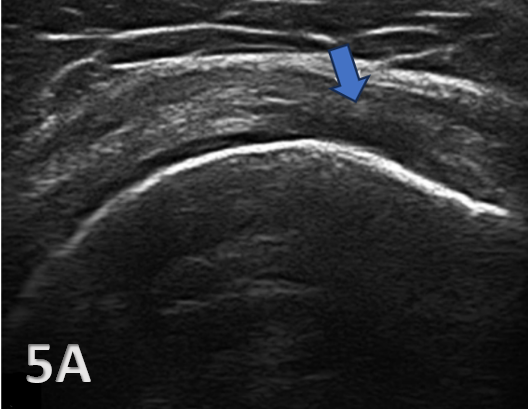
Tendinopathy: Characterized by hypoechoic (darker) areas and tendon thickening which may signify tendinopathy or degeneration.
-
Tears: Full-thickness or partial-thickness tears are displayed as hypoechoic or anechoic (absence of echoes) defects within the tendon. Additionally, they may be identified by discontinuities in the tendon fibers.
-
Calcific tendinitis: Identified by hyperechoic (brighter) foci with or without acoustic shadowing.
Conclusion
Musculoskeletal ultrasound has emerged as a pivotal tool for assessing and managing disorders of the infraspinatus muscle and tendon. Its capability to deliver real-time, high-resolution imaging renders it invaluable for dynamic evaluations and guiding rehabilitation protocols. Despite inherent limitations, the benefits of MSK-US position it as a cornerstone of contemporary clinical practice. To effectively integrate MSK-US into rehabilitation settings, practitioners must acquire specialized training encompassing both ultrasound techniques and detailed knowledge of infraspinatus musculoskeletal anatomy. By leveraging this technology in clinical practice, rehabilitation providers can elevate diagnostic accuracy, optimize therapeutic interventions, and ultimately enhance outcomes for patients grappling with shoulder pathologies.

.png)
.png)
_and_long_axis_(lax)_view_.png)
view.png)
.png)