



INTRODUCTION
Ulnar collateral ligament (UCL) injury is a common elbow injury among overhead athletes, particularly baseball pitchers; however, limited research exists for non-throwing athletes.1 While the understanding of UCL pathology is most robust in the specific context of repetitive valgus loading of the ligament during the throwing motion, other sporting activities can impart stress on the medial elbow which places the UCL at risk for injury.2 Therefore, UCL pathology is not limited to pitchers and does occur in other sport populations, primarily those classified as contact sports.
Contact sports, however, exclude a large population of athletes encompassed in upper extremity weight-bearing (UEWB) competition, including gymnastics and cheerleading. A retrospective study of UCL injury among athletes in the National Collegiate Athletic Association (NCAA) from 2009-2014 revealed “a high rate [not defined] of UCL injury exists in non-throwing sports populations” with little data regarding return to play criteria. The statistics from that study indicate 76.1% of the documented UCL injuries occurred during contact-related sports as compared to 23.1% that were classified as related to throwing sports as the mechanism of injury.3 Another study evaluating UCL epidemiology reviewed a consecutive series of 136 UCL injuries sustained during sport at a single institution over a 16-year period of time.1 These results indicated that 26.7% of the sustained injuries occurred in athletes that were participating in non-throwing sporting activities including gymnastics, cheerleading, mixed martial arts, and football. A problem exists with athletes being rehabilitated with non-sport-specific evidence and recommendations.
Review of Literature
The UCL is the primary restraint to valgus loads across the elbow. The ligament is composed of three bundles- the anterior oblique, posterior oblique, and transverse. The anterior oblique bundle is the strongest of the three and composed of two bands: the anterior, which is the primary valgus stabilizer with the elbow in 30-90 degrees of flexion and the posterior, which is the primary valgus stabilizer with the elbow in 90-120 degrees of flexion.4 The anterior oblique bundle originates on the medial epicondyle of the humerus and inserts on the sublime tubercle of the proximal ulna. In throwing athletes, UCL injuries are noted to be chronic, attritional stress related injuries. In contrast, a non-throwing athlete’s mechanism of injury is more consistent with an acute, traumatic incident.2 The differences between throwing and non-throwing athletes reflects a distinct subset of UCL pathology, often with different prognostic implications. The acute traumatic injuries sustained by non-throwers often induce a partial injury or complete tear of the ligament at a single site, compared to the more common attritional tear patterns seen in throwing athletes.2 These structural differences attributable to the nature of the injury lead to different treatment options, both non-surgically and surgically.
For high-demand overhead athletes, surgical management is often recommended for complete and partial tears or following failed conservative therapy as a way to effectively return athletes to their preoperative level of play. In fact, research shows that over the past 15 years, a significant increase has been noted in UCL reconstruction.5 Although outcomes after surgery have been favorable with the throwing athlete, UCL reconstruction usually requires at least 10 to 16 months for full recovery with potential surgical risks and complications, such as fracture, inadequate healing, and nerve injury.6
Swindell et al5 noted that nonsurgical treatment of UCL injuries may be helpful among non-throwing athletes (what is termed “lower demand populations”) as well as high-demand overhead athletes suffering from partial tears and sprains found on MRI examination. In addition, Cain et al7 report that nonoperative treatment of UCL injuries is generally indicated in non-throwing athletes with acceptable results. In a case report including five Division 1 collegiate gymnasts with UCL injuries, four out of five were able to return to a component (limited to event specialists at this higher competitive level) of competitive gymnastics following a structured rehabilitation program.8
Currently, the focus of conservative therapy primarily revolves around rest, anti-inflammatory medication, immobilization under certain conditions, and structured rehabilitation protocols. Few studies have been published detailing the nonsurgical treatment options currently utilized in practice for UEWB athletes. Furthermore, return to sport (RTS) criteria largely focuses on open chain activities such as throwing for speed, accuracy, and distance with UCL integrity analysis and only minimal emphasis on weight-bearing capabilities. Clinical commentaries based on expert opinion to guide decision making on RTS for upper extremity (UE) athletes have been suggested but these documents lack standardized scoring, classifications, and testing criteria.9 This lack of evidence-based data on RTS limits therapists’ prognoses for a large population of athletes.
In general, nonsurgical physical therapy rehabilitation consists of three phases: (1) reduction of inflammation and restoration of ROM, (2) progressive muscle strengthening and endurance, and (3) gradual RTS.5 Swindell et al5 indicated most protocols in nonsurgical rehabilitation accomplish RTS through an interval-throwing program, which would not be used with non-throwing athletes. Unfortunately, no other structured exercise program has been referenced or documented for UEWB athletes to ensure success with RTS criteria. Therefore, the purpose of this case report is to illustrate the use of early weight-bearing activities into the rehabilitation protocol for non-operative management of athletes with a UCL injury. The authors hope that this will encourage further research in this population regarding RTS testing.
CASE DESCRIPTION
The subject was a 17-year-old right hand dominant female who participated in both competitive and high school cheerleading. The case report was successfully reviewed for IRB exemption to allow publication, which included informed assent for the subject and consent for the subject’s mother through the University of Central Arkansas Institutional Review Board. The subject presented with a two-week history of medial elbow pain following a sports injury. The injury occurred during the performance of an acrobatic skill (Arabian), where the subject performed the following mobility sequence: exited a twisting flip, landed on a single lower extremity, transferred weight to the opposite lower extremity, and then proceeded to place both hands on the artificial turf (football field) to perform a round off. While entering the round off, she experienced what she described as a “crackle” of her elbow. During this skill, she is transferring weight from her initial contact hand (right) to the other hand (left) with bilateral lower extremities extended in the air (Figure 1). She denied feeling a distinct “pop” in her right elbow but expressed a sense of instability, prompting her to discontinue the remaining tumbling pass to avoid further and potential catastrophic injury. She had immediate pain and resultant swelling with ecchymosis at medial elbow and her symptoms were addressed by the athletic trainer on site. The subject utilized an ice pack and kinesiology tape (KT), per the trainer’s recommendation, and refrained from any weight-bearing activities for the remainder of the sporting event. She chose to not pursue any additional medical treatment or imaging and was managed by the athletic trainer with modalities for two weeks prior to her self-referral for a physical therapy evaluation.

Examination
The examination was performed by a board-certified orthopedic clinical specialist with 10 years of physical therapy experience. Additionally, the physical therapist was a 15-year veteran gymnastics coach. A physical examination followed the subjective history and screening, which included a systems review and upper quarter screen indicating no other concerns. The subject had normal body mass index, age-appropriate vitals, and only musculoskeletal system involvement noted. The subject did have a history of a successful anterior cruciate ligament reconstruction two years prior but no other medical history of significance.
The physical examination was tailored to the subject’s tolerance, based on the severity and behavior of symptoms and focused on obtaining an appropriate diagnosis. Elements of the physical examination included inspection, palpation, range of motion (ROM), flexibility, soft tissue mobility, strength, and special tests. Joints above and below the noted injured area were cleared during the upper quarter screen. The subject expressed no pain at rest but maintained right elbow and shoulder adducted with 90 degrees of elbow flexion in a guarded position. The subject had two previously applied strips of KT tape in place on the right medial elbow and with removal, demonstrated mild skin irritation and hypersensitivity to touch. Mild residual swelling was present at medial epicondyle but no ecchymosis during the initial examination. Photographic evidence of moderate ecchymosis after the initial soft tissue trauma is presented in Figure 2.

The subject demonstrated full pain-free active range of motion (AROM) for bilateral elbow flexion and extension, forearm supination and pronation, with +5 degrees of passive hyperextension on the right compared to +1 degrees on the left. The subject demonstrated slight weakness and no pain with resistance testing of the elbow flexors, forearm pronators, and wrist extensors on the right; however, moderate weakness with minimal pain of the elbow extensors, forearm supinators, and wrist flexors on the right. Bilateral shoulder and left upper extremity strength testing revealed no deficits with resistance in all planes of movement. Hand dynamometry for mass grasp revealed 58 lbs. on the right (dominant) upper extremity and 55 lbs. with left (non-dominant) upper extremity. She exhibited facial grimacing and apprehension with dynamometer strength testing but indicated no significant pain.
Orthopedic special tests were selected based on the hypotheses developed during the subject interview and with the previous objective findings. Findings included a positive valgus stress test, positive moving valgus stress test, and negative varus stress test. Neurovascular screen was unremarkable with appropriate sensation to light touch and no neural tension present for bilateral upper extremities. Return to sport UE functional testing was deferred at this time due to acuteness of injury. These tests would have consisted of Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) and the Seated Shot-Put Test (SSPT) both of which have well established reliability and validity.9
Patient-reported outcome measures were selected to adequately capture the subject’s perception of her functional status. In addition, these outcome measures are responsive to individual patient preferences, needs and values, and assist to guide clinical treatment decisions. The subject completed a self-report outcome measure with Focus on Therapeutic Outcomes (FOTO) with a score of 69/100, with 100 established as the highest functioning level without limitations. Administration of the Quick Dash resulted in a raw score of 43/100, on a scale ranging from 0 (no disability) to 100 (most severe disability). Both FOTO and Quick DASH were utilized to assess functional outcomes with documented reliability,10–12 per the clinic’s policies and procedures.
Diagnosis/Prognosis
Clinical decision making and development of a hypothesis began with the subject profile, location of symptoms, and reported mechanism of injury. Questioning during the interview and findings of the physical examination refined the hypothesis. The physical therapist’s diagnosis based upon clinical experience was a potential grade II UCL sprain, as evident by presentation and performance of ligamentous valgus instability test with positive findings of joint space opening.13 Alternative hypotheses and differential diagnoses included acute fractures, radio-humeral contusion, and radial head subluxation which were ruled out with further tests and measures. With reference to the International Classification of Function and personal goals, the subject, parent, and therapist discussed a non-surgical rehabilitation approach with a goal of return to sport participation, with no need for outside referral at that time and to initiate physical therapy.
Interventions
The subject attended 14 physical therapy sessions over the course of nine weeks. Additionally, the subject participated in independent and modified workouts with the subject’s designated sports team, developed by the physical therapist. The initial goal for the chosen interventions was to reduce pain, improve functional movement, and restore strength at the elbow. Subsequent goals were to achieve desired and functional strength for weight-bearing activities and RTS. The subject was scheduled to attend collegiate try-outs in a few months and participate in a world cheerleading competition in six months. Treatment sessions included interventions consisting of manual therapy, therapeutic exercise, therapeutic activity, neuromuscular re-education, and standard modalities as needed.
Manual therapy in the initial phase of treatment consisted of soft tissue mobilization and friction massage to reduce adhesions, improve blood flow, and reduce pain. Interventions designed for neuromuscular re-education included proprioceptive and stability training. Therapeutic exercise consisted of graded exposure with ROM, endurance activities, strength training, and the inclusion of blood flow restriction (BFR) with the Delfi Personalized Tourniquet System (Owens Recovery Science, San Antonio, TX). Therapeutic activity included functional weight-bearing components as well as dynamic movements of lifting, carrying, jumping, and return to sport- specific training. The modalities selected for this subject included interferential current (IFC), cryotherapy with cold packs, and self-application of ice massage as needed.
This impairment-based approach was not based on a set protocol, due to lack of supporting research for a weight-bearing subject, but tailored to the individual subject based on examination findings and desired functional goals. Interventions were modified based on current/daily status, delayed onset muscle soreness, physical activity performed outside of the clinic, and physical capabilities. Both the subject and guardian agreed with established goals and designated treatment plan of care.
The initial evaluation consisted of a one-hour session which included a subject interview, physical examination, treatment interventions, and the prescription of a detailed home exercise program. The subsequent 30-45-minute sessions consisted of hands-on assessment and interventions as described above. Table 1 includes a broad description of the treatment program. In addition to the in-clinic treatment sessions, the subject performed independent exercises daily as part of a home exercise program and inclusion of previous cardio and core fitness routine. The intensity of each session was monitored and adjusted based on the subject’s symptoms and numerical pain rating.
Weight-bearing Treatment
Weight-bearing exercises for the upper extremity come in a variety of forms and levels of difficulty, beginning with a standing weight shift with palms on a support surface or static quadruped hold and progressing through plank positions to inverted push-up positions. These aforementioned exercises, however, are not challenging enough for high-level weight-bearing athletes who necessitate additional sports specific training requiring more creativity with implementation. The focus on upper extremity weight-bearing exercises can be beneficial for overall strength and stability with the general athlete. However, for these unique athletes, more advanced weight-bearing exercises are vital to return to their perspective sport and safety with performance of acrobatic skills.
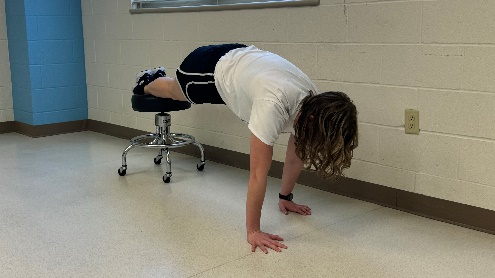
The progression of weight-bearing was discerned in parallel with the subject’s response to treatment interventions and daily visual re-assessments and a broad overlay of interventions is presented in Table 1. The subject was initiated with light UE weight shifts in standing in week one for joint approximation, biofeedback, kinesthetic awareness, muscle engagement, and joint mobility. These exercises were a prelude to additional weight acceptance with perturbations and performance of wall push-ups and limited range triceps dips in week two. By week three, the subject was able to sustain additional weight through her UEs with quadruped activities and inclined push-ups. Week four was pivotal with majority of her exercises performed in a weight-bearing position; these exercises consisted of various angles of weight acceptance on upper extremities, lateral shifts to unilateral UE support, increased duration, and dynamic integration of exercise games (Figure 3).

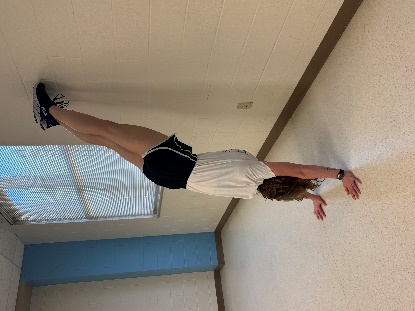
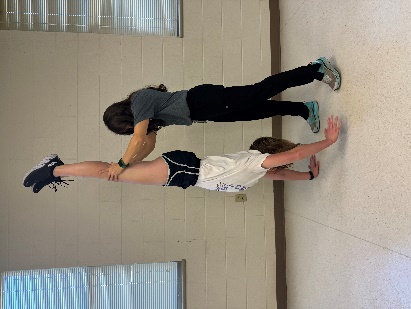
With the steady advancement demonstrated by improved tolerance to exercise duration and additional weight-bearing, the focus of therapy shifted to the subject’s tolerance of transitions to other weight-bearing positions. Although she could withstand 30 seconds of a handstand (UE weight-bearing) position, she had difficulty with the quick transition into this position, which is essential with tumbling. Cheerleaders need to be able to withstand the quick impact and joint force that is a result of tumbling. The amount of force generated by a cheerleader during tumbling can vary based on factors such as the athlete’s speed of movement, body mass, technique, and the level of skill being performed. Tumbling involves rapid and dynamic movements and the force exerted is influenced by the acceleration and deceleration of the body. At this point, she was unsafe to pursue any higher-level tumbling, requiring these quick unweighted to weighted positions; however, with implementation of week five exercises (Figures 4-5), she exhibited continued positive strides in her rehabilitation plan.


With week six and facilitation of a re-evaluation, the subject was noted to have successfully passed the RTS testing for UE involvement, although the practitioner did not clear her for full return to sports due to the remaining deficits of unweighted to weighted UE activities and the subject’s lack of confidence with release to full activity. The subject continued with previous UEWB exercises and progressed with weight acceptance focus and UE plyometric activity. With the subject’s transition to less clinical appointments and additional hours with sports specific training at cheer practice, she was able to have more isolated training in her therapy sessions. These sessions included shock absorption during transitional movements while receiving education on proper technique, strength, and conditioning to handle the desired higher-level skills (Figures 6-7).


With the early initiation of weight-bearing exercises that increased in both difficulty and duration, the subject was able to return to full sports participation with her advanced tumbling skills on padded surfaces (as required for her participation with competitive cheerleading) within the anticipated three-month timeline. Traditional sports rehabilitation for a UCL injury primarily focuses on shoulder and scapular strengthening with open-chain UE activities. This individualized treatment program focused on more dynamic exercise interventions, as evident by the abundance of weight-bearing exercises. Using functional, sport specific, weight-bearing activities, the subject was more invested and confident during interventions and exhibited a more successful outcome.
OUTCOMES
Within the first week of treatment, the subject was able to resume and perform daily tasks (writing, grooming, bathing) with little to no difficulty or complaint of pain. Following the second week of therapy, the subject reported discomfort only with more challenging daily tasks (i.e. opening a door with full triceps extension) or with inadvertent performance of quick UE cheer motions. Within the third week of therapy, the subject was able to participate with UE motions during cheerleading and perform non-UE weighted acrobatic movements without difficulty. By weeks four and five, the subject was able to resume basic cheerleading tumbling activities but had mild discomfort with full elbow extension activities.
At six weeks, the subject was re-evaluated and demonstrated improved self-reported FOTO and Quick Dash scores of 83 (improvement by 14) and 34 (improvement by 9), respectively. She reported a 2/10 pain rating (utilizing the numerical pain scale) during performance of tumbling but 0/10 pain at rest. During this reassessment, the subject demonstrated 80% limb symmetry index with the RTS UE functional testing of one-armed SSPT and 25 touches with the CKCUEST. Previous literature indicated the average touches were 22.5 for college football players,14 25 for healthy adolescents,15 and 30 for college baseball players.16 To date, variance is noted with researchers and no data exists for cheerleaders or gymnasts to assist a clinician with acceptable RTS status. Additional assessment exhibited a negative valgus stress test with lack of instability detected but she did report mild discomfort. Both PROM and AROM were near symmetrical with no deficits noted. She demonstrated no pain or weakness with resisted testing of right UE with the exception of right elbow extension which exhibited mild weakness. Dynamometer grip strength was not reassessed. She was limited with upper extremity full weight-bearing tolerance to 30 seconds before having deficits with strength tolerance and discomfort.
Based on these findings, continued skilled physical therapy intervention was recommended with frequency reduced to one day a week in the clinic and implementation of more sports-specific integration with competitive cheer coach and school athletic trainer. A detailed plan was provided to these individuals with acknowledgement of communication and collaboration demonstrating desired therapeutic alliance.
With the reduction of therapy sessions, the subject was able to implement additional cardiovascular and core programs previously performed which assisted in the therapy plan. Following week seven, the subject focused on psychological readiness and was self-monitoring her abilities and fatigue with implementation of sports specific training. During week eight, the client had returned to more advanced tumbling skills but was hesitant with standing weight-bearing skills (specifically the standing back handspring) due to more prolonged weight acceptance on upper extremities. Modifications were addressed with her competitive and school cheer teams to avoid these skills and more focus in therapy was placed on duration in UE weight-bearing and quick transitions to this positioning.
At week nine, the client was re-evaluated and demonstrated no elbow pain, instability, ROM, or strength deficits. Through the functional self-report questionnaires, she rated her abilities as 98 on FOTO and 0 on Quick Dash; this calculated score achieved the desired minimal clinical improvement differential. She performed the UE functional RTS (CKCUEST) testing and scored at 105% with her dominant, injured UE. Additionally, she was able to tolerate approximately one minute of prolonged UE weight-bearing, sufficient for her to return to all routine tumbling sports participation. At this time, she was performing her most advanced tumbling skills on surfaces that provided spring assist (rod floor and Tumble Trak®) with no need to perform on the ground with completion of football season.
DISCUSSION
The purpose of this case report was to describe an innovative approach to rehabilitation of an UEWB athlete, who achieved full return to sports following a UCL injury. To the authors’ knowledge, limited research exists supporting return to sports for this unique athlete population which impedes prognosis and professional consensus regarding rehabilitative approach. Presently, the only recommendation provided in the literature for non-throwing athletes with non-operative UCL injury is an individualized rehabilitation program with reassessment of the athlete’s pain with valgus stress once they have reached their baseline performance metrics and prior to return to play.17 Additional studies indicate the need for an evidence-based nonoperative protocol and consensus for the treatment of UCL injuries in UEWB athletes.18 Unfortunately, no specific testing exists to determine readiness both physically and psychologically to develop more sports specific protocols.
This multimodal treatment approach that highlights progressive loading of the upper extremity was beneficial for this subject. The tailored treatment plan combined with the subject’s motivation was successful with restoration of UCL stability. With the recommended non-operative UCL rehab of traditional focus on rotator cuff and periscapular strengthening combined with more sport specific gradual weight-bearing activities, this athlete was able to progress to full weight acceptance and return to sport demands.
Although this case report demonstrates positive outcomes for one UEWB athlete with a UCL injury, this rehabilitation program may or may not be beneficial for additional UEWB athletes with an upper extremity injury with moderate impairment deficits. While speculation may exist that the results were due to the implementation of sports specific weight-bearing activities, determining the true cause-and-effect relationship of interventions to outcomes is not possible in a case report.
CONCLUSION
This case report highlights the successful treatment of an upper extremity weight-bearing athlete with a UCL injury after integration of various treatment interventions with a focus on progressive UE weight-bearing. Further research is imperative regarding the non-operative rehabilitation of athletes who perform high level UEWB activities as a part of their sport as well as more in-depth study of return to sport testing.