
INTRODUCTION
Swimming is a popular form of exercise both recreationally and competitively. A 2021 survey revealed that there were 2.8 million people aged six years and older competing on a swim team in the United States (US).1 The non-weight bearing nature of the sport may lead people to believe that it is safe for joints. While this may be true for the recreational swimmer, elite swimmers may swim up to 14,000 meters and undergo 2,500 shoulder revolutions per day,2 with competitive swimmers practicing five to seven days per week, sometimes twice daily.3 It is therefore not surprising that shoulder pain is the most common orthopedic complaint in swimmers. A majority of high school competitive swimmers in one study believed that shoulder pain is normal, with 47% of this group reporting that they take pain medication regularly to manage their shoulder symptoms.4
The most recent wide-scale study reporting the prevalence of shoulder pain in youth swimmers in the US was published by McMaster and Troup in 1993,5 who collected over 1,000 survey responses from swimmers aged 13–16 years who were selected for participation in USA Swimming-sponsored national training camps. The authors defined shoulder pain as pain that interfered with training or progress in training and reported that 9-26% of the swimmers were currently experiencing pain and 38-67% reported a history of shoulder pain.5 Furthermore, the more years of competitive experience the swimmers had, the more likely they were to experience shoulder pain.5 To date, there has not been another study from a diverse sample reporting on the prevalence of pain and disability in youth swimmers in the US, thereby accounting for possible changes in training over the past three decades.
Recent studies reporting prevalence of shoulder pain in youth competitive swimmers have been smaller in scale and limited to a single geographical region. An Australian study published in 2010 with 90 swimmers aged 13–25 years reported a pain prevalence of 91%.6 An Italian study revealed that in a cohort of 197 swimmers aged 12–20 years, 51% reported shoulder pain within the prior 12 months.7 A US study of female swimmers aged 8–77 years found that 18.6-22.6% reported significant pain and disability.3 Although definitions of pain and disability vary among these studies, it appears that there are differences in rates of shoulder pain across geographical regions and age-groups.
Several risk factors for shoulder pain have been identified in the literature. Tate et al. found that youth swimmers with shoulder pain, disability, and dissatisfaction reported a greater history of shoulder trauma, had greater years of competitive swimming experience, and had less participation in another sport compared to their less symptomatic counterparts.3 However, this study included only female swimmers from a single geographical region of the US.3 Since female youth competitive swimmers have reported a higher prevalence of shoulder pain than males7 and training practices can differ across geographical regions, a wide-scale study including males and females across different geographical regions of the US would provide more generalizable data to identify swimmers at risk for shoulder pain and disability who may ultimately benefit from a prevention or intervention program.
Due to the paucity of large-scale studies identifying symptoms in competitive swimmers, the primary purpose of this study was to determine the prevalence of shoulder pain, disability, and dissatisfaction with current level of function of the shoulders in youth competitive swimmers aged 9–17 years over a diverse geographical area of the US. Additional aims of this study were: (1) to determine the influence of age, competitive swimming experience, and previous history of shoulder pain that interfered with practice/competition or traumatic injury on shoulder pain, disability, and dissatisfaction, and (2) to determine if differences in sex, geographic area, and participation in a second sport relate to reported shoulder pain, disability, and dissatisfaction.
METHODS
Design
A multi-site cross-sectional survey design was used.
Participants
YMCA or USA club swimming association teams and their swimmers in the following age groups were recruited for the study: 9 to 10 years-old, 11 to 12 years-old, 13 to 14 years-old, and 15 to 17 years-old. Parents/guardians and swimmers were invited to participate through an information sheet explaining the study and provided informed consent/assent. This study was approved by both the University of Southern California Institutional Review Board and the Arcadia University Institutional Review Board.
Surveys
Parents/guardians and swimmers completed a swimmer survey and coaches completed a coach survey developed by the authors as part of a larger study. The results of the swimmer surveys collected between 2015 and 2018 are presented in this manuscript. The swimmer survey requested anthropomorphic data including age, sex, height, weight, and swimming and training data including competitive age-group, primary stroke, years of competitive swimming participation, months per year of swimming, and participation in other sports. In addition, components of the Penn Shoulder Score (PSS) and the Disability of Arm Shoulder Hand (DASH) Sports were used for self-reported outcome measures. The satisfaction and pain sections of the PSS were used to rate swimmers’ satisfaction from 0-10, with 0 being not satisfied and 10 being fully satisfied with current shoulder function, as well as for pain at rest, with normal activity, and with strenuous activity on a numeric pain rating scale from 0-10, with 0 being no pain.8 The term “dissatisfaction” is used in this manuscript instead of “satisfaction” to enhance readability and is defined as a lower Penn satisfaction score. The DASH Sports was used to assess swimming-related disability with a score range of 4-20 points, 4 equating to having no difficulty with physical ability related to swimming and 20 equating to being unable to perform swimming tasks.9
Swimmers were also asked to describe any current symptoms they may have had using one of five options as described by Neer and Welsh: Phase 0, no pain or shoulder symptoms; Phase I, pain/ache only after heavy workouts; Phase II, pain/ache (not disabling) during and after workouts; Phase III, disabling pain during and after workouts that interferes with athletic performance; and Phase IV, shoulder pain preventing competitive sport participation.10 These surveys were administered during high training volumes of each team’s season, as confirmed by the team’s head coach. Surveys were given either in-person using paper format or electronically using online format. The online format was administered via the RedCap database management system and was identical in content to the paper format. The head coach of the team distributed the paper form or a link to the online survey via email to the parents of the team members who provided consent. Participants had one week to complete the survey after receiving it.
Data Analysis
Participants were divided into four age-groups based on their competitive level: Group 1 = 9 to 10 years, Group 2 = 11 to 12 years, Group 3 = 13 to 14 years, and Group 4 = 15 to 17 years. Years of competitive swimming experience were divided into three groups based on the sample interquartile range: 0-25% labeled as least experienced, 26-74% labeled as moderately experienced, and 75-100% labeled as most experienced. An athlete was identified as having a history of shoulder pain if they indicated previous pain that interfered with competition or practice or if they had ever sustained a traumatic shoulder injury. Geographic region of the swimming team was divided into two groups: West included swimmers in Arizona and California, and East included swimmers in Florida, New Jersey, Pennsylvania, and Vermont.
Shoulder pain, disability, and dissatisfaction were reported for each age-group. ANOVAs with multiple post-hoc comparisons were performed to determine the effect of age-groups and percentiles of years of competitive swimming experience on shoulder pain, disability, and dissatisfaction in swimmers.
Independent t-tests were used to report mean differences in pain (PSS Pain Subscale individual items, PSS Pain total), disability (DASH Sports total), and dissatisfaction comparing sex (male vs female), participation in a second sport (yes vs no), geographic region (West vs East) and presence of a history of pain or injury (yes vs no).
Two separate linear regression analyses were performed to determine how age, sex, geographic area, participation in a second sport and prior pain or injury explained variability in pain (PSS Pain total) and disability (DASH Sports total). Independent variables were entered into the model using forward progression, with an entry criterion of 0.05 and exclusion criterion of 0.10.
Significance was set to 0.05 for all tests except those indicating a Bonferroni correction when multiple comparisons were warranted. These values are included in their respective tables. Bonferroni corrections were used first during multiple comparisons for data considering age-group and then for data considering the competitive experience of the athlete in an interquartile range. All statistical analyses were performed using SPSS (IBM, Armonk, NY).
RESULTS
Surveys were collected from 671 swimmers between the ages of 9 and 17 years old from YMCA and USA club swimming association teams from Arizona, California, Florida, New Jersey, Pennsylvania, and Vermont. Some swimmers did not fully complete their surveys; therefore the N of each measure differed slightly. As such, the authors were able to identify sex in 631 surveys (254 males [40.3%], 377 females [59.70%]), geographic region in 594 surveys (477 West [70.2%], 117 East [29.80%])) and participation in a second sport in 666 surveys (234 answered yes [35.1%]). Table 1 contains descriptive statistics of participants, Penn pain and satisfaction ratings, and DASH Sports ratings.
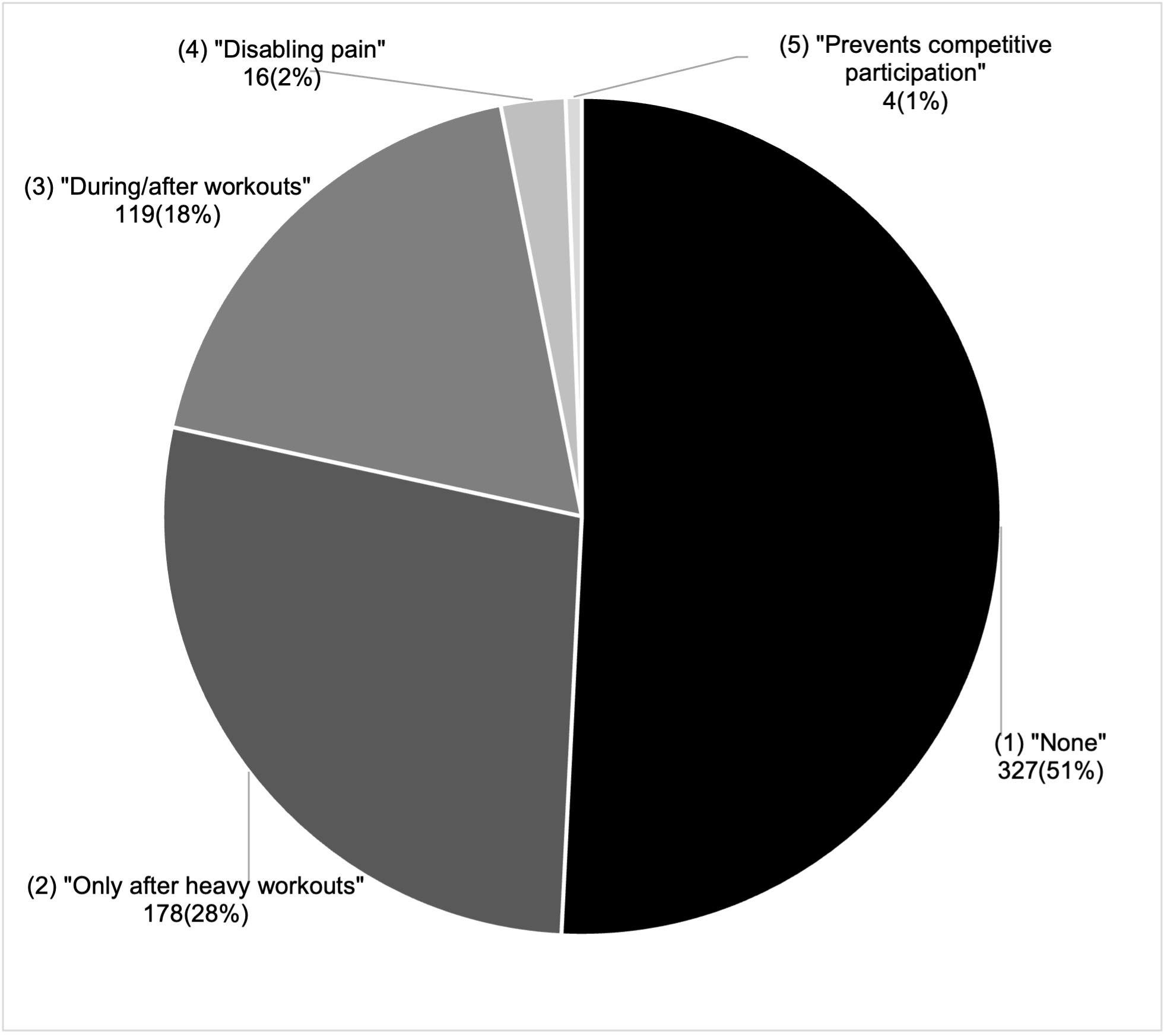
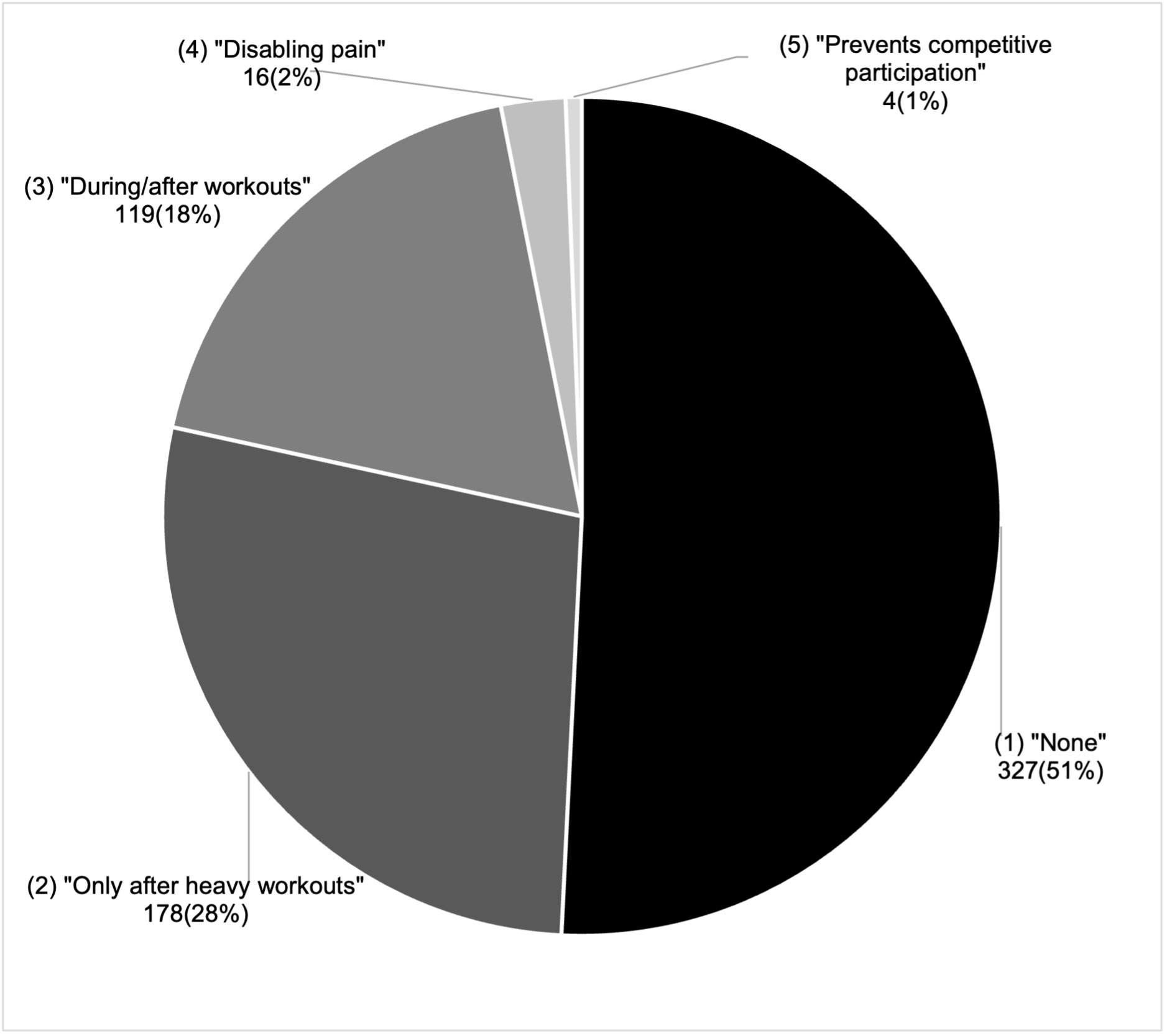
The figures represent descriptives of the prevalence of shoulder pain (Figure 1), swimmers per age group report a history of shoulder pain (Figure 2) and if they have shoulder pain today (Figure 3). Tables 2, 3 and 4 report the effects of age and swimming experience, sex, geographic area and other sports participation on reports of shoulder pain, disability and dissatisfaction with the use of their shoulder. Table 5 reports the effects prior pain or injury on shoulder pain, disability and dissatisfaction with shoulder use.


DISCUSSION
The purposes of this study were to (1) determine the prevalence of shoulder pain, disability, and dissatisfaction in youth competitive swimmers, (2) determine the influence of age, competitive swimming experience, and previous history of shoulder pain or injury on shoulder pain, disability, and dissatisfaction, and (3) determine if sex, geographic area, and participation in a second sport relate to shoulder pain, disability, and dissatisfaction. To the authors’ knowledge, this is the first large scale survey study involving youth competitive swimmers in the US since the McMaster and Troup study in 1993, in which the authors reported a current shoulder pain prevalence of 10% in 13 to 14-year-old swimmers and 13% in 15 to 16-year-old swimmers.5 By comparison in the current study, the percentage of swimmers who reported having current symptoms was 21.3% of 13 to 14-year-old swimmers and 28.1% of 15 to 17-year-old swimmers. McMaster and Troup did not collect data on 9 to 10-year-olds and 11 to 12-year-olds, so direct comparisons cannot be made for these age groups.5 Possible reasons for the higher percentage of swimmers with symptoms in the current study may include differences in swimming yardage, years of training, dryland training, and the exclusion of 17-year-olds from the 1993 study; however, data is not available for comparison thereby firm conclusions cannot be made.5
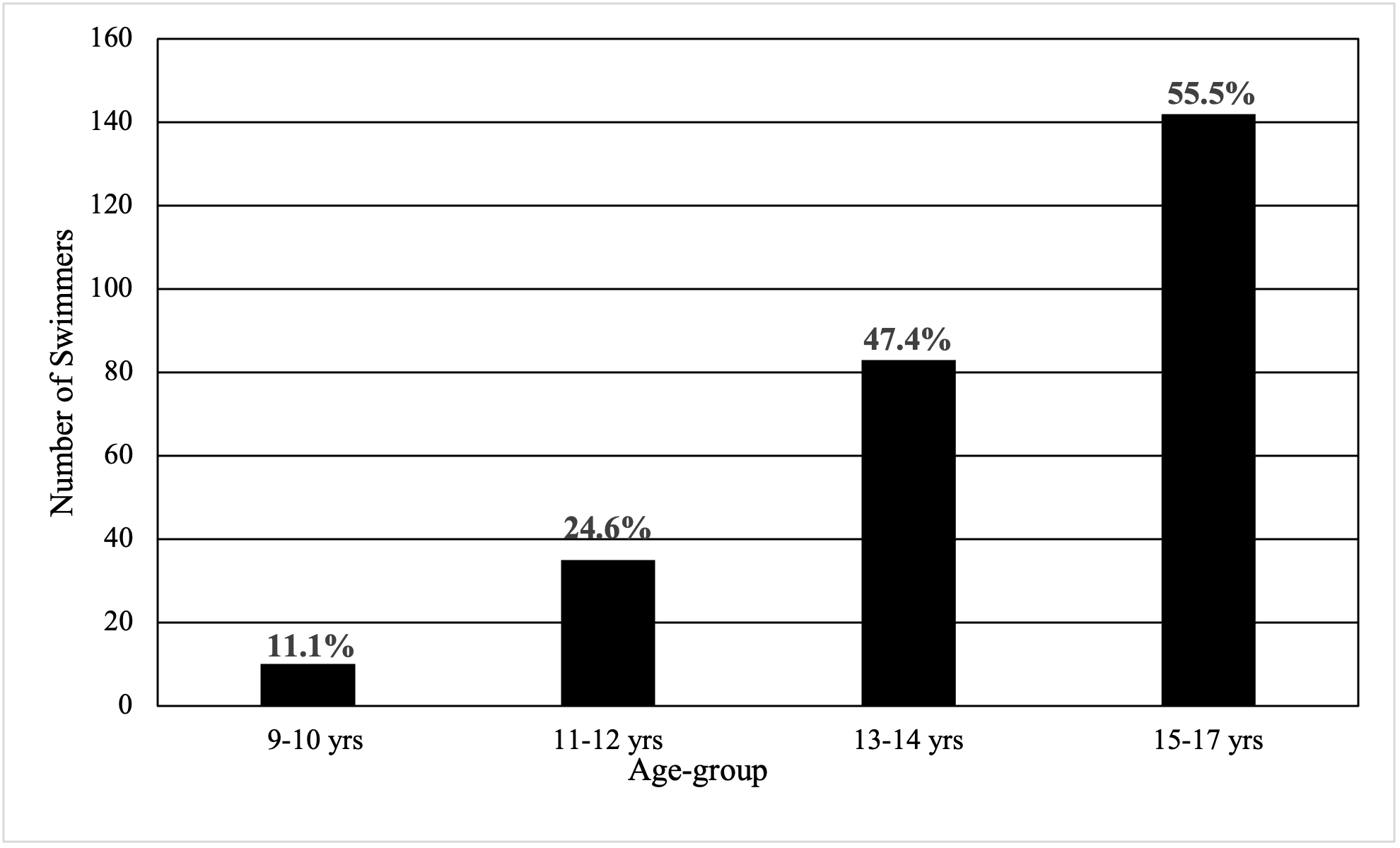
When swimmers were asked if they had ever experienced shoulder pain interfering with practice or competition, 47.4% of the 13 to 14-year-old swimmers and 55.5% of the 15 to 17-year-old swimmers answered “yes”. This finding is similar to McMaster and Troup’s report of 46.5% of 13 to 14-year-old swimmers reporting a history of interfering shoulder pain.5 However, McMaster and Troup reported 65.5% of their 15 to 16-year-old group having a history of interfering shoulder pain, which is higher than the current study’s report of 55.5%.5 This may be due to the higher level of competition in the 1993 study participants as a subgroup of the swimmers in that prior study were invited to participate in US national training camps.5 The current study invited swimmers of all levels within their age-groups to participate, regardless of competitive level.
Pain, Disability, and Dissatisfaction
As Table 1 depicts, the overall mean ratings of pain, disability, and dissatisfaction are relatively low, but about one-fifth of swimmers reported some amount of swimming shoulder-related disability. When swimmers were asked if shoulder pain impacted their swimming, 49% of swimmers surveyed reported having shoulder symptoms that impacted their swimming. While most swimmers reported pain/ache Phase I, only after heavy workouts (27.6%) and Phase II, during/after workouts (not disabling) (18.5%), a smaller percentage of swimmers reported Phase III, disabling pain during/after workouts (2.5%) and Phase IV, that prevents competitive participation (0.6%), as can be seen in Figure 1. For comparison, Bak and Faunø found values of 20% for Phase I, 59% for Phase II, 18% for Phase III, and 2% for Phase IV in a group of 36 swimmers from Denmark with histories of shoulder pain with a mean age of 17.11 Females made up 61% of their study participants and 36% were National team members.11 Since subjects in that prior study were recruited based on reporting a history of shoulder pain, had older mean ages, and greater than one third competed at the national level, it may be reasonable to expect that swimmers in the Bak and Faunø study reported higher percentages of disabling and non-disabling pain during/after workouts, as well as pain that prevented participation.11 Nonetheless, the findings of the current study support the concern that reported pain after and during workouts is being experienced by swimmers in the US. Bak and Faunø recommended that swimmers be classified into these phases of disability so proper interventions can be made to prevent progression into the subsequent phase.11 Furthermore, the current authors suggest that interventions such as stroke correction, yardage moderation and guidelines, and rehabilitation/training programs, addressing swimmer-specific impairments should be studied to determine their efficacy in reducing symptom and disability progression.
Influence of Age, Experience and History of Prior Shoulder Pain or Injury
In the current study, the percentage of “pain interfering with competition or practice” increased with each swimming age-group from 11.1% for the 9 to 10-year-olds to 55.5% for the 15 to 17-year-olds, as can be seen in Figure 2. The largest percentage difference between chronological age-groups was 22.8% between the 11 to 12-year-olds and 13 to 14-year-olds. Figure 3, which displays the number and percentage of swimmers who had shoulder pain at the time of the survey, demonstrates the largest percentage difference, 12.1%, between these age groups as well. This coincides with mean peak height velocity, defined as the period when a child experiences the fastest upward growth in stature,12 in females at 11 years and males at 13 years,13 which could explain the large percentage difference in pain found in this sample of swimmers. Increased training volume occurring near the time of peak height velocity can increase likelihood of injury,14 a phenomenon which has also been demonstrated in youth soccer players.15 With changes in body size, muscle mass, and maturation of the neuromuscular system, an athlete’s performance may improve naturally without specific intervention.16 In youth competitive swimmers, significant improvement in performance over the course of one year was shown to be strongly correlated with anthropomorphic changes while biomechanical variables remained relatively unchanged.17 However, shortly after a growth spurt, there is rapid longitudinal growth in bone with a delay of muscle length growth that leads to relatively rapid muscle lengthening and increases in resting tension of muscles, which limits overall amount of force production and reduces neuromuscular control.16 Therefore, it may be important for swimming coaches to consider sudden or recent developmental skeletal growth when implementing and executing swim training programs to mitigate potential risk for injury.
While the chronological age of the swimmer in the current study was related to shoulder pain, the years of competitive swimming experience is another factor that might affect a swimmer’s shoulder pain, disability, and dissatisfaction. The results demonstrate that pain and disability increase with age and years of competitive swimming experience. Specifically, 15 to 17-year-olds had significantly more pain and disability than 11 to 12-year-olds. Moreover, 13 to 14-year-olds and 15 to 17-year-olds had significantly more pain and disability than 9 to 10-year-olds. Likewise, moderately to most experienced swimmers had significantly more pain and disability than less experienced swimmers, which show that pain and disability may evolve over time and with a cumulative volume of training. Consistent with Tate et al., despite only collecting data on females, swimmers also reported increased pain, disability, and dissatisfaction with more competitive experience.3 Using ultrasound imaging, Dischler et al. demonstrated that years of swimming participation were directly associated with supraspinatus tendon thickening and declining function using the Western Ontario Rotator Cuff score.18 Another study of swimmers utilized MRI to demonstrate a direct positive correlation between supraspinatus tendon thickening and tendinopathy with years of experience and volume of training.6 With these previous swimming studies detailing progressive pain, disability, and morphological tendon changes as volume and experience increase, care must be taken when designing training programs for more experienced swimmers to minimize and prevent further shoulder pain and disability.
Additionally, the authors suggest that surveillance and prevention measures should be considered at younger ages and experience levels to attempt to prevent shoulder dysfunction leading to tissue pathology, which may negatively impact swimming performance. Longitudinal studies are needed to determine if there is a long-term consequence of shoulder pathology in youth on shoulder disability as adults.
It is important to note that while the findings show statistically significant differences among groups, the threshold for Minimum Detectable Change (MDC) and Standard Error of Measurement (SEM) for the PSS and the DASH were not reached, indicating that the differences are not clinically significant. MDC and SEM values for the Penn Pain subscale were reported as 5.2 and 3.8, respectively, and the Penn Satisfaction subscale results were reported as 1.3 and 1.8, respectively.8 For the complete DASH measure, MDC was reported as 12.8 and SEM as 7.619; however, clinically meaningful thresholds for the DASH subscales, such as the DASH Sports, have not been previously reported. Therefore, the authors cannot conclude whether the statistically significant differences are clinically significant or meaningful.
Reported history of previous shoulder pain that interfered with competition/practice or traumatic injury significantly predicted higher levels of current pain, sports-related disability, and dissatisfaction with the use of the swimmers’ shoulder(s). Additionally, more competitive years of experience significantly predicted higher levels of pain. This is consistent with the findings of McMaster & Troup, who reported that the prevalence of shoulder pain increased with more participation time in swimming.5 Given the consistency of results, it is advantageous and beneficial for coaches and clinicians to be aware of any prior history of shoulder pain or traumatic shoulder injury in their swimmers, understanding the association of this with further pain, disability, and dissatisfaction. Effective interventions should be developed for these at-risk individuals.
Influence of Sex, Geographic Area, and Other Sport Participation
When comparing the swimmers geographically, significant differences were identified in reported pain and disability between Eastern and Western teams, with Eastern teams reporting greater pain and disability. Further studies should investigate training methods, including yardage and dry land training to determine if these vary between the Eastern and Western regions of the US, which may explain differences found in the reported pain and disability findings in the current study. Interestingly, swimmers who participated in a second sport reported significantly less dissatisfaction than swimmers who participated in swimming only. Evidence of dissatisfaction in sport specialized athletes is limited, but athletes who participate in a single sport and a predominantly individual sport like swimming may be at risk for social isolation, overdependence, burnout, manipulation, injury, and compromised growth and maturation.20 Thirdly, no significant differences were found in shoulder pain, disability, or dissatisfaction between male and female swimmers. This contradicts previous research findings that female competitive swimmers had a higher prevalence of pain than males.7 More research is needed to assess whether sex differences in shoulder pain, disability, and dissatisfaction exist to raise athletes’ and coaches’ awareness as well as optimize pain prevention strategies.
Limitations
This study has several limitations. While data were captured from a broad geographical area in six states, data from regions in the middle of the country were not represented, and a majority of the participants were from the Western region of the US. In addition, surveys were administered in two different formats: paper and online. The online format allowed for survey distribution to more regions, but research personnel were unable to speak in-person to coaches and teams to explain the study, instead relying on coaches to relay information to their teams and parents. As this research focused on youth across different ages with various levels of comprehension and understanding, survey response accuracy may be a limitation. Another limitation was that a direct comparison to McMaster and Troup5 cannot be made since they also studied swimmers at higher level of competition than the current study with slightly different age groups. Lastly, while some findings were statistically significant, the differences did not reach the thresholds for MDC and SEM, so clinicians should use caution when integrating these results in their clinical decision-making.
CONCLUSION
This survey study of 671 swimmers from six states identified the prevalence of shoulder pain, disability, and dissatisfaction within the four competitive US swimming youth age-groups. Forty-nine percent of swimmers surveyed reported having shoulder symptoms that impacted their swimming. Consistent with prior studies, older swimmers and those with more years of swimming experience had a higher prevalence of shoulder pain and disability, and prior history of shoulder pain or injury was associated with higher rates of current pain and disability. Participation in a second sport other than swimming was associated with increased satisfaction regarding shoulder function. Overall, the current study adds to the body of evidence related to factors and risk profiles of youth swimmers across two regions of the US who report increased shoulder pain and disability. It may guide clinicians and coaches in designing safe and effective performance and rehabilitation programs for swimmers.
Corresponding author
Brian D. Stirling, Stanford Health Care,
Redwood City, CA 94063 United States
Telephone number: +1 (609) 273-2257
Email address: stirlingdpt@gmail.com
Conflicts of Interest
Lori A. Michener serves on the advisory board for Operative versus non-operative treatments for atraumatic rotator cuff tears: a multicenter randomized controlled trial (PI: Nitin Jain, MD, MPH) for NIAMS and PCORI, and she also served as Vice President for the APTA Academy of Orthopedic Physical Therapy from 2017 – 2023. Jonathan C. Sum received USC Division of Biokinesiology and Physical Therapy support for registration and travel for the ASSET Annual Meeting in 2022 and 2023, and serves on the executive board for ASSET as a volunteer.
Acknowledgements
The authors thank Kathryn Ayoob, Anthony Blubello, David Blum, Maggie Bryant, Jocelyn Chang, Jessica Curran, Alyssa Peterson, Jenna (Hankard) Somasundaram, Rini Varghese, Chelsea Weedman, Garin Wyberg, Christine Yim and Bonnie Zeigler for assistance with data collection and organization.