

INTRODUCTION
Posterior shoulder tightness (PST) is defined as soft tissue tightness in the posterior region of the glenohumeral joint, including the infraspinatus, teres minor, and posterior glenohumeral joint capsule.1 This condition has been observed in so-called shoulder range of motion (ROM) disorders, such as frozen shoulder and stiff shoulder, impingement syndrome, rotator cuff tears, anterior instability, and glenohumeral internal rotation deficit (GIRD), among overhead athletes.2,3
PST induces abnormal humeral head motion during shoulder flexion and abduction and is involved in subacromial pain syndrome, thereby affecting shoulder ROM.4–6 It also can cause scapular malposition, which has been identified as a factor in shoulder disorders.7 Aside from pain, this condition also is present in numerous pathological processes in the shoulder, highlighting the importance of treatment, including preventive measures. However, aggressive treatment, such as manipulation or capsular release, is rarely necessary, with most cases showing improvement following with conservative treatment such as physical therapy, massage, and stretching.8,9
Massage and static stretching are typical approaches for improving soft tissue flexibility. However, self-massage may be challenging to perform in certain areas, such as the shoulder region, inhibiting continuous and preventive intervention. Furthermore, several previous studies have reported that 45–60 s of static stretching interventions can potentially decrease muscle force generating capacity, a phenomenon referred to as stretch-induced force deficit.10,11 Therefore, as alternatives to stretching and massage, approaches using vibration have attracted considerable attention in recent years. In fact, recent systematic reviews and meta-analyses showed that vibration therapy for lower extremity muscles reduces stiffness and increases ROM.12,13 Similarly, other authors have suggested that vibration therapy improves flexibility, muscle activation, and maximal voluntary contractility.14,15
Despite the increase in attention directed toward vibration therapy, most studies showing the effects of vibration therapy on stiffness and ROM have been conducted using whole-body vibration or vibrating foam rollers. Moreover, unlike handheld devices, which can easily target specific areas, whole-body vibration or vibration foam rollers make targeting specific areas, such as the soft tissues of the posterior shoulder, quite difficult. A handheld massager is a portable tool that can be used in any environment, including sports stadiums and homes. However, only a few previous studies have investigated the effectiveness of a handheld vibration massager. Konrad et al.,16 who investigated the acute effects of a handheld vibration massager on calf muscles, reported that patients increased their ankle dorsiflexion ROM while maintaining ankle plantar flexion torque. These results are similar to those observed with other vibration therapies, such as whole-body vibration and vibrating foam rollers, and indicate that handheld devices can improve ROM without decreasing muscle activity and maximum voluntary contractile force. The current study extends previous findings and may facilitate the establishment of a new treatment for PST. The authors hypothesized that massage using a handheld vibration tool would increase ROM without decreasing muscle strength.
Thus, the purpose of the current study was to evaluate the effects of vibration massage using a handheld device on the soft tissues of the posterior shoulder joint, particularly on internal rotation (IR) passive ROM and external rotation (ER) muscle strength.
METHODS
Study design
This crossover study examined the effects of vibration massage over the soft tissues of the posterior shoulder on ROM and muscle strength. The dependent variables included IR-ROM and ER muscle strength, whereas the independent variables included the presence or absence of intervention (vibration vs. control) and the time effects before (PRE) and immediately after the intervention (POST).
Participants
This study enrolled 15 healthy men (aged 20.5 ± 1.7 years; height, 169.9 ± 6.3 cm; weight, 62.9 ± 7.4 kg). Participants who had no experience with regular resistance training over the prior six months and had no history of neuromuscular disease or orthopedic neck and upper extremity pain/injury were included. Based on previous studies,16 the sample size required for a two-way repeated-measures analysis of variance (ANOVA) [effect size = 0.40 (large), α error = 0.05, power = 0.80] was calculated using G∗ power 3.1 software (Heinrich Heine University, Düsseldorf, Germany). After calculating the sample size, >14 participants were ultimately needed for analysis.
This study was approved by the Institutional Ethical Review Board and was conducted in accordance with the ethical principles of the Declaration of Helsinki and the Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects. All participants provided written informed consent after being fully informed of the study procedures and objectives.
Procedures
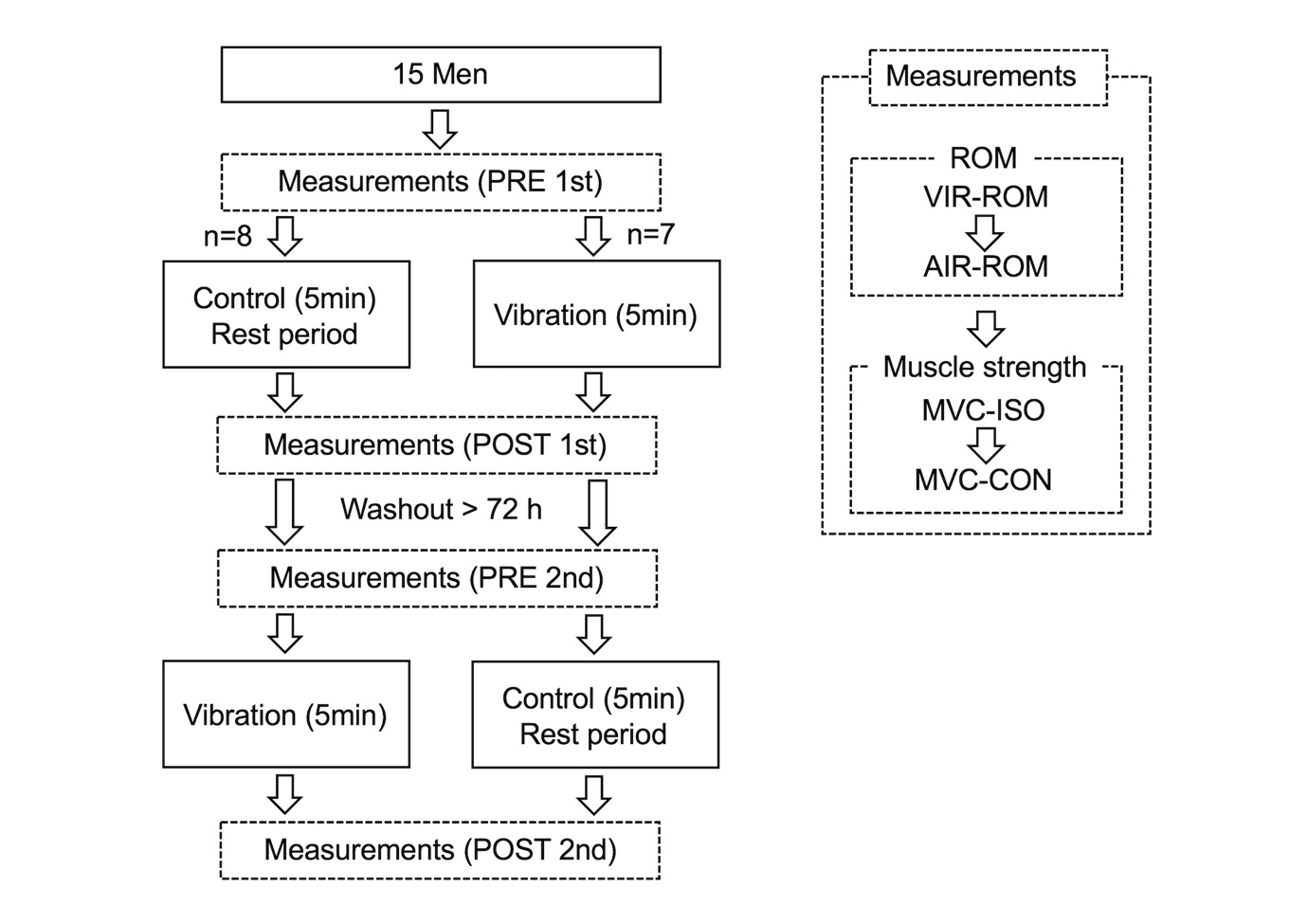
The procedures are illustrated in Figure 1.

Participants were instructed to visit the laboratory twice, at least 72 h apart. Participants were randomly assigned to receive either handheld vibration massage (vibration) or the control condition (no vibration) using the permuted block method. Participants who received the vibration intervention at their first visit were provided the control condition on their second visit. Conversely, participants who received the control condition at the first visit were subsequently provided the vibration intervention at their second visit. Shoulder exercises, including elevation and internal and external rotations, were performed for five minutes prior to measurement. Moreover, isometric and concentric contractions were practiced once each at approximately 30% effort. All outcome variables were measured before (PRE) and after (POST) the intervention. The intervention (vibration or control) was administered immediately after the PRE measurement, and the POST measurement was taken immediately after the intervention. The time taken for participants to complete the PRE measurement, intervention (vibration or control), and POST measurement in one visit was <20 min. The two examiners performing the measurements were blinded to grouping of the participants. In both PRE and POST measurements, (1) passive IR-ROM at the vertebral level reached by the extended thumb (VIR-ROM); (2) passive IR-ROM of the shoulder joint at 90° abduction (AIR-ROM); (3) maximum voluntary contraction in isometric (MVC-ISO); and (4) concentric isokinetic contraction torque (MVC-CON), was measured following this order.
IR-ROM evaluation
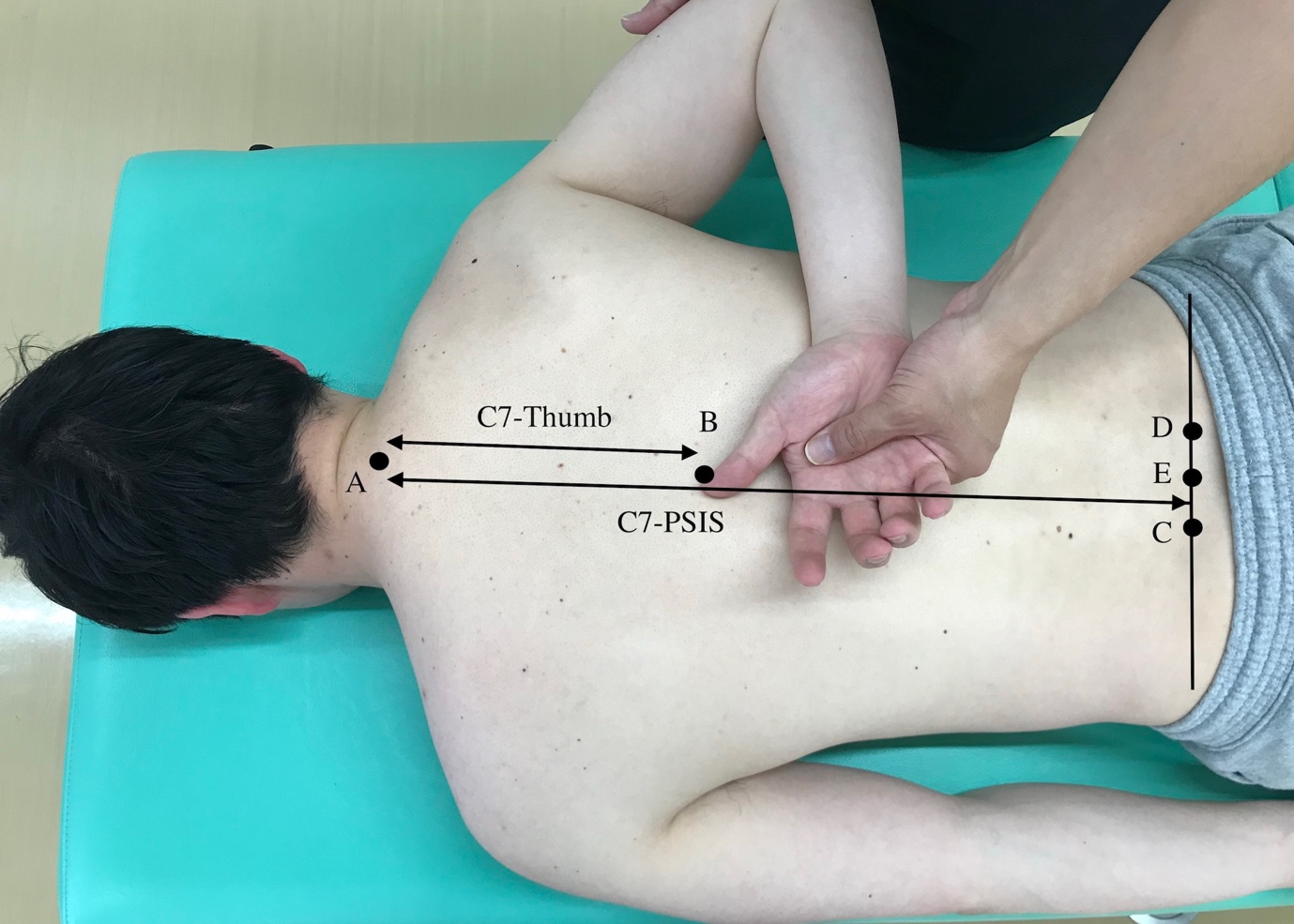
Two shoulder IR-ROM tests, namely VIR-ROM and AIR-ROM, were performed. VIR-ROM is recommended by the American Academy of Orthopedic Surgeons as a measure of shoulder IR-ROM, with reports showing moderate to high intraexaminer reliability.17,18 To obtain normality, VIR-ROM measurements were obtained based on the method described by Mitsukane et al.19 The ratio of “the length between the thumb and the seventh cervical spinous process” to “the length between the middle position of both superior posterior iliac spines and the seventh cervical spinous process” was calculated (Figure 2), with lower ratios indicating greater the ROM. VIR-ROM involves the extension and IR of the glenohumeral joint and is influenced by the extensibility and flexibility of the infraspinatus muscle. It is a static stretching method for the infraspinatus muscle.20 Given that VIR-ROM is also affected by factors other than the glenohumeral joint, such as the elbow, wrist, and thumb, AIR-ROM was also evaluated. AIR-ROM was measured using a digital inclinometer (BEVEL BOX; Niigataseiki, Niigata, Japan) with the patient in the prone position and their shoulder joint in 90° abduction, after which the angle of IR was recorded in 1° increments (Figure 3). The digital inclinometer has a minimum reading of 0.1°, a reading accuracy of ±0.2°, and a repeatability of 0.1°. AIR-ROM was believed to involve stretching only the inferior fiber of the middle and inferior fibers of the infraspinatus.20 AIR-ROM showed high reproducibility as a method of measuring glenohumeral joint IR-ROM given that it controls scapulothoracic joint motion through scapular fixation.21 In this study, the examiner stabilized the coracoid process (scapular movement) using their forearm while also supporting the subject’s distal upper arm with their other hand to measure AIR-ROM with a measurement assistant (Figure 3). These considerations ensured that scapular movement was minimized as much as possible avoid tension in the subject’s periscapular muscles and avoid a shift in the horizontal abduction angle of the glenohumeral joint. In all participants, ROM measurements and measurement assistance were performed by two physical therapists with >10 years of experience in orthopedics.


MVC-ISO and MVC-CON evaluation
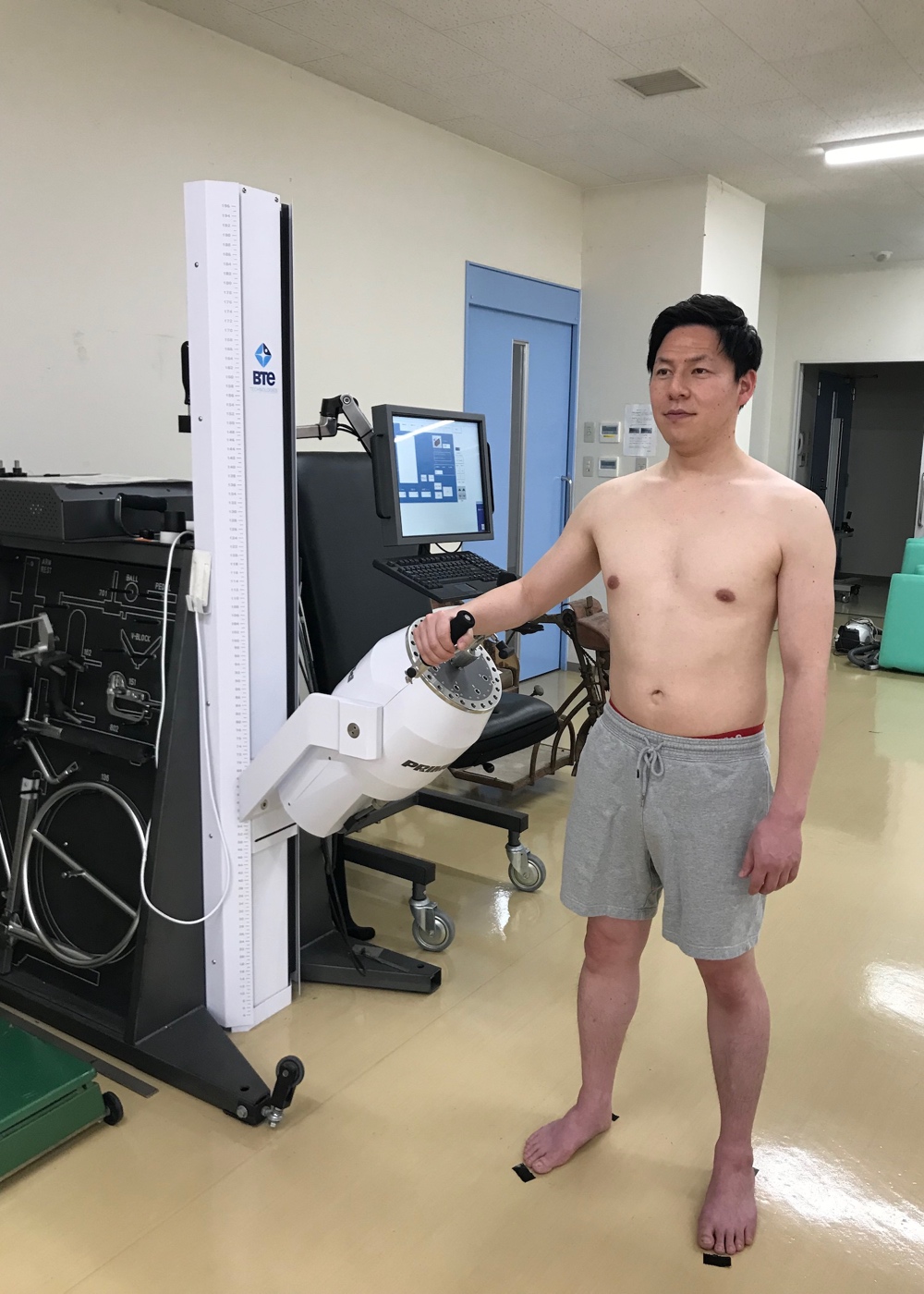
Shoulder ER muscle strength measurements for MVC-ISO and MVC-CON were performed using a dynamometer (Primus RS; BTE Technologies, Hanover, MD, USA) and depicted in Figure 4. According to the Primus RS manual, measurements were obtained in the standing position with their feet shoulder width apart. To ensure that postural changes did not influence PRE and POST measurements, a tape was placed on the floor to standardize the standing position. Participants were also instructed to avoid compensatory movements during measurements. MVC-ISO measurements were performed with the shoulder joint in 45° of abduction, in a neutral position of IR and ER, and with the elbow joint flexed at 90°. MVC-ISO was performed twice, for 6 seconds, with a 60-s rest between efforts, and the maximum value was analyzed. MVC-CON measurements were performed at an angular velocity of 60°/s from 55° IR to 55° ER with the shoulder joint in 45° abduction and the elbow joint in 90° flexion. The examiner encouraged the participants to maximize their effort during muscle contraction. The peak (maximum) torque in three concentric contractions was used as the MVC-CON torque.

Vibration massage
Using the spherical attachment of a handheld vibration massager (Recovery Gun RG-01; Dream Factory, Inc., Osaka, Japan), a vibration frequency of 58 Hz and amplitude of 5 mm, vibration massage was applied over the infraspinatus fossa for five minutes. The frequency and amplitude settings were based on reports showing increases in ROM and muscle strength.14,16,22 The five minute intervention time was based on a previous study in which a handheld vibration massager was used to improve the flexibility of the lower limb muscles.16 Vibration massage was performed in a relaxed prone position (neutral IR and ER positions with 90° shoulder joint abduction) (Figure 5) and initiated just below the scapular spine (head side of the infraspinatus muscle). The vibration massager was moved linearly from distal to proximal and then from proximal to distal within 20 s. The vibration massage started from the head side and ended at the caudal side. The pressure of the vibrating massager was evaluated using a numerical rating scale (NRS). The degree of pressure was numerically quantified by the following descriptors: 0, no pressure; 1, slight pressure; 5, moderate pressure; and 10, very strong pressure. During the massage, the participants were asked to confirm the pressure level through verbal responses while maintaining a consistent pressure level of NRS 5 (moderate pressure). Vibration massage was administered to all participants by one physical therapist (YY) who did not perform ROM and muscle strength measurements. Participants receiving the control condition maintained the same relaxed prone position for five minutes, similar to that in the intervention condition, except that no vibration massage was performed during that time. The instructions for the control condition were provided by the same single physical therapist who performed the vibration massage.

Test–retest reliability of measurements
The test–retest reliability values of VIR-ROM, AIR-ROM, MVC-ISO, and MVC-CON were determined by the coefficient of variation (CV) and intraclass correlation coefficient (ICC) based on the interconnection PRE measurement data of all participants. The CVs were 4.9% ± 3.8%, 3.2% ± 2.8%, 4.1% ± 3.5%, and 6.5% ± 4.4%, whereas the ICCs (1, 1) of the measurements were 0.97, 0.99, 0.93, and 0.82, respectively. Based on the reliability coefficient, the standard error of the measurement (SEM) (Eq. 1) and the 95% confidence interval of the minimum detectable change (MDC), MDC95 (Eq. 2), were calculated.
SEM=SD√1−ICC
MDC95=1.96SEM√2
VIR-ROM had an SEM of 1.2% and MDC95 of 3.2%. AIR-ROM had an SEM of 2.6° and MDC95 of 7.1°.
Statistical analysis
All statistical analyses were conducted using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to confirm the normality of all variables. To analyze interactions and main effects, two-way repeated-measures ANOVA [condition (vibration vs. control) vs. time (PRE vs. POST)] were performed on all variables. After confirming the interaction or main effect, a paired t-test (Bonferroni-corrected) was performed to compare the changes in PRE and POST values in both conditions, PRE and POST values between conditions, and POST and POST values between conditions. The effect size [partialη2 (ηp2), Cohen’s d] was calculated as the difference in means divided by the pooled standard deviation (SD), with effect sizes of 0.00–0.19, 0.20–0.49, 0.50–0.79, and ≥0.80 being considered trivial, small, moderate, and large, respectively.23 A p value of <0.05 indicated statistically significant differences. Descriptive data were reported as mean ± SD.
RESULTS
The results are presented in Table 1. Shapiro–Wilk test confirmed normality of all variables. Repeated-measures ANOVA showed a significant interaction [F = 17.6, p = 0.001, ηp2 = 0.556] and time (F = 42.9, p < 0.001, ηp2 = 0.754) effect for VIR-ROM; however, no between-condition effect (F = 2.64, p = 0.127, ηp2 = 0.159) was observed. The posthoc test showed a significant change in VIR-ROM (−4.1%, p < 0.001, d = 0.445) in the vibration condition but not in the control condition (−1.7%, p = 0.052, d = 0.169). Preintervention comparison of the two conditions showed no significant difference (p = 1.000), whereas postintervention comparison showed significantly greater ROM in the vibration condition than in the control condition (p = 0.036, d = 0.273).
AIR-ROM ANOVA revealed significant interaction (F = 15.3, p = 0.002, ηp2 = 0.523) and time (F = 48.9, p < 0.001, ηp2 = 0.777) effects; however, a between-condition effect (F = 2.68, p = 0.124, ηp2 = 0.161) was not observed. The posthoc test showed a significant change in AIR-ROM (+11.4°, p < 0.001, d = 0.694) in the vibration condition but not in the control condition (+2.8°, p = 0.096, d = 0.232). Preintervention comparison of the two conditions showed no significant difference (p = 1.000), whereas postintervention comparison showed significantly greater ROM in the vibration condition than in the control condition (p = 0.048, d = 0.483).
MVC-ISO ANOVA showed no significant interaction (F = 0.004, p = 0.951, ηp2 < 0.001), time (F = 2.79, p = 0.117, ηp2 = 0.166), or between-condition (F = 0.019, p = 0.892, ηp2 = 0.001) effects. MVC-CON ANOVA showed no significant interaction (F = 0.101, p = 0.755, ηp2 = 0.007), time (F = 1.061, p = 0.321, ηp2 = 0.07), or between-condition (F = 0.651, p = 0.433, ηp2 = 0.044) effects.
DISCUSSION
The current study examined the effects of a handheld vibration massage to the posterior shoulder soft tissues on IR-ROM and ER MVC torque. Notably, the results indicate that a handheld vibration massage increased the IR-ROM without negatively effecting the MVC torque. The current study demonstrates of the usefulness of a handheld vibration massage device as an intervention for shoulder joint stiffness and extends previous research focused on whole-body vibration stimulation and lower extremity muscles.
Conventional mechanisms proposed to explain the increase in ROM after massage include biomechanical (decreased muscle contraction), physiological (increased blood flow), neurological (decreased pain perception), and psychophysiological (increased relaxation) changes.24 Vibration massage also creates pressure and friction in the treated skin, fascia, and muscles, which may affect tissue viscosity and decrease resistance to joint motion. Moreover, studies have shown that vibration therapy had an effect on decreasing pain perception.25,26 Despite the unknown details regarding the mechanism underlying increased ROM, ROM changes after a handheld vibration massage may be associated with decreased muscle stiffness and pain perception changes.
Cross-body stretching and sleeper stretching are common interventional strategies that have been shown to improve IR-ROM by 3.1°–11.0° immediately after the intervention.27,28 Furthermore, one report showed that combining soft tissue mobilization and stretching promoted a 12.1° improvement of IR-ROM after the intervention.29 The current study demonstrated that a 5 minute application of a vibration massage to the soft tissues of the posterior shoulder promoted an ROM expansion of 4.1% in VIR-ROM and 11.4° in AIR-ROM, with the changes in both variables exceeding the MDC95 range. These results demonstrate improvements comparable to those reported in previous studies, further indicating the potential for expanding interventions targeting the soft tissues of the posterior shoulder. Vibration interventions for shoulder joint ROM have been reported to be as effective in improving ROM as stretching and proprioceptive neuromuscular facilitation.30 However, these reports differ from the present study in that they applied vibration to the shoulder joint from a vibration table via the hand or forearm, (i.e., indirectly to the shoulder joint). In the present study, vibration massage was applied directly to the posterior shoulder soft tissues, after which ROM increase was confirmed. Based on these findings, vibration has the potential to increase ROM through both direct and indirect stimulation methods to the intervention site.
The present study found no MVC changes after the handheld vibration massage, which supports the results of a previous study using a similar device on the calf.16 However, the mechanical vibration theory states that handheld vibration massage can induce tonic vibration reflex contraction of the muscle.15 This mechanism is stimulated by a sequence of rapid muscle stretches that occur during vibration, triggering muscle spindles, which subsequently induce involuntary muscle force production.15 However, no significant changes in muscle strength were found after the vibration intervention. Although this study provided the intervention at a frequency of 58 Hz, amplitude of 5 mm, and stimulation duration of 5 minutes, changes in these parameters may have influenced the effects on muscle strength.14 Therefore, future studies are needed to investigate the effects of various vibration parameters on muscle strength.
Previous authors have shown that the throwing side of overhead athletes presents with reduced IR-ROM compared to their non-throwing side and that of normal individuals.31 Furthermore, restrictions in shoulder joint ROM and reduced ER strength have been identified as risk factors for overhead athletes,32 and PST has been shown to influence kinematic changes in the glenohumeral joint.5,33,34 Thus, massage and static stretching are commonly employed to address ROM and stiffness. However, self-massage may be difficult in certain areas, such as the shoulders, hindering ongoing and preventive interventions. Moreover, although static stretching has been commonly implemented to improve ROM and muscle stiffness, the decrease in muscle strength for a certain duration during warm-up has remained a primary concern.10,11 The infraspinatus and teres minor muscles (the target soft tissues of the posterior shoulder) exhibit high muscle activity reaching 74% and 71% of the maximum voluntary muscle contraction during the cocking phase of the overhead throwing motion, respectively, when pain and injury are likely to occur in the throwing motion.35 Therefore, the soft tissues of the posterior shoulder should be the focus of injury prevention given that they are required for both flexibility and stability. Considering these factors, improving flexibility without causing muscle weakness is imperative during warm-up. The results of the current study indicate that a handheld vibration massage is effective in improving ROM without negatively affecting muscle strength. In other words, it can be used for warming up.
The handheld device is easy to carry, can be used in any setting, including sports stadiums and homes, and is easily used in sports and rehabilitation settings. In the current study, the intervention was conducted by only one examiner to achieve reproducibility of the intervention. In practice, however, the described intervention is intended for individuals to employ for self-care. In essence, self-management is important and should be further investigated using self-administration of a vibrational device.
The current study has several limitations worth noting. First, the study population included only healthy men. As such, further investigations are required on athletes, those who perform overhead activity, or those with PST and GIRD, who may demonstrate different results. In the current study, vibration massage was applied to the entire infraspinatus fossa. Therefore, the possibility that the applied vibration may have affected not only the infraspinatus muscle but also the posterior articular capsule via the teres minor and scapula cannot be overlooked. Regarding stimulation pressure, moderate pressure (NRS 5) was used as the standard and this standardization relied on the subjective reports of the participants. Therefore, slight differences in the sensation of pressure reported between participants could have been present. Finally, this study only examined the acute effects of vibration massage on ROM and muscle strength. Previous studies on interventions aiming to improve flexibility, such as stretching and massage, have examined duration of improvement, long-term intervention effects, pain relief, and muscle stiffness. These effects of handheld vibration massage remain unclear and require further investigations.
CONCLUSIONS
A single five minute session with a handheld vibration massage device applied to the soft tissues of the posterior shoulder increased IR ROM without negatively affecting muscle strength. The results presented herein indicate that a handheld vibration massage can be used for warming up.