INTRODUCTION
Despite increasing participation across the lifespan of females in sport and recreational activity, evidence regarding guided musculoskeletal rehabilitation for the athlete mother is limited.1 The benefits of exercise during pregnancy are well known, yet lack of awareness regarding appropriate training protocols may continue to contribute to the low percentage of women achieving the current recommended physical activity guidelines.2,3 The American College of Obstetricians and Gynecologists (ACOG) has recently updated guidance for exercise with suggestions for pregnant athletes.4 These exercise recommendations are based solely on medical health, and while appropriate to protect the medical status of baby and mother, lack a clear focus on musculoskeletal health or appropriate timeline for returning to activity.4 Current ACOG recommendations do not discuss the increased demands placed on the musculoskeletal system and the stress pregnancy places on the pelvic floor in relationship to exercise. As more evidence-based suggestions for safe and holistic movement during the perinatal period continues to develop, special attention to musculoskeletal health and progression of exercise is warranted in the relatively vulnerable period of pregnancy and postpartum.5–7
Commonly experienced postpartum symptoms such as pelvic floor dysfunction, urinary incontinence, and pain can interfere with athletic performance.1 Physical therapy in the treatment of pelvic floor dysfunction has been well established, but is not currently considered standard of care for recreational or elite athletes during pregnancy and postpartum.8 Presently, there are no musculoskeletal-specific guidelines to address symptoms from the onset of pregnancy through the completion of the first three months postpartum (often referred to as the fourth trimester). Conflicting recommendations that do not delineate the postnatal medical vs. musculoskeletal clearance may result in either overly conservative or zealousness approaches to recovery, leaving mothers to navigate this fourth trimester independently despite the incredible amount of anatomical and physiological healing taking place.9 Understanding of appropriate and safe exercise, neuromuscular control, and pelvic floor-specific considerations in during pregnancy and postpartum may allow athletes to better maintain strength and conditioning throughout pregnancy as well as promote a timely return to sport and minimize postpartum symptoms.
Athlete mothers may require more specific guidance on returning to impact tasks then the general population during performance of independent training regimens and the maintenance of resistance training.4 A clear timeline related to the progression of exercise may assist clinicians and coaches with appropriate guidance to maximize sport and activity performance. The range of women, clinicians, and coaches who are unaware of the proposed rehabilitation timeline is significant, and continuous longitudinal assessments and modifications of protocols such as this may prompt larger and more specific studies to help eliminate the either/or distinction of athlete vs. mother. Therefore, the purpose of this case series is to assess pelvic floor symptoms through implementing a new pre- and postnatal exercise training paradigm in a group of women aiming to return to recreational athletics.
METHODS
Participants
Participants of this study were electively undergoing physical therapy treatment as a preventative musculoskeletal measure beginning in pregnancy. Participants were included as a sample of convenience if they were pregnant women between the ages of 25 and 35 and considered a low-risk pregnancy. Participants completed at least one in-person visit per trimester. All participants performed regular independent exercise programs prior to pregnancy including impact work such as running, ranging between 5-20 miles/week for at least three months prior to pregnancy. All participants regularly met ACSM guidelines for activity for at least three months prior to pregnancy and were meant to represent a field of recreational athlete mothers not specific to any individual sport. Exercise participation prior to this study included a variety of recreational tasks including running, CrossFit, HIIT training, and strength training as desired by each individual.
It should be noted that all participants described varying levels of occasional stress incontinence, heaviness and pressure (prolapse-related symptoms), and varying levels of pain in their current pregnancies prior to the start of this protocol. Exclusion criteria from the present study included Grade 4 perineal tearing during delivery and high-risk pregnancies. The U.S. Health Insurance Portability and Accountability Act (HIPPA) was discussed, and informed consent obtained from all participants to allow for the use of medical information. All participants in this case series were informed that the data collected would be submitted for publication, and the study was approved by the local institutional review board.
Procedures
Women participated both during and after pregnancy in the previously published protocol.10 Participants all worked with the same physical therapist for the entirety of their care, who had training specific to pre- and postnatal interventions through specialization from Herman and Wallace Pelvic Rehabilitation Institute. Participants attended an average of one physical therapy visit per trimester prior to delivery. Based on the anatomical and physiologic healing time frames, participants avoided high impact tasks (described clinically as “anything leaving the ground” such as jumping, running) until cleared by the pelvic floor physical therapist. Participants attended an average of eight physical therapy visits after delivery beginning as early as two weeks postpartum and continuing until at latest 16 weeks postpartum. In addition to the postpartum physical therapy visits, each participant was provided with a home exercise program with video guidance from an author-developed program on Medbridge (Table 1) during the 0-6 week postpartum period with internal muscle exam performed by the physical therapist after the six-weeks postpartum physician clearance. During weeks 6-12 postpartum, patients attended in-clinic physical therapy between one to two times per week with discharge ranging between weeks 12-16 postpartum. Time until discharge varied between participants depending on their progression through the rehabilitation program and ability to meet the markers for readiness to progress. Outcomes of the study were measured at six weeks postpartum and discharge (12-16 weeks). Criteria for discharge included asymptomatic independence in desired exercise program (varying from CrossFit to HIIT training) as well as asymptomatic running performance for individually desired distances.
Outcomes
Symptoms of pelvic floor dysfunction
Symptoms of pelvic floor dysfunction were monitored and adjusted for in the postpartum group to assist with readiness for progression into the next phase of rehabilitation. These symptoms were based on patient subjective reports and patients were instructed to either continue forward with the protocol or instructed to repeat movements from a previous session until asymptomatic depending on the discretion and expertise of the clinician. These symptoms included urinary and/or fecal incontinence, urinary and/or fecal urgency, symptoms of prolapse, pain with intercourse, and musculoskeletal lumbopelvic pain.5 This is not an all-inclusive list of signs of pelvic floor dysfunction, but they are main markers for dysfunction that may limit progression in exercise. As with any protocol, presence of any of these symptoms in isolation may not necessarily be grounds to halt progression but should be monitored and accounted for by the licensed professional supervising the protocol. Any ongoing or onset of vaginal bleeding not related to the menstrual cycle during or after an attempted low impact or high impact exercise was to be utilized as an immediate referral back to the participant’s obstetrician/gynecologist.5 However, no participants experienced vaginal bleeding during the course of the rehabilitation.
Functional and other outcomes
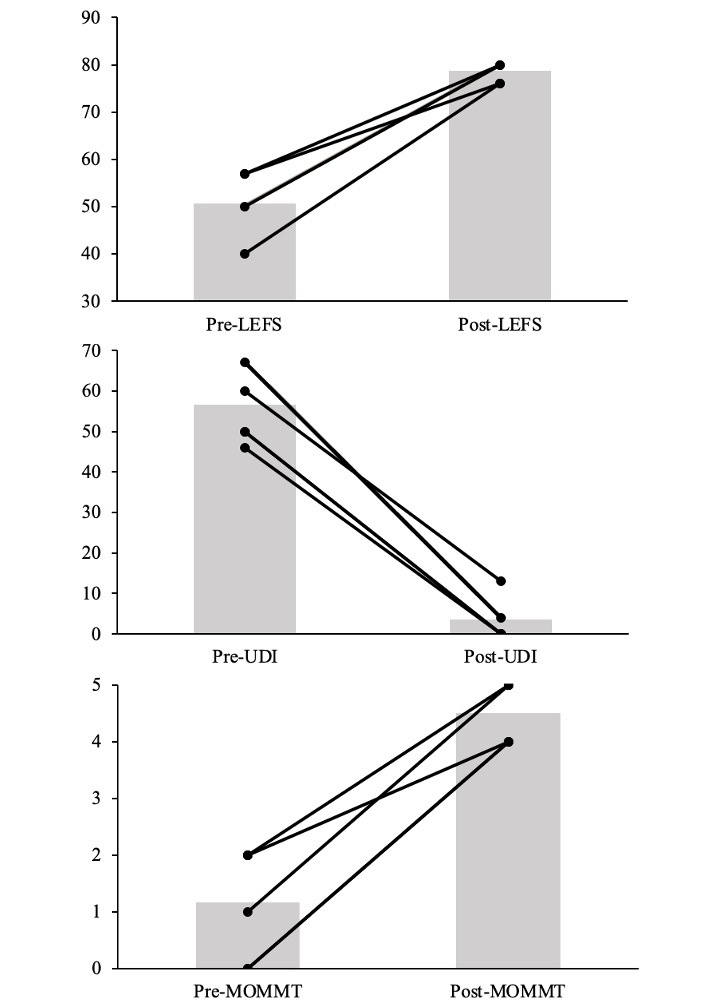
The lower extremity functional scale (LEFS) is a functional questionnaire focused on the ability of the participant with consideration to lower body dysfunction.11 Questions include tasks such as housework, sport participation, walking, stairs, running, and hopping. The LEFS is scored out of 80 points, with a higher score suggesting greater function and less disability. LEFS was used to determine a percentage of disability. Minimal clinically important difference requires a change in score by 9 points or greater to indicate significant change in function.11
The urinary distress inventory short form (UDI-6) is a six question form meant to assess the life quality and symptom related distress of women suffering from urinary incontinence.12 The UDI-6 is scored out of 100, with a higher score suggesting greater urinary distress. Minimal clinically important difference requires a change in score by 11 points or greater to indicate statistically significant change in function.12
Lastly, the modified Oxford grading system (MOMMT) was used to evaluate the strength of the pelvic floor by vaginal palpation. The grading score is described as the following: 0 = no contraction, 1 = flicker, 2 = weak, 3 = moderate, 4 = good (with lift) and 5 = strong (with lift). Inter-rater reliability for this measure is high (95% confidence interval) and this is a widely used and recognized method for strength grading for this musculature.13
Initial evaluation of patients in the postpartum period focused solely on external musculoskeletal approaches prior to the six-week postpartum mark as listed in the recommended protocol. After medical follow up at six-weeks postpartum, each patient consented to an internal (vaginal) muscle exam to determine baseline strength, endurance, and to assess any notable tenderness to palpation that may indicate myofascial trigger points and associated dysfunction at the pelvic floor musculature. Based on this exam, deficits were addressed throughout the 6-12 week protocol recommendations with individualized treatment dependent on baseline muscle performance. While some participants were noted to have underactive pelvic floor musculature post-delivery, others were noted to have overactive pelvic floor musculature and this clinical information was used as an adjunct to supplement completion of the suggested protocol. For example, for participants who were noted to have increased pelvic floor musculature tone at six-week postpartum assessment, increased focus was placed on relaxation of the pelvic floor musculature throughout their plan of care. Vice versa, those who were noted to have underactive decreased pelvic floor musculature tone at this check-in were guided to include supplemental contract/overflow tasks of the pelvic floor. This variation in presentation emphasizes the importance of a qualified pelvic health physical therapist to better individualize the suggested protocol for each athlete.
RESULTS
Of the six participants, two mothers were primipara and four mothers considered multipara. All mothers had a vaginal delivery. Participants were discharged between the 12-16 week postpartum mark at which point all were participating in their desired exercise programs without pain, urinary dysfunction, or prolapse during performance. These exercise programs included group fitness such as CrossFit and local HIIT training in addition to individual running programs for varying distances.
At the time of discharge, all six participants improved their LEFS, UDI and MOMMT scores (Table 2). The LEFS assessment improved by 28 points on average, suggesting a meaningful clinical difference from pre- to post-rehabilitation. The UDI improved on average 53 points, also suggesting a clinically significant change from pre- to post-rehabilitation. All individuals improved MOMMT scores at the time of discharge, with good to strong lift of the pelvic floor muscles (Figure 1).
.png)
DISCUSSION
Evidence for pelvic floor physical therapy itself has been well established for the management of urinary incontinence, pelvic organ prolapse, sexual dysfunction, and the prevention of pelvic organ prolapse.14–17 Despite this evidence, no specific pre- and postnatal musculoskeletal rehabilitation guidelines currently exist to assist clinicians in determining rehabilitation frequency or exercise progressions. The lack of information in this realm may be limiting a potential change in standard of care encouraging referral to physical therapy upon determination of viable pregnancy. These results of this case series suggest that pregnant and postpartum athletes benefit from a guided rehabilitation program for the management and improvement of common postpartum symptoms, which may also limit the continuation of symptoms into their goal of returning to sport.
Postpartum urinary incontinence creates a barrier to exercise, limiting women from participating in an exercise program and may encourage avoidance in regards to strength training tasks.18 While few athletes experience stress incontinence prior to pregnancy and childbirth, a significant amount of women experience incontinence during pregnancy.19 Previous authors have found the presence of incontinence during pregnancy to be indicative of the presence of incontinence in the postpartum period, with athletes experiencing a greater likelihood of incontinence persisting up to five years postpartum.20 The completion of the exercise program and timeline to return to activity utilized in this study resulted in each of the participants fully returning to their desired activity levels without notable symptoms of incontinence or pain by the four-month postpartum mark. At time of discharge from this rehabilitation protocol, no participants were experiencing incontinence symptoms. The exercise program during pregnancy may have allowed for easier and faster establishment of strength, endurance and neuromotor control of the pelvic floor muscles, however this cannot be determined by this case series design. Functionally, participants had improved LEFS scores after the exercise program at the time of discharge. As pregnant and postpartum women have higher incidence of leg pain than non-pregnant women, this outcome emphasizes the importance of an establishing a rehabilitation timeline before postpartum.21
Utilizing a pelvic health physical therapist for the pregnancy and postpartum period appears to be beneficial to the six women included in this case series, via the assessed outcomes. A guided rehabilitation model as the standard of care can help to ensure that the pelvic floor muscles are both contracting and relaxing correctly. In addition, a specialized physical therapist can help to assess the need for appropriate focus on up-training or down-training the musculature of the pelvic floor, which would limit incorrect performance of strength and mobility work leading to undesired symptoms. The importance of this case series not only lies in the description of a preventative approach to maternal care, but also highlights the importance of continuous reassessment of the changing body throughout the pregnant and early postpartum periods as athletes work to continue and return to sport participation.
LIMITATIONS
The scope of this rehabilitation protocol is to provide a starting point for exercise prescription in postpartum women and should be personalized for each individual by an appropriate provider or pelvic health physical therapist. Each phase should ideally be monitored by a pelvic health physical therapist who can best make determinations on readiness to progress through exercise. Due to the limitations of a case series, there is not a way to determine if other exercise rehabilitation approaches would have elicited similar changes in postpartum symptoms. While these guidelines establish a musculoskeletal progression, it does not consider the individual’s needs related to varying degrees of vaginal tearing and/or cesarean-section delivery. Participants entered at different points in their pregnancy with different, but common, incoming symptoms. Thus, a more controlled approach to evaluating their prenatal symptoms is warranted. This small sample of women considered low-risk pregnancies (vaginal deliveries and no cesarean sections), which limits the conclusions that can be drawn from the results, and cause and effect cannot be assumed. These methods should continue to be studied on larger and varying populations. Additional research should also be performed to improve more specific care considerations for women after cesarean-section deliveries and various degrees of vaginal tearing during vaginal births.
CONCLUSION
The potential benefits of pelvic floor rehabilitation and exercise training during the pregnant and postpartum period cannot be neglected. The results of this case series suggest that a graded rehabilitation program during postpartum period improved symptoms of incontinence, prolapse, and pain in the athlete mother. In addition, a structured approach to modifications and interventions in the prenatal period may have positively affected outcomes postpartum although more work must be done here to determine the effects of such an approach. An exercise prescription protocol specialized to pregnant and postpartum athletes may help women to maintain fitness, minimize postpartum symptoms that interfere with exercise, and ultimately return them to sport in a safe manner.
Conflicts of Interest
The Authors report no conflicts of interest.