INTRODUCTION
One in every 29 female athletes and 1 in every 50 male athletes sustain an anterior cruciate ligament (ACL) rupture of the knee during participation in sports.1 Most of these injuries and subsequent ACL reconstructions (ACLR) occur in young individuals who intend to return to their previous level of sport or physical activity.2,3 Unfortunately, only 76% of these athletes are able to achieve successful return to preinjury level, with up to 35% reporting decreased performance upon return.4 Further, research has shown a progressive decline in volume of overall physical activity as early as two years after returning to sports.5–7 Consequently, the inability to achieve or maintain previous level of sport participation following surgery can lead to a destructive cascade of psychological stress, decreased knee-related health, and reduced quality of life.8,9
The complexity of an ACL injury and subsequent ACLR impacts each young athlete differently, particularly when considering the interaction of factors within the five socioecological levels of influence thought to impact health: intrapersonal, interpersonal, organizational, community, and policy.10,11 Yet, very little is known about how young athletes perceive these factors to impact their engagement in sports and physical activity in the years following ACLR and across their lifespan. Quantitative methods are often unable to capture all factors that influence outcomes following ACLR, such as the patient’s perception of their experience, what meaning he or she attributes to the phenomenon, or how the patient’s worldview is constructed following surgery.12 By contrast, qualitative research methods allow for an exploration of patient perspectives that can illuminate the meaning of an experience or phenomenon (e.g. physical activity participation after ACLR). Insights gained from the use of qualitative methods allow for the exploration of complex human beliefs, attitudes, and behaviors that can generate a deeper understanding of the patient experience.
As such, the purpose of this qualitative study was to answer the research question, “what are the lived experiences and perceptions of factors that facilitate or hinder physical activity among young athletes following ACLR?” Improved understanding of patient perspectives following ACLR can shed light on the factors perceived to facilitate or hinder physical activity participation among this population. In turn, this insight has the potential to inform the development of necessary interventions and services that will improve the return to sport process and optimize long-term physical activity participation.
METHODS
Study Design
This study was part of a larger qualitative study of outcomes after ACLR, which employed a phenomenological approach with semi-structured interviews. A phenomenological approach was selected for the study design to allow for learning from the “lived experiences” of individuals in the post-recovery phases after ACLR. An interpretivist epistemology was used to understand how participants experience the phenomenon of physical activity after ACLR through their senses.12 This perspective enables the gathering of the subjective meanings of experiences constructed by participants, recognizing that multiple realities exist.12,13
All research conducted in this study was in accordance with Cincinnati Children’s Hospital institutional review board’s approval. The Standards for Reporting Qualitative Research was used to guide the reporting of study methods and results.14 Funders played no role in the design, conduct, or reporting of this study.
Sample
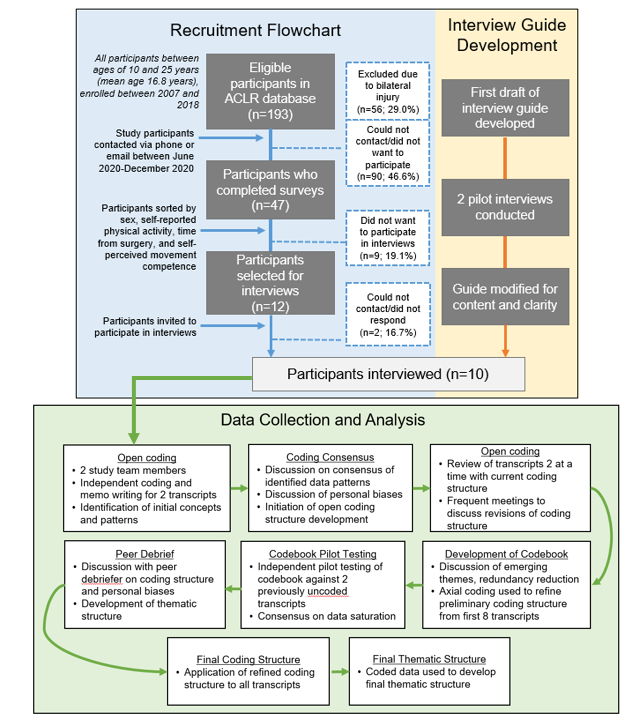
A non-probability, purposive sampling method was utilized to ensure a diversity of perspectives and experiences following ACLR. Ten participants were recruited from an existing research database of individuals between the ages of 10 and 25 at time of return to sport after ACLR (Figure 1).15,16 Informed consent was obtained from all participants.
__development_of_semi-s.png)
Data Collection
An interview guide was developed to evaluate factors related to physical activity participation across levels of the Socioecological Model (Figure 1; Appendix A: Interview Guide).10,11 Prior to study enrollment, the research team conducted two pilot interviews in order to assess the semi-structured interview guide for content and clarity, and modify as needed. Interviews were conducted between December 2020 and February 2021 by the primary investigator, a clinician with 9+ years of experience in pediatric sports medicine. All interviews took place via video conferencing software. The interview audio recordings were transcribed verbatim by the use of dictation software (Zoom Video Communications, Inc.). Participant names were replaced with an alias for data analysis and reporting.
Data Analysis
Following the procedures of collaborative qualitative analysis (CQA),17 data collection and analysis were performed until saturation was achieved, defined as the degree to which new data repeat what was expressed in previous data.18 The two independent coders who engaged in iterative analysis of the data for this study were physical therapists trained in qualitative methods without history of ACLR. The steps of data analysis are shown in Figure 1. The final codebook was applied to the entire dataset and the data was organized using NVivo data management software (QSR International, 2021). The study team members then used all coded data to develop a thematic structure with themes and subthemes derived from the participants’ perspectives.
Strategies for Achieving Trustworthiness of Analyses
Credibility, or the extent to which the research findings are congruent with reality,12 was ensured during the processes of open coding and codebook development, when a peer debriefer was invited to provide feedback based on her perspectives. The peer debriefer for this study was a clinician researcher with expertise in qualitative methods and personal history of ACLR. An electronic audit trail was completed in order to ensure dependability, or the extent to which the results of the study are consistent with the data collected.12,13 To ensure transferability, rich and thick verbatim descriptions were used to describe participants and results of the study through utilization of evidence presented in the form of quotes from interviews.13 Reflexivity of research team biases expected to influence data collection and analysis was maintained throughout the research process by way of frequent inquiry and discussion.
RESULTS
Participant Characteristics
Ten participants (6 female, 4 male) completed interviews for this study (Table 1). Median time between ACLR and interview was 5.9 years (range: 4.3-10.2 years).
A description of the situatedness of a research study within the contexts of the investigators, participants, and time period is necessary to ensure transferability of qualitative work.20,21 All research participants were interviewed 9-11 months into the global COVID-19 pandemic when most state governments were recommending or enforcing preventative measures such as social distancing, capacity limits, and mask-wearing. Many gyms, schools, and facilities were either closed or operating at a reduced capacity in accordance with public health guidelines.
Themes
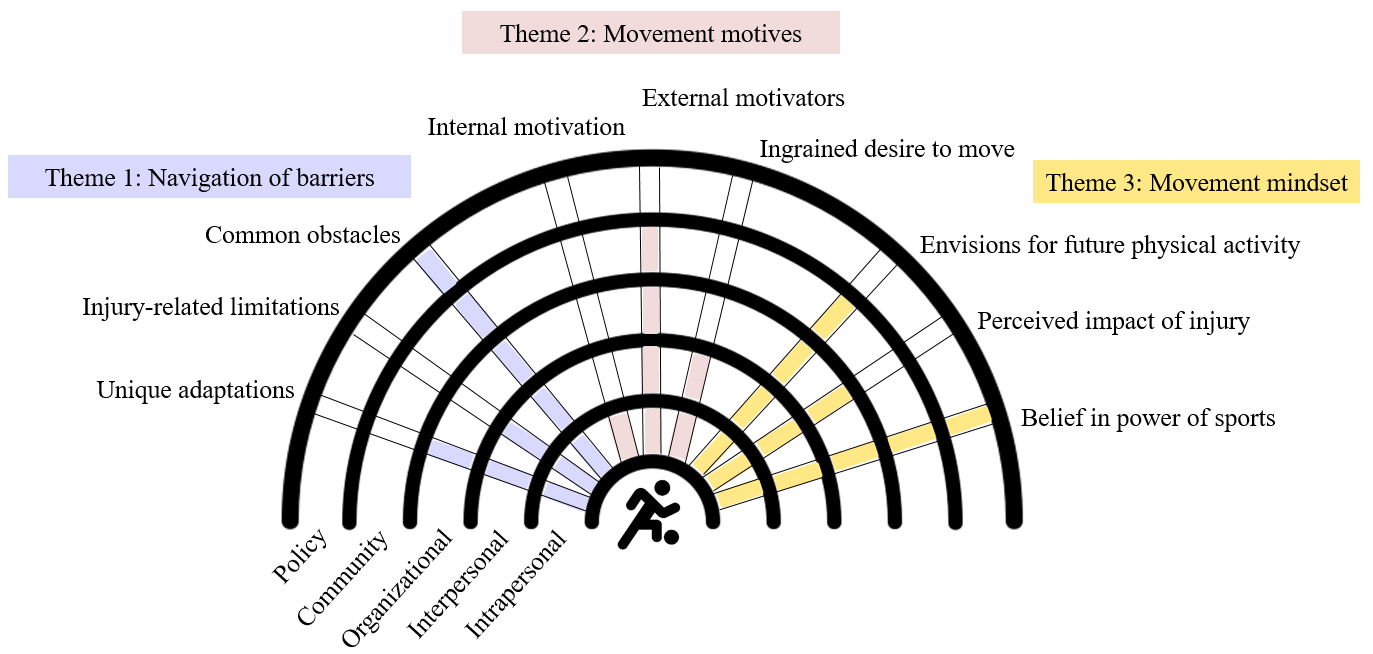
Three overarching themes were identified during data analysis: 1) navigation of barriers, 2) movement motives, and 3) movement mindset. Several subthemes associated with each of the three primary themes were also identified (Figure 2). An overview of each theme and associated subthemes is summarized below, with representative quotes reported in Table 2. Factors perceived to influence physical activity after ACLR were categorized according to levels of the socioecological model. This depiction and examples of perceived factors within each socioecological level are shown in Figure 2 and Table 3, respectively.

Navigation of Barriers
Common obstacles
All participants discussed perceived barriers to physical activity participation in the years following ACLR, including poor weather, lack of resources, and general discomfort in the workout environment. Most common was a perceived lack of time to work towards physical activity goals, often a result of the rapid school- and work-related transitions experienced during the young adult years. As one participant who recently took on a new internship reported, “I do still try to stay active. I go to the gym at least two, three times every week. With working co-op, I haven’t been able to go as much,” (Mikey). For participants no longer involved in organized sports, finding the motivation to stick to an exercise schedule on their own was perceived as a continual challenge (Quote 1.2., Table 2).
Injury-related limitations
Many participants acknowledged physical limitations as barriers to their current physical activity. Perceived to have originated from the ACL injury and subsequent recovery process, these limitations were described as giving-way episodes (Ruth), decreased strength (Stella, Mikey), early fatigue (Ruth, Kate), soreness (Kate, Garrett), tightness (Garrett), and limited range of motion (Juan). These physical barriers often influenced physical activity choices and triggered the perception that the knee still needed to be catered to. Garrett explains,
“it was my right knee that was operated on, so that kind of shoots up into my hip where, you know, if I don’t stretch adequately enough, it’ll tighten up really, really fast. Which will then translate into lower back pain on my right side. So, having to be extremely mindful of what I’m doing and making sure I stretch enough prior to any sort of physical activity.”
Also sparked by the original ACL injury, fear of reinjury was another barrier perceived to influence physical activity choices. In the years following ACLR, some of the participants opted out of their preferred sport in order to avoid another injury. Others voiced a hesitancy to try new sports for the same reason, as “something awful can go wrong,” when trying something for the first time (Juan).
Unique adaptations
In response to the injury-related factors perceived to hinder physical activity, participants made activity-related adjustments to meet their own needs and expectations. Most described a unique awareness of the body post-injury, along with its abilities and limitations when engaging in physical activity. This awareness was often described as having a positive effect on one’s physical activity journey. One participant reported, “if I weren’t to have like an ACL injury, I probably would be doing like…some bad type of exercise, workout, diet. But now I feel like I’m very much aware of things like that and…I just pay more attention,” (Stella). The cohort described how this unique awareness and their appraisal of risk dictated their physical activity behaviors, such as the desire to continue wearing a knee brace. A broad perspective of the potential implications of a second injury was also present among the athletes who exercised risk appraisal. Garrett explained why he no longer participates in pickup basketball in Quote 1.5., Table 2. Other participants recognized that moving with hesitancy may also place them at risk of further injury. “You’re going to get hurt if you’re nervous. You just gotta go full in,” (Joe).
Movement Motives
Ingrained desire to move
The strength of athlete identity was diverse within the cohort. Some participants held tightly to their identity as a “mover,” while others admitted that past or current participation in sports wasn’t integral to their current “self,” despite participation in athletic competitions throughout childhood and adolescence. Regardless of the strength of athlete identity, all participants expressed an ingrained desire to be active, reinforced by Mia’s statement, “[being active] kind of makes your personality.” Many described a shift in the meaning of sports since their time as a young athlete. Among those no longer competing, some of the participants who experienced this shift were motivated to find activities that replaced the elements of sport they found to be most meaningful. For others, this shift in the meaning of sport did not derail the desire to remain active, but rather set them on a new “learning curve” for life after youth sports (Kate). Perceived barriers to physical activity participation were often overshadowed by factors perceived to facilitate a movement-based lifestyle.
Internal motivation
Intrinsically, movement was perceived to be essential to the participants’ mental wellness and day-to-day function. Participants perceived physical activity to provide them with significant physical benefits, both aesthetic and health related. When explaining what value she gets from being physically active, one participant reports, “I guess just how you feel after working out. You feel accomplished and like you’ve done something for yourself. It’s kind of like self-care,” (Nelle). For most, physical activity was perceived as a critical means of relieving stress. Many described a heightened sensitivity to periods of decreased activity, which often served as catalysts for movement. One participant describes this feeling as, “if I haven’t worked out in a while, I start to feel slow, I start to feel kind of heavy. I feel tired, and I’m like, ‘Okay, maybe I need to get kind of back into working out,’” (Stella). Some even recalled a specific event that served as a positive tipping point in their physical activity journey after ACLR (Quote 2.3., Table 2).
In addition to the perceived mental and physical benefits of physical activity participation, the cohort spoke at length about the many other intrinsic factors that motivate them to move. Most participants found pure enjoyment in movement. For sports-related activities and solo workouts alike, “fun” was often used to describe the feeling of engaging in physical movement. Betterment of oneself was also a motivating factor for physical activity. Some participants voiced the desire to meet personal physical goals, such as gain or maintain a starting position on a team (Joe, Mia), learn new physical skills (Kate), or optimize physical performance (Olive, Mikey). Others have found motivation in competing with themselves when competing against sports opponents is no longer an option.
External motivators
One’s social network was perceived to be the most significant external motivator for engagement in physical activity. Many of the participants discussed the positive influence of their families on their movement today. Some spoke of a deep-seated value on physical activity and sports within their family culture. One participant explained the influence of her family’s support on her motivation as a college athlete, “they helped me get to this point, so I work hard for them,” (Mia). Those in the cohort who were surrounded by a physically active social network perceived themselves to be more active. Participants often spoke about their friends serving as movement accountability partners, providing a steady motivation to engage in physical activity with others. Others credit those in their social network for introducing them to the sport or activity they enjoy most. Many were motivated or felt obliged to keep up with active peers (Quote 2.7., Table 2). The participants also discussed gaining exercise-related knowledge and motivation not only from their social network, but from their built and natural environments as well. Among the cohort, those currently in college highlighted the positive impact of their institution’s recreational facilities. The young adults who had transitioned from college to career often voiced an appreciation for the factors within their surroundings that support physical activity participation, such as hiking trails and walkable cities.
Movement Mindset
Envisions for future physical activity
Collectively, participants viewed themselves as “active,” whether or not they were still involved in competitive sports. Some recognized that their physical activity levels had decreased following the cessation of sports participation, like Nelle, who reported, “[I’m] obviously, probably not at my prime, or I guess the level that I was at, but I’m still pretty active.” Others described a perceived maintenance of physical activity, despite having to transition away from organized sport, like Mikey who perceived himself to be “as active as a college student can be without playing an actual sport.” The desire to maintain a high level of physical activity was strong, yet some participants forecasted an inevitable decline in activity due to age or residual effects from the ACL injury (Quote 3.2., Table 3). Other participants perceived a future career, marriage, or family life to become a potential barrier to their physically active lifestyles. A few also expressed concern that another injury may derail their physical activity-related goals. Yet, all participants communicated an intent to continue pursuing a physically active lifestyle, as succinctly stated by Juan, “[I’m] 100% likely [to continue pursuing physical activity].”
Perceived impact of injury
The perceived overall impact of the adolescent ACL injury on current physical literacy and physical activity participation varied among the participants. Some classified the ACL injury as a non-issue when considering its impact on current physical activity participation. One participant reported, “honestly, [it] barely crosses my mind,” (Nelle). For these participants, terms such as “blip” and “hiccup” were used to describe the event. In contrast, Kate explained why she is still trying to find her footing in Quote 3.4., Table 3.
Most of the participants also perceived their adolescent ACLR experience to have a positive effect on their physical activity participation. While these participants acknowledged the initial hardship of the incident, they currently viewed the overall impact in a positive light. The cohort discussed positive post-injury effects, such as gains in knowledge and a stronger awareness of one’s body and abilities. One participant described the trajectory of his motivation to move since ACLR as, “I would say [the ACL injury was] something like a catalyst, I guess, for change,” (Joe). Others discussed improvements in overall resilience and character as a result of undergoing ACLR.
Belief in the power of sports
This theme also included the participants’ view of the larger impact of sports on their lives, shaped by an underlying belief in the power of sports. Taking a broad view of the impact of sports on one’s life, some participants referred to sport as a societal tool for good. Many of the participants recognized and valued the lasting benefits of sport participation on their lives today. In regards to current physical activity, Mikey reports, “I think if I didn’t play sports [in high school], I wouldn’t be nearly as motivated to stay active [today].” Some participants discussed the positive impact of sports on other aspects of life, including their careers. Olive described the potential impact of sports on her 3 year-old son in Quote 3.7., Table 3.
DISCUSSION
The purpose of this study was to understand the lived experiences and perceptions of factors that influence physical activity among young athletes following ACLR. Three overarching themes were identified, which included factors that spanned all levels of the Socioecological Model. All participants acknowledged the unique adaptations they make to overcome barriers to engaging in physical activity today. These adaptations, along with the participants’ internal and external movement motives, were perceived to facilitate engagement in physical activity. Underlying these perceived barriers and motives was a movement mindset that was derived from the injury experience itself, along with the participants’ lived experiences as young athletes. The findings demonstrate the usefulness of applying a systems-level approach for investigation of physical activity behavior among young athletes. The participant perspectives also reveal limitations within current clinical practice that may be thwarting the optimization of a physically active lifestyle following ACLR.
Physical Activity Perceptions and Behavior after Adolescent ACLR
Previous research has shown that young patients who return to sport after ACLR demonstrate less overall physical activity than their healthy peers.5,7 Accelerometry data has also revealed that this population spends significantly less time in moderate-to-vigorous physical activity per day.5,22,23 Prior to this work, a small number of studies have investigated physical activity behavior after ACLR, but even fewer have explored the meaning attributed to physical activity by patients after ACLR. Many of the participants in the current study described themselves as “very” or “quite” physically active as compared to peers. However, their views of an inevitable decline in activity are consistent with those voiced by young adults in a similar timeframe after intra-articular knee injury.24 Participants also admitted having to make adjustments in their physical activity as a result of previous knee injury, a behavior seen as early as one year following adolescent ACL injury.24,25 Furthermore, young athletes have described an increased awareness of their injured knee that sometimes negatively impacts physical activity participation,24 a perception consistent with those seen in the ‘unique adaptations’ subtheme of the current findings. This qualitative work also suggests that individuals who suffer an adolescent knee injury place a high value on physical activity for both knee-related health and long-term health. Yet, the findings indicate that this population continues to experience frequent barriers to physical activity participation.
Lasting Barriers and Long-Term Adaptations
Long-term health and quality of life is often not considered nor addressed within the current care paradigm after ACLR.26,27 The findings of this study would suggest that standard practice may not be meeting the long-term needs of these athletes, particularly in the physical domain. At 3-10 years post-ACLR, most participants spoke of persistent barriers they face in regards to physical activity engagement. Consistent with previous work,28,29 a continued fear of reinjury or lack of confidence was often perceived to negatively influence activity levels. Also highlighted were perceived effects of physical limitations on one’s physical activity. A high volume of ACLR-related research has concentrated on physical function after surgery, showing that deficits in strength,15,30,31 functional performance,15,32 and patient-reported function19,22,33 are common in the years following ACLR. Accordingly, participants identified factors such as tightness, giving-way episodes, and loss of strength as barriers within their movement experience. These findings not only demonstrate the perceived impact of physical limitations on one’s physical activity, but also suggest that young athletes may continue to encounter physical function barriers that extend beyond rehabilitation. A thorough examination of barriers faced in the years after adolescent ACLR, both physical activity-related and not, would be an important topic of future studies in order to inform development of interventions aimed at long-term quality of life.
Rethinking the Care Paradigm after ACLR
The participants’ perspectives in this study highlight the dynamic interactions between the individual and the various levels of their environment, which allows for a richer examination of the influence of adolescent ACLR on physical activity participation. While the participants spoke at length on elements within the intrapersonal domain (e.g. fear, enjoyment), they also described how these elements were influenced by factors within the environments in which they interact. As a common example, a perceived lack of time to be physically active was reinforced within the context of an inactive social network. Lack of social support frequently resulted in lower motivation to be physically active. Similarly, relationships between intrapersonal and interpersonal factors were perceived to be influenced by those within the organizational, community, and policy domains of the Socioecological Model.10,11 Participants reported factors such as a lack of competitive sport options (organizational), discomfort exercising in a local gym (community), and COVID-19 restrictions (policy) as significant influences on their motivation and social network. By utilizing a systems-level socioecological framework, this study adds novel and holistic insight to what is known about physical activity behavior and outcomes following adolescent ACLR.
Of special note, the participants unanimously named their social networks as the most important external motivator for movement. Following ACLR, participation in group exercise has shown to positively influence psychological factors and increase perceptions of physical function.34 Furthermore, in addition to exerting a positive influence on rehabilitation outcomes,29 a good connectedness with health professionals, coaches, teammates, and family has been shown to aid in the management of fear of reinjury following ACLR.35 The importance of addressing relatedness concerns in the years after adolescent ACLR cannot be understated, as these findings suggest that connectedness is a key factor in both short- and long-term physical activity engagement.
Strengths and Limitations
This cohort was recruited to represent adolescent athletes who undergo ACLR with the intent of returning to prior level of sport. As such, the scope of transferability of findings may be limited to a younger athletic population following primary ACLR. There were no participants who suffered a second ACL injury, an outcome that represents up to 30% of adolescents who undergo primary ACLR.36,37 The participants in this study acknowledged the known risk of second ACL injury as a factor that influenced current physical activity choices. Thus, it is possible that this cohort represents athletes who successfully adjusted their activity and expectations following ACLR in order to reduce risk of subsequent injury.
The authors believe the recruitment window of 3-10 years post-ACLR allowed sufficient time for reflection on physical activity following adolescent ACLR. However, it is likely that the participants’ current perspectives were influenced by factors, events, and experiences from the initial post-rehabilitation period, which was not a focus of the study. It is important to recognize that the attitudes and beliefs shared by the participants were likely driven by a cascade of factors that began early post-injury. The current findings suggest that these young athletes experienced shifts in activity levels, mindset, and social network during their adolescent and young adult years. Future work should explore the impact of these shifts and others on perceived physical activity 3+ years following adolescent ACLR.
CONCLUSION
This qualitative study provides unique insight into the factors perceived to influence physical activity 3-10 years after adolescent ACLR. Perspectives that gave rise to the three themes identified indicate that the adolescent ACLR experience has the potential to significantly influence one’s physical activity into young adulthood. It is critical that those who provide care for young athletes consider elements throughout the socioecological framework when designing clinical and educational interventions to enhance the long-term health and quality of life after adolescent ACLR.
Acknowledgements
The study team is especially grateful to the patients who participated in this project – it is an honor to elevate your voice and use your stories to positively impact future patient outcomes.