Background
A landing error scoring system (LESS) is often used to evaluate landing maneuvers.1,2 The LESS has 17 items to be evaluated, and points are added one at a time if any incorrect landing behavior is observed in the sagittal and frontal planes. It has a high reliability of 0.91 within examinees and 0.84 between examinees .3 Recently, a machine called the portable motion analysis system (Physimax) was developed that can immediately calculate LESS scores after capturing motion on video. In addition, Physimax has been reported to have excellent validity compared to three-dimensional motion analysis.1
The transversus abdominis and internal oblique muscles are functionally important during landing movements.4 Their activity is considered necessary to prepare the trunk for landing and to prevent it from tilting during the process.4 Although it has traditionally been difficult to evaluate the function of deep trunk muscles, recently, high validity has been reported by comparing the thickness of deep trunk muscles with electromyographic activity using ultrasound equipment.5–7 Additionally, the amount of thickness changes in these muscle groups between an “at rest” condition and during a contraction may give information regarding the activation of the muscles. Athletes with the lower percent of change in the thickness of the muscles of transversus abdominis and internal abdominal oblique when their performance is assessed with ultrasound equipment would be expected to have poorer LESS scores. The purpose of this study was to examine whether an association exists between landing movements and a high risk of lower-extremity injury and trunk muscle function.
Methods
Subjects
Thirty-nine athletes were included in the study. The inclusion criteria were 1) gymnasts for whom landing was an important element, and 2) the level of competition was the first division of the Kanto University Federation. Measurements were performed from January 2022 to March 2022. This period was selected because no major competitions were scheduled.
Exclusion criteria were a history of injury to the lower extremity or back in the prior three months or a history of surgery to the lower extremity or back or if the athlete was not participating in gymnastics competitions because of lower extremity pain.
This study was approved by the Ethics Committee of the affiliated Hospital (Approval No. 2021-006). The purpose, contents, and procedures of the study were fully explained to the participants and their consent was obtained.
Measurement method of trunk muscle thickness
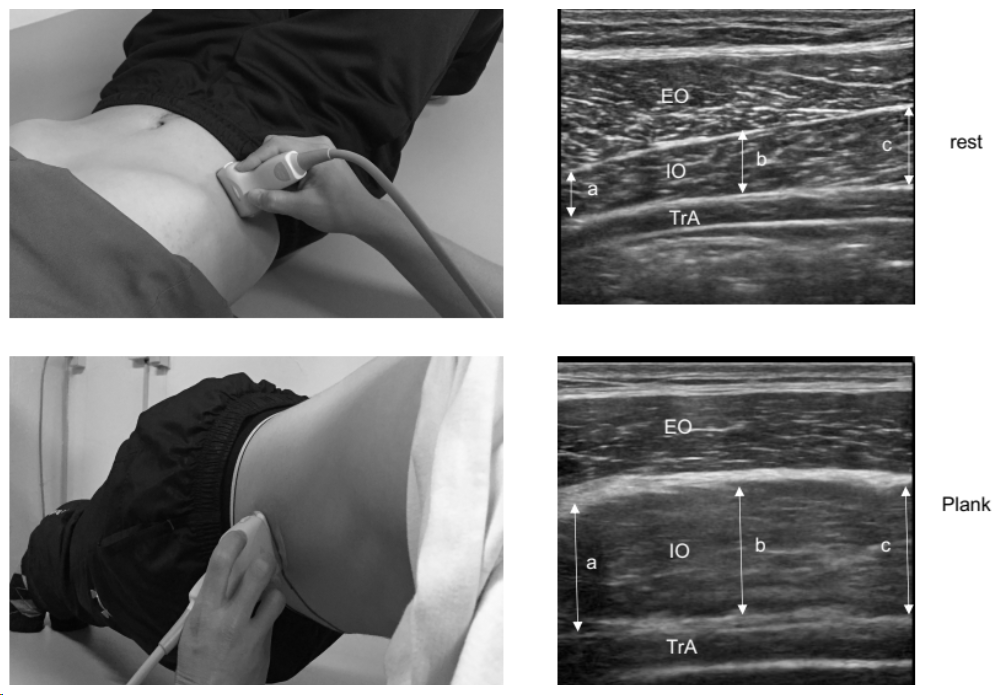
The transversus abdominis, internal oblique, and external oblique muscles were imaged at rest and during plank (hereafter, PL) using an ultrasound tomography device (HITACHI, Noblus, Japan). The resting position was supine with the hip and knee joints in mild flexion, and the posture during PL was such that the trunk and lower limbs were aligned with the body supported by the forearms and feet (Figure 1), which has been reported to activate the trunk muscles at a level equivalent to squatting.8 Additionally, because it is a static movement, ultrasonography provides stable imaging of trunk muscle thickness, which is why it was employed in this study.
Measurements for muscle thickness a linear probe (11 MHz) were conducted using a linear probe placed at the intersection of the navel and a perpendicular line from the axilla, and the thickness of each muscle was measured. A still image was captured at the end of the exhalation period under natural breathing conditions. Two still images were taken at rest and during the PL.
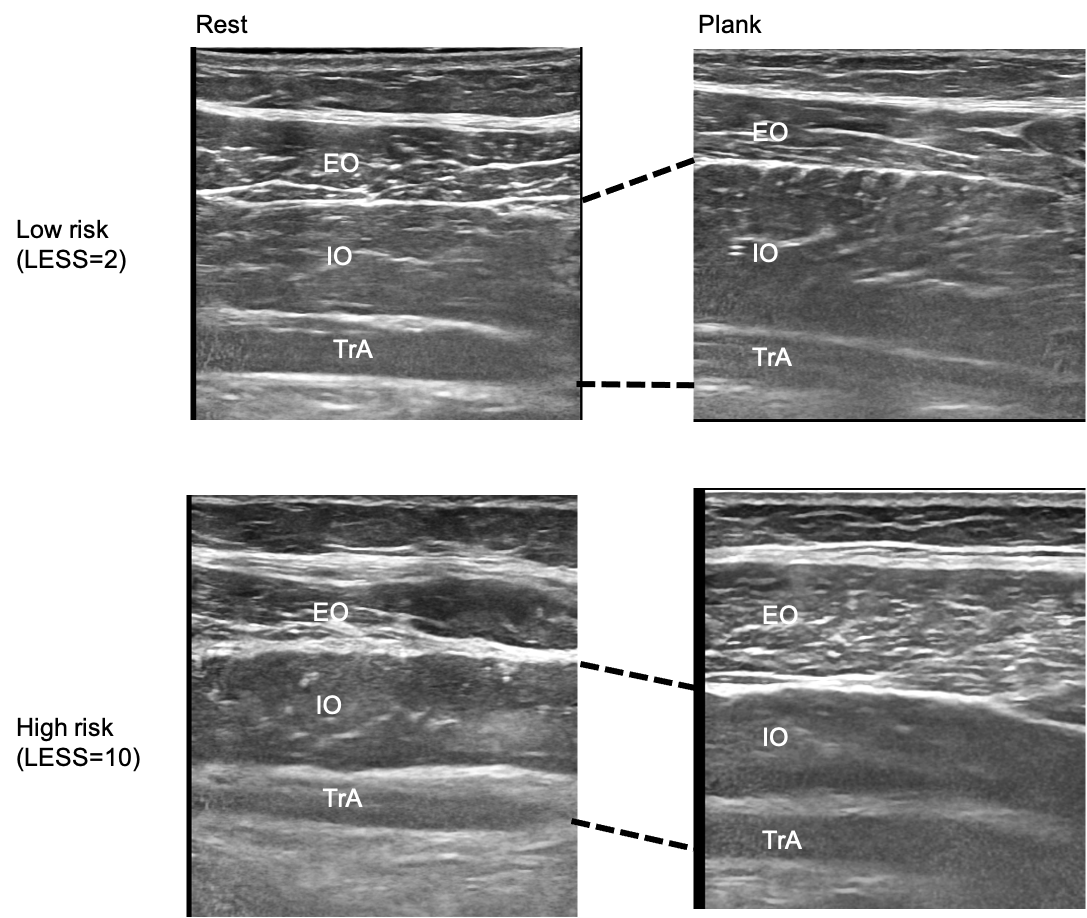
ImageJ software was used to measure the thickness of each muscle from the saved images. The transversus abdominis, internal oblique, and external oblique muscles were defined as the transversus abdominis muscle in the center of the image, and muscle thickness was measured between the upper and lower fascia in millimeters. In addition to the thickness of each muscle, the total thickness of the transversus abdominis and internal oblique muscles was calculated as an index of the deep trunk muscles in this study.9 The average of the two measurements, one at rest and the other during PL, was calculated. From the results, the percentage of change in muscle thickness (calculated as [muscle thickness at PL - muscle thickness at rest] / muscle thickness at rest * 100) was determined.

Landing motion measurement method
A motion analyzer (Physimax Technologies, Israel) equipped with a high-speed camera was used to evaluate the landing movements. The participants were instructed to land the drop jump from the platform to the target position and jump quickly until three successful attempts were made.
The specifics of a jump trial were defined as follows: (1) jumping from the box with both feet simultaneously; (2) jumping forward from the box; (3) landing on a mark on the floor 1 m away from the platform; and (4) jumping again smoothly without stopping. After each trial, there was a two-minute break, and trials continued until three jumps had been successfully completed. The participants performed jumps wearing shoes, a T-shirt, and shorts.1
The LESS scores were calculated by adding points for errors in the sagittal plane, frontal plane, and overall movement during landing. Evaluation in the sagittal plane observes whether the trunk, hip, and knee joints are flexed during landing. The evaluation of the frontal plane was based on whether the trunk was in lateral flexion and the knee joints were externally bent. There are 17 items to be evaluated, and a score of 6 or higher indicates a high risk of lower-limb injury.10,11
Statistical methods
Those who scored six or more points on the LESS were considered to be at high risk of injury (high-risk group), and those who scored less than six points were considered to be at low risk of injury (low-risk group). Muscle thickness at rest, muscle thickness during the plank, and the percent of change in trunk muscle thickness were compared between the groups. Comparisons between the two groups were performed using an unpaired t-test.
The relationship between LESS scores and trunk muscle thickness were examined using stepwise multiple regression analysis. The dependent variable was the number of LESS scores, and the independent variables were muscle thickness of the transversus abdominis, internal oblique, external oblique, and internal oblique + transversus abdominis muscles at rest; muscle thickness of the transversus abdominis, internal oblique, external oblique, and internal oblique + transversus abdominis muscles during the plank; and the percent of change in muscle thickness of the transversus abdominis, internal oblique, external oblique, internal oblique, and transversus abdominis muscles.
Statistical analysis software (SPSS Statistics 22, IBM, USA) was used for statistical analysis, and a p-value of less than 0.05 was considered statistically significant.
Results
Table 1 presents the characteristics of the study participants. They were 21 ± 1 years old, 172 ± 12 cm tall, and 65 ± 11 kg in weight. No significant differences were observed in male/female ratio, age, height, weight, or BMI between the two groups.
Table 2 presents a comparison of trunk function between the low- and high-risk groups. The results showed that the high-risk group had significantly lower muscle thicknesses of the transversus abdominis (mean difference=0.04, d=0.56) and transversus abdominis + internal oblique abdominal muscles (mean difference=0.10, d=0.55) during the plank. Additionally, the high-risk group showed significantly lower percent of change in muscle thickness of the internal oblique (mean difference=0.12, d=0.55) and transverse abdominis plus internal oblique (mean difference=12.49, d=0.70) muscles.
Subsequently, the relationship between the LESS scores and trunk muscles was examined using the stepwise method of multiple regression analysis, and only the percentage of change in muscle thickness of the internal oblique and transverse abdominal muscles was extracted as a factor (Table 3 and Figure 2).

Discussion
This study highlights the critical relationship between trunk-muscle function and the risk of injury during athletes’ landing maneuvers. Notably, a significant association was identified between a low function (as indicated by change in thickness during plank activity) of the transversus abdominis and internal oblique abdominal muscles and higher injury risk as determined by the LESS results (Figure 2). These findings underscore the importance of trunk stability in injury prevention and suggest that targeted interventions may be beneficial for strengthening or improving the function of these muscles. Furthermore, the use of ultrasound to evaluate trunk function represents a novel approach in this area of research, offering new insights into the biomechanics of landing motions.
Relationship between the high-risk group of LESS and the trunk muscles
Transversus abdominis and internal oblique muscles are connected to the thoracolumbar fascia and play a crucial role in trunk stability.12,13 Additionally, these muscles are reported to be the most active trunk muscles during landing motion.4 Athletes with poor trunk stability are at a higher risk of lower extremity injuries.14–16 When a trunk is unstable during landing and there is high impact, it can cause stress on the knee joint and lower leg, leading to lower-limb injuries.17 Notably, lateral flexion of the trunk is significantly associated with the external stresses on knee joints.18 Furthermore, trunk extension increases the extension torque on the knee joints.19
The current findings indicate that the group at high risk during landings shows less change in the thickness of the muscles of transversus abdominis and internal oblique during plank position than the low-risk group. The change in the percentage of muscle thickness has been previously correlated with electromyographic (EMG) activity.7,20 Therefore, athletes in the high-risk landing group likely exhibit lower trunk muscle activity than those in the low-risk group, although EMG was not directly considered in this study.
Clinical significance
In a study comparing the trunk activity and external knee joint stress, researchers compared the squatting motion when performed with hollowing, in which the abdominal muscles are drawn in, and bracing, in which the abdominal muscles are inflated. Bracing the abdomen has been reported to result in less trunk sway and lower knee external stress.21,22 Additionally, the trunk and knee eversion angles for drop jumps improve after trunk training.23 Therefore, promoting the activity of the internal abdominal oblique muscles in a bracing-type maneuver, may improve trunk stability and landing motion. However, this supposition was not studied in the current research.
Lateral flexion of the trunk and backward center of gravity during landing movements have been related to lower-extremity injuries.15,24,25 However, there has been no “qualitative” assessment of which trunk muscles are actually used, such as the number of seconds in the trunk-hold test16,17 or reactions during sway.26,27 In this study, the authors determined the responses of trunk muscles that are important for landing using an ultrasound assessment of change in thickness between rest and a plank. This paradigm may be useful for future research.
This study has several limitations. First, trunk muscle thickness was not measured during the actual landing movement. Second, only landing movements were screened; thus, the actual occurrence of injury could not be assessed. Future studies should evaluate which factors of the LESS are improved by trunk-exercise interventions and which scores show improvement. Additionally, a prospective study needs to be designed to determine the relationship between interventions and injury incidence. Third, the participants in this study were exclusively gymnasts, whose landing techniques are specific to their sport. The landing scenarios during the LESS were highly controlled. Therefore, to generalize the findings, athletes from sports, such as basketball, in which landing often involves uncontrolled contact, should be recruited, and a broader investigation should be conducted.
Conclusion
Athletes with more landing movement errors, determined based on LESS scores, showed lower change in muscle thickness in the trunk muscles. The transversus abdominis and internal oblique abdominis muscles have been shown to be important to trunk stability, and future intervestigattions using change in thickness measurements could be conducted to determine whether errors improve after interventions.
Corresponding author
Yuki Muramoto, PT, MS
Department of Physical Therapy Science, Tokyo Metropolitan University Graduate School of Human Health Sciences
7-2-10 Higashiohisa, Arakawa-ku, Tokyo 116-0012, Japan
e-mail: yukimuramoto1019@gmail.com
Conflict of interest
None declared.
Acknowledgements
The authors thank all the players who participated in the study, as well as the supervisors and coaches who provided help. The authors also thank Editage (https://www.editage.jp) for assistance in structuring this paper and English language editing.