






INTRODUCTION
The Achilles tendon (AT) is the largest, strongest, and most powerful spring in the human body, primarily functioning to provide a tendinous connection for the soleus and gastrocnemius to the calcaneus. It endures tremendous loads, particularly during eccentric calf contractions. Rupture of the AT is a traumatic injury requiring significant force and often results in lasting functional deficits, regardless of the treatment approach.1–3 Recent years have seen an increase in AT ruptures, particularly in explosive sports such as basketball, football, and gymnastics.4,5 While the rise in AT ruptures in professional football is well-documented,6,7 the increasing popularity of recreational paddle sports, such as pickleball, has also contributed to a rise in AT injuries.
Treatment for acute AT rupture is categorized into surgical and non-surgical management. Surgical repair is generally preferred for elite athletes due to superior outcomes in reducing rerupture rates and restoring plantar flexor strength.8–12 Surgery was advocated to reduce the risk of rerupture compared to non-operative treatment with cast immobilization, however when implementing early mobilization and WB for both nonsurgical and surgical patients, it was postulated that rerupture risk was equal between the groups.12 In contrast, a recent multicenter, randomized controlled trial comparing complication rates between non-operative treatment, minimally invasive surgery, and open surgery showed the non-operative group had a 10x increase in rerupture.13 Participants in this study were cast immobilized for 2 weeks from time of injury or surgery, and then allowed full WB in an orthosis with heel lifts for 6 weeks while following a standard ATR rehabilitation protocol.13 Thus while the impact of surgical vs non-surgical management on rerupture risk needs further investigation, early functional rehabilitation including weightbearing and mobilization is recommended regardless of treatment pathway. Minimally invasive techniques (PARS) have been developed to minimize surgical wound complications compared to open surgery, but studies have shown similar wound complication rates between the techniques,13,14 while open techniques are stronger and require shorter immobilization periods.14 Recently the SpeedBridge™ (Arthrex Inc, Naples, FL) has been touted as combining the advantages of open surgery with minimally invasive techniques by using suture anchors to secure the AT to the calcaneus. Clinical results with this technique have not yet been published and concern regarding persistent calcaneus pain from the suture anchors remains. Thus, open techniques remain the gold standard at this time as the strength of repair allows earlier mobilization and WB, while maintaining complication rates similar to minimally invasive techniques.
Post-operative rehabilitation guidelines vary significantly, especially regarding WB progression and immobilization duration.15 Historically, conservative WB progressions were followed aiming to minimize tendon elongation, which was associated with poor outcomes. However, recent advancements favor early progressive loading, as evidence suggests tendon elongation is unaffected by accelerated WB and early mobilization compared to delayed WB.15–18
This commentary outlines advancements in rehabilitation for athletes undergoing ATR. We highlight key principles, including early WB and mobilization, use of BFRT, progressive loading, and monitoring athletic qualities as part of the RTS continuum. We will review evidence and include clinical expertise where appropriate.
OVERVIEW
Anatomy and Basic Science
The AT’s thick and robust structure play crucial roles in strain transfer during physical activities. The AT can withstand enormous loads approaching 11x bodyweight (BW) during sporting activities such as high-speed running19,20 and 15x BW in gymnastics landings.4 A thorough understanding of the involved anatomy and biomechanics is required to guide post-operative rehabilitation.
Key anatomical factors include but are not limited to:
-
Thickness and Robustness: Structure of the tendon is essential for handling high loads and strain transfer. A larger cross-sectional area (CSA) after rupture improves the tendon’s load-bearing capacity. Zellers et al. found that CSA at 12 weeks post-operation was the strongest predictor of heel-rise test limb symmetry index (LSI) at 52 weeks, correlating with superior functional recovery.20
-
Twisting Structure: Twisting structure of the AT is integral to its anatomy. The AT twists approximately 90 degrees laterally from the middle of the calf to its insertion on the posterior calcaneus. This twisting affects strain transfer and muscle contribution based on lower leg orientation (e.g., inversion vs. eversion).21
-
Viscoelastic properties: Viscosity and elasticity both contribute to the AT’s role in force absorption and transmission. Tendon elasticity is important for energy storage and release during stretch-shortening cycle (SSC) activities, while viscosity is important in force absorption. Tendon healing and maturation to allow restoration of these properties is critical in restoring tendon function.
Incidence/Prevalence
AT ruptures account for 10.7% of all tendon and ligament injuries, with an annual incidence of 8 cases per 100,000 people, predominantly affecting males (79.2%) and occurring mostly during sports (65.2%).22 Acute AT ruptures usually result from high-load impacts, such as rapid ankle dorsiflexion with the hip and knee extended. Up to 90% of sports-related AT ruptures are caused by acceleration-deceleration mechanisms.23 The incidence of AT ruptures has notably increased in competitive athletes, with a 3-5x increase in the NFL over the past 25 years, including 24 cases in the 2023-2024 season.6 Chan et al. reported a significantly higher AT injury rate in women’s gymnastics (16.73/100,000 athlete exposures) compared to other sports.24 Reports of up to 46% of individuals with an AT rupture had a history of AT pain or tendinopathy,22 complicating patient management.
Treatment Strategies
AT ruptures can be managed surgically or conservatively. Conservative management may be preferred in recreational athletes, but rates of surgical vs nonsurgical management vary depending on cohort.22 In competitive athletes, surgical repair is preferred due to superior outcomes in plantar flexor strength and reduced rerupture rates.10,12,25 Regardless of treatment option, there is evidence suggesting early functional rehabilitation and WB result in comparable functional outcomes and patient satisfaction.25,26 Minimizing tendon gapping and tendon elongation are critical determinants of successful outcomes. It is well established that tendon lengthening occurs after AT rupture, regardless of surgical or conservative management.27,28 Maquirriain et al. identified two main factors related to tendon lengthening: inadequate surgical construct tension and progressive elongation during rehabilitation.27 During surgery, tension of the opposite leg is gauged with the goal of increasing resting tension of the ATR relative to the uninvolved side, allotting for some elongation of the construct post-operatively.29,30 Avoiding dorsiflexion past neutral until 8 weeks post-surgery is advised, as the greatest tendon elongation occurs between 2-6 weeks post-surgery regardless of WB protocol,18 significantly impacting postoperative outcomes.16,28
Surgical Techniques
-
Open Repair: strongest biomechanically, longer surgical time, wound complication rate similar to minimally invasive, often recommended in high demand athletes to allow robust repair.31
-
Percutaneous Repair: minimally invasive, cosmetic benefits, higher risk of tendon elongation compared to open repair, suggested higher risk of sural nerve injury.31,32
-
SpeedBridge System™: tendon anchored to bone via anchors and hour-glass suture construct, providing less displacement and higher ultimate load to failure than other techniques in vitro. Clinical results are lacking, and calcaneal pain may persist due to suture anchors.
POST-OPERATIVE REHABILITATION
Rehabilitation plays a pivotal role in optimizing outcomes post-ATR. Specifics regarding WB and range of motion (ROM) progressions are decided by the surgeon based on surgical technique, tissue quality, type of fixation and personal preference. Communication with the treating surgeon and understanding the specifics of the surgical procedure and healing time frames will ultimately guide the rehabilitation progression. This commentary will highlight key components of an accelerated rehabilitation approach for an athlete following acute ATR. An accelerated rehabilitation approach should always be discussed with and approved by the surgeon [Table 1]. Key rehabilitation principles include early loading and mobilization, restoring tendon mechanical properties, progressive strengthening, restoring elastic qualities and navigation through the RTS continuum. The authors recommend a criterion-based progression that considers individual and contextual factors, as well as the biology of healing.
Key Rehabilitation Principles
-
Respect time frames of tendon healing11,12,25
-
Phase 1: Acute Inflammatory Phase (up to 1-2 weeks): Inflammatory cells remove injured tissue.
-
Phase 2: Proliferative Phase (up to 4 weeks): Fibroblasts produce Type I collagen, increasing tendon strength.
-
Phase 3: Remodeling Phase (up to >18 months): Maturation of tendon structure, improving tensile strength and elasticity.
-
-
Early Mobilization: Mechanical loading promotes tendon healing and maturation.33–36 Studies suggest early mobilization post-ATR improves tendon healing and decreases rerupture rate when compared to delayed mobilization.11,17,33
-
Restore mechanical properties of the tendon: Mechanical properties of the tendon including stress, strain and shear modulus are critical in maintaining the functional integrity of the Achilles complex.37,38 Mechanical tension and mobilization support collagen fibril alignment and tendon thickness.39 Low-load BFRT (LL-BFRT) has been shown to increase AT mechanical and morphological properties similarly to conventional high-load resistance training and can be utilized during early phases of post-operative rehabilitation.40,41
-
Progressive Strengthening: It is well established that calf musculature undergoes significant atrophy after ATR.42–45 Progressive resisted exercises targeting local and global muscle strength deficits should be implemented and follow a functional progression. Targeting the ankle plantar flexors in varying degrees of ankle dorsiflexion can alter relative muscle contributions (i.e gastrocnemius vs soleus) to target specific deficits.46,47 Exercise variables including magnitude, duration, and rate of loading should be considered to design exercises and progressions based on the clinical need.48
-
Restore Elastic Actions: Elasticity of the AT is essential for the tendon’s role in SSC activities.
-
Return to Sport Continuum: Consider RTS as a continuum, rather than a moment in time. Quantify and monitor key criteria or key performance indicators (KPI’s) with serial testing along the continuum to guide RTS decision making.49
Immediate Post-Operative Phase (0-2 weeks)
Goals: Manage pain, control swelling, protect surgical site.
The initial phase of recovery post-ATR is characterized by maximal protection of the healing repair. Protection of the repair site allows the initial phases of tendon and wound healing and minimizes the risk of complications. Any signs of infection or deep vein thrombosis (DVT) should be brought to the surgeon’s attention immediately. Traditionally the patient is non-weight bearing (NWB) with a short leg cast or CAM boot to promote wound healing and protect the repair. Length of immobilization varies among surgeons and surgical techniques. Accelerated WB protocols are variable, but may allow immediate partial WB (PWB) in a CAM boot with heel lifts.11 The use of a heel lift can reduce plantar flexor activity by 57% during normal gait, thus decreasing strain on the surgical repair.50 During the immediate post-operative phase, proximal and core strengthening can be initiated as part of in-person rehabilitation or a home exercise program. With clearance from the treating surgeon, BFRT may be initiated at this time on the ipsilateral or contralateral limb. Exercise selection can vary based on post-operative restrictions, however proximal exercises for the hip and knee musculature are typically safe to initiate immediately after surgery. Submaximal volitional plantar flexion isometrics may be initiated in the boot or cast to facilitate venous return and stimulate calf activity in a protected, shortened position within the immobilizer. Care should be taken to minimize sweating around the wound which may increase the risk for infection. Elevation and cryotherapy can be used to manage post-operative pain and swelling.
Controlled Mobilization Phase (2-6 weeks)
Goals: Progression to full WB (FWB) in boot, improve gastrocsoleus activation, minimize pain and swelling, initiate cardiovascular training when incision is well healed.
The primary goal during this phase is to accommodate ambulating in the boot and provide controlled tension to the repair while avoiding tendon elongation. Accelerated WB protocols will typically progress from PWB to FWB in the CAM boot by 4-6 weeks. Patient education regarding load progression and managing walking volumes should be stressed at this time. The patient may ambulate with a shorter stride length to avoid adverse stress on the repair. While AT length is difficult to measure directly, passive tension as a proxy measure can be evaluated with the patient prone, knee bent to 90 degrees and hip in a neutral position [Figure 1]. The resting position of the ankle is measured and monitored.27,30

Sudden increases in relative dorsiflexion ROM should be communicated to the surgeon and considered when reducing heel lift height or increasing WB. Once progressed to FWB in the CAM boot, with surgeon’s clearance the patient may begin gait training in an athletic shoe with heel lifts.
Ankle active range of motion (AROM) exercises can be initiated at this time. Ankle dorsiflexion is typically limited to neutral with the knee flexed for 4-6 weeks post-operatively to avoid elongation stress on the repair. Early initiation of AROM can facilitate proper collagen fibril formation,39,51 and early mobilization has been shown to reduce AT elongation and improve clinical outcomes.17,52,53 While early protected mobilization seems to be beneficial, it is generally recommended that passive stretching of the calf complex be avoided for up to 12 weeks post-surgery to protect the repair from elongation. It is expected and often preferred that patients have a sensation of tightness throughout the early phases of rehab, potentially indicating that tendon elongation is occurring at an appropriate rate. It is rare for a patient to complain of their Achilles being “too tight” at long-term follow up. Immobilization in a boot will restrict rearfoot, midfoot and hallux motion, allowing potential joint mobility dysfunctions. Assessment and treatment of joint mobility dysfunctions should be initiated within a protected ROM to improve joint mobility without passively stretching the Achilles complex. When the incisions are well healed, soft tissue mobilization can reduce tone of the surrounding musculature.
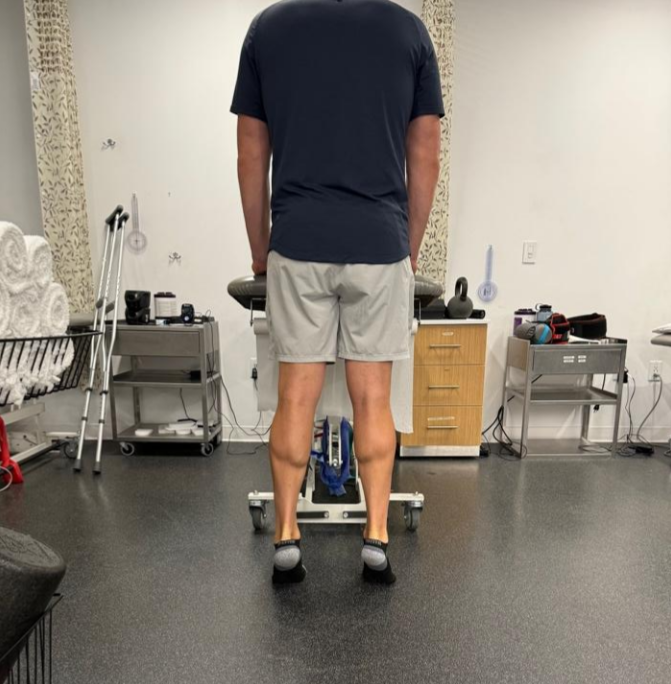
Plantar flexion isometrics can be continued with submaximal, non-painful efforts at end range plantar flexion ROM. This position puts the gastrocsoleus complex in a shortened position and minimizes elongation stress on the repair while promoting stiffness in the tendon. Neuromuscular electrical stimulation (NMES) can be used to improve muscle activation with isometric gastrocnemius contractions during the early phases of rehabilitation. Biofeedback using fixed dynamometers or force plates can be used to provide an external focus and quantify contraction intensity to gradually increase exercise demands [Figure 2].

While the use of BFR has limited research regarding its use in post-operative ATR rehab, there is evidence to support its use as a mainstay in lower extremity post-operative rehabilitation. In a randomized controlled trial of patients who underwent ATR, Hansen et al demonstrated greater isokinetic strength in the operative calf muscle at 3 months post-operative when using BFRT compared to the control group consisting of standard of care rehab.54 The use of LL-BFRT with Achilles tendinopathy has been shown to apply similar mechanical adaptations to heavy loading.40,41,55 It is the authors’ experience that BFR can help reduce atrophy and preserve lower extremity strength after surgery. As stated previously, BFR may be initiated in the first 2 weeks with exercises such as straight leg raises, side lying hip abduction and long arc quads to maintain lower extremity strength and hypertrophy while protecting the ATR. Plantar flexion isometrics can be progressed to limited range isotonic progressive resisted exercises (PRE) with BFR as ROM and tolerance to contraction improve. We recommend an emphasis on the use of BFR during the first 12 weeks of rehab to target plantar flexor and proximal lower extremity strength. In mid-late phase rehab (i.e > 12 weeks), a greater emphasis is put on mechanical loading and progressive resistance without BFR, using moderate to higher loads. In later phases of rehab, the authors continue to use BFR as an adjunctive treatment for “deload” days or additional session volume targeting muscle hypertrophy. Anecdotally the use of BFR for ischemic preconditioning may be beneficial to enhance muscle recruitment and recovery. While the authors have observed a significant benefit in this patient population, further research is warranted regarding ideal use of BFR following ATR.
Early Rehabilitation Phase (6-12 weeks)
Goals: Normalize gait, restore ankle plantar flexor strength, gradually restore closed chain ankle dorsiflexion ROM.
The primary goals of this phase are to return to “normal” walking with gradual restoration of plantar flexor strength and foot and ankle joint mobility. Once the patient progresses to FWB in a boot, they may be cleared to transition to an athletic shoe and begin to reduce heel wedge height. The AT undergoes peak loads approaching 2-4x BW during the gait cycle.19 To meet strength and mobility demands, an assistive device is reintroduced to ensure proper gait mechanics as the AT is exposed to increased loading without the walking boot’s protection. Gradual reduction of heel wedge height will help normalize gait mechanics while restoring tension on the repair. Monitoring symptoms and resting tension of the AT can help guide decision making when reducing heel lift height to control tendon elongation. Common gait deviations include a prolonged stance phase and avoidance of push-off in terminal stance, which can be addressed with targeted drills and cueing. Continuing to avoid passive stretching of the gastrocsoleus complex is necessary until 12 weeks. The transition to a shoe may create sensations of limited ROM, but as previously mentioned, a tight feeling is normal and should not prompt aggressive ROM work.
Aquatic therapy and unweighted treadmills are helpful in restoring proper gait mechanics by gradually increasing WB demands as the patient weans from their assistive device. It is important that the WB progression aligns with ideal gait mechanics. Poor mechanics lead to joint dysfunction, adverse muscle tone or inhibited strength, especially with fatigue. In a single subject case report by Zellers et al., upon transition from a CAM boot to athletic shoes, their patient demonstrated a decline in tendon mechanical properties including shear modulus and tendon viscosity as examined on continuous shear wave elastography (cSWE).38 The authors suggested that this may explain why some patients are prone to rerupture upon transitioning from the boot and that the tendon will require increasing load for further remodeling and restoration of mechanical properties. Extra care is taken to avoid progressing to lengthened positions too quickly to prevent elongation stress on the repair. The patient should be educated to avoid movements that put excessive eccentric stress on the ankle (i.e. stair negotiation) without an appropriate strength base. Therefore, it may be necessary for the patient to remain in their CAM boot outside of physical therapy as their gait mechanics, strength, and load tolerance improve.
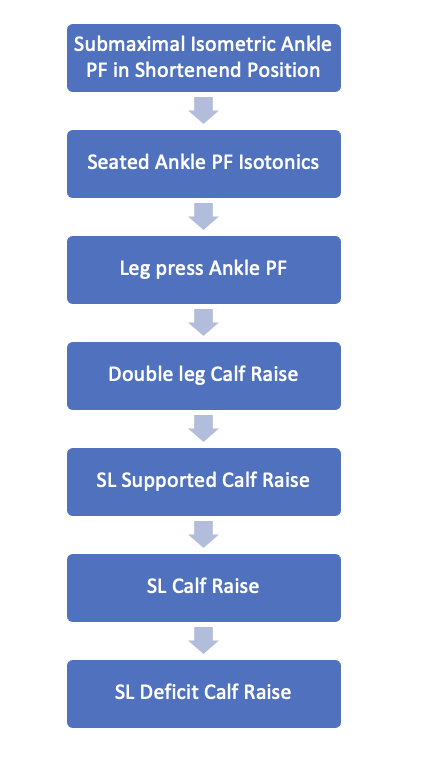
Progressive strengthening of the ankle plantar flexors should occur during this phase. The AT sustains enormous loads during athletic activities such as running, jumping and hopping.19,20 Progressive loading can help develop the necessary local muscle strength to tolerate these high stresses. Plantar flexor loading progressions can be initiated with the knee flexed to avoid progressing both variables of resistance and muscle/tendon length too quickly [Figure 3].
.png)

A sample plantar flexion strength progression is demonstrated in [Figure 4], using the concepts of progressive loading and muscle/tendon length to avoid over-stressing the repair. Milestones to achieve a full ROM heel raise may occur 8 weeks or later for double leg, and 12 or more weeks for single leg. While this is a good strength target, it has been reported that only 50% of patients were able to complete a single leg heel raise at 12 weeks post-injury.56


Quality of motion should be assessed during calf exercises, teaching proper heel raise technique by pushing through the 1st metatarsophalangeal (MTP) joint and avoiding compensation through great toe flexion. Intralimb compensations are often demonstrated after ATR and can persist long after surgery if they are not addressed.43,45,57 Appropriate exercise selection and reduction of weight demands can improve movement quality without common compensations. The authors have found gravity-assisted devices (e.g. AlterGⓇ) and aquatic therapy to be valuable when developing single leg strength and the ability to perform a single leg heel raise without compensation. Submerging in water to umbilicus height has been shown to reduce BW by approximately 50%. Aquatic therapy can be utilized to reinforce movement quality with various movements and also provides additional benefits such as cardiovascular training and swelling reduction via hydrostatic pressure.58
Fundamental movement patterns such as squats, step-ups and lunges can be progressed within available ROM. Baxter et al reported on the peak Achilles stress during various functional movements and traditional exercises.48 While this study was done on healthy individuals, it serves as a model for incremental stress on the Achilles based on exercise selection. Movement quality during exercises and soreness rules can help guide strength progressions for local and global muscle strength during this phase. Cardiovascular fitness can be further developed at this time with stationary cycling. Progression to an elliptical and stair climber may be initiated when the patient can ascend an 8" step with good concentric control and sufficient closed-chain ankle dorsiflexion ROM.
Late Rehabilitation Phase (12-24 weeks)
Goals: Gradual and progressive loading, strength measures > 70-80% limb symmetry index (LSI), initiate plyometric progression/return to running.
Mid-late stage rehab is characterized by restoring full sport-specific ROM along with fundamental local and global strength and neuromuscular control in preparation for impact activities. Gradual restoration of controlled closed kinetic chain dorsiflexion is of the utmost importance due to its crucial role in sport-specific movements such as deceleration. The authors advise implementing progressive resistance exercises to build functional strength and athleticism, while constantly evaluating movement quality to detect potential deficiencies and failed load transfer. Principles of kinetic linking can be used to integrate local muscle strength into full body movements along the kinetic chain.49,59
A key milestone during this phase is returning to plyometric activities including running and jumping, which are heavily reliant on the stretch-shortening capabilities of the AT complex. It is recommended that the rehab specialist ensure sufficient strength of the plantar flexors prior to initiating plyometric movements. This can be accomplished by assessing quantity and quality of double and single leg heel raises and technical capabilites with pre-running drills, as well as objective isometric and isokinetic assessments of force output if available. Low amplitude impact activities such as ladder drills and band-assisted pogo hops can be initiated to introduce SSC activities [Figure 5]


As strength and plyometric ability improve, progression may occur from intensive to extensive plyometric variations including box jumps and eventually drop vertical jumps. We recommend the rehabilitation professional does not rush this process, ensuring development of sufficient workloads of intensive plyometrics prior to progressing to higher demand movements.
Timelines to initiate running are highly variable after ATR. It is our preference for field and court sport athletes to demonstrate 1.5-2.0x BW isometric seated PF strength, 10 single leg heel raises through full available ROM, and good control and mechanics through single leg squatting movements prior to initiation of a running progression. Initiation of running is typically started no sooner than 12-16 weeks after surgery. Use of an AlterGⓇ treadmill or pool can allow for earlier introduction of impact activities at reduced BW. Additionally, the use of pre-running drills can be used to introduce concepts of foot-ankle complex stiffness and short contact times in preparation for level ground running [Figure 6].
Throughout the rehabilitative process, and especially while preparing the athlete for the RTS phase, it is important to consider the contralateral limb. Due to a significant reduction in activity and chronic load deficit throughout ATR rehabilitation, the contralateral limb may be exposed to higher risk of re-injury upon RTS. While relatively small, a higher incidence of contralateral AT rupture following ATR has been reported compared to that of initial AT rupture in the general population.60,61 After initial AT rupture, 1.3 to 5.5% of adult patients have been reported to experience subsequent contralateral AT rupture.60,61 Occupations involving physical activity were identified as a significant risk factor for contralateral AT rupture.61 Our preference is to implement similar strength and functional training techniques to the contralateral limb as the athlete recovers from ATR. Monitoring metrics of the contralateral limb such as peak torque to BW, reactive strength, and other data points described below is also advised as the athlete prepares for the RTS phase.
Return to Sport Phase (24+ weeks)
Goals: progress training volume, satisfy strength and power requirements (>90% of KPI’s), monitor loading throughout RTS clearance continuum.
Successful RTS after ATR is highly variable (61-100% RTS in elite athletes) and largely dependent on level of activity and demands of each sport.5 High demand jumping and explosive sports are often associated with lower RTS rates and performance deficits upon RTS.5 In a review of RTS rates and performance, NBA players showed deficits in performance metrics such as minutes per game and player efficiency rating in the first 2 years after injury.5 ATR typically yields positive long-term outcomes, but various studies have highlighted specific residual effects. Cretnik in 2019 reported a low re-rupture rate of 1%, with 80.89% of patients returning to their previous level of activity, however 16.48% experienced decreased ROM.60 Plantar flexion strength deficits are common and often range between 10-30% LSI after 1 year post-operative, with large inter-individual variation.43,44,62,63 Disproportionate weakness in end-range plantar flexion has been identified and may be related to anatomic factors such as tendon elongation and changes in tendon compliance.64 Deficits in heel-rise endurance of 20-30% persist for greater than 12 months post ATR.65,66 These studies collectively indicate that while many patients regain significant function, some experience long-term deficits in strength, elasticity, and ROM.
There is poor understanding of the ideal battery of RTS testing after ATR in athletes. Over the last couple decades, significant advancement in RTS testing protocols has been made regarding ACL injury.49,67,68 In the absence of evidence, clinicians can use clinical reasoning and extrapolate testing considerations from other long term rehabilitation to design RTS testing batteries.
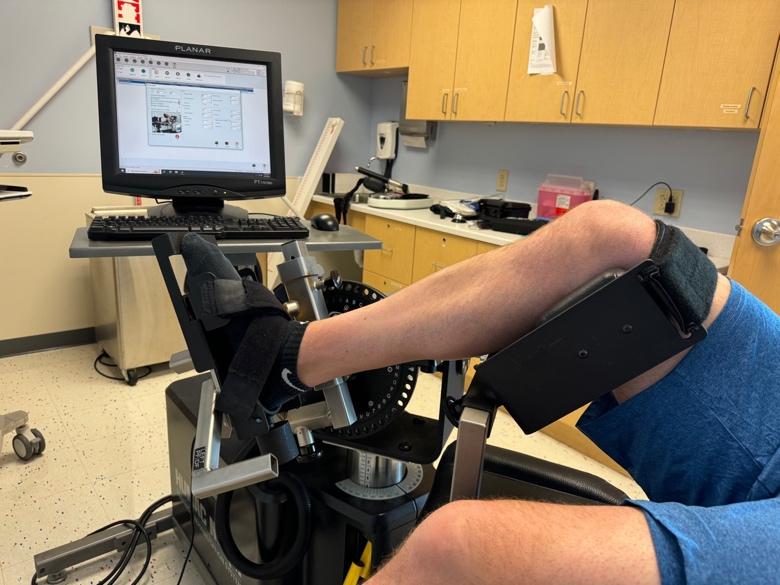
Draovitch et al. described RTS clearance as a systematic approach to testing, focusing on identifying key neuromuscular capabilities and systematically testing them along the rehab continuum to help guide RTS decision making.49 The gold standard to assess ankle strength requires an isokinetic dynamometer [Figure 7]. Historically, isokinetic strength assessments of plantar flexion and dorsiflexion have been used post-ATR. While isometric strength may be assessed with force plates and dynamometers earlier in the rehabilitation process, the authors typically wait until 4 months post-operative to begin isokinetic strength testing. When using isokinetic testing, a target of > 90% LSI and peak isometric strength of 1.5-2.0x BW is recommended, although reference values can vary based on testing methodolgies and cohort demographics. Strength assessment of the ankle plantar flexors in the seated position has been described using force plates or various dynamometers.69 In the absence of preinjury data, LSI can be used to evaluate plantar flexion strength in comparison to the contralateral limb. Population specific normative data is limited, but is available for specific cohorts.69,70 Allometric scaling can be used to evaluate strength in relation to an individual’s body weight. In elite athletes a target seated ankle plantar flexion force output of 1.5-2.0x BW or greater has been suggested as a benchmark for isometric strength in healthy individuals.70 Muscular endurance and muscle-tendon unit function can be assessed with the heel rise work test as described by Silbernagel et al [Figure 8].26,65,66,71 Single leg heel rise performance LSI (involved/uninvolved x 100) can be calculated based on number of repetitions as well as total work (repetition x height of heel raise).


Jump testing with or without dual force plate technologies has been used to assess lower extremity neuromuscular qualities, performance, and interlimb asymmetries in athletes. The countermovement jump is an assessment of slow SSC ability. Drop vertical jumps and repeated jump testing can be used to assess reactive strength. The reactive strength index (RSI) is an assessment of fast SSC plyometric ability (< 250 ms) and a KPI for explosive sports. RSI is typically calculated as a ratio of jump height divided by ground contact time. An RSI of >1.3 for double leg drop vertical jumps (DLDVJ) and >0.5 for single leg drop vertical jumps (SLDVJ) has been suggested in the ACL literature for field sport athletes.68 The single leg hop for distance (SLHD) can be used to assess horizontal power and dynamic lower extremity function. Kotsifaki et al., demonstrated that during a horizontal hop for distance, nearly 43% of the energy contributing to the propulsive phase of jumping is generated from the ankle. Distance metrics as well as 3D biomechanics to observe movement quality can be an informative component of a RTS testing battery.72 The table below summarizes sample jump testing that can be used to assess various neuromuscular qualities [Table 2]. We recommend utilizing jump testing to assess both double leg and single leg plyometric abilities. Upon demonstration of proper mechanics and loading patterns during pre-planned sport-specific movements, recent advancements in end-stage RTS training including neurocognitive and reactive training should be implemented.64 Sport-specific field-based testing should be performed and compared to pre-injury or position-specific normative values.
Reconditioning Phase
The progression of sport-specific loads and conditioning may be the most poorly understood phase of rehabilitation. As the athlete transitions back into on-field/on-court activities, the focus is on building in components of skill development, force and load accumulation, and sport-specific workload capacities to prepare for full activity.49 As defined by Buckthorpe et al., the 4 pillars of quality on-field rehabilitation include (1) restoring movement quality, (2) physical conditioning, (3) restoring sport-specific skills, and (4) progressive development of chronic training load.73 Communication between all stakeholders is critical to avoid load spikes during critical transition phases of rehab, which may increase risk of injury. It is our experience that clinicians often underload during the late phases of rehabilitation, leading to a relative overload during the transition phases of performance training. Effective communication between all stakeholders can help ensure smooth transitions through phases of rehabilitation and help guide successful return to performance.
CONCLUSION
AT ruptures, particularly prevalent in explosive sports, have prompted advancements in both surgical techniques and post-operative rehabilitation protocols. These innovations aim to enhance functional recovery, minimize rerupture rates, and facilitate a timely return to sport.
Key principles in rehabilitation emphasize the importance of respecting tendon healing phases, implementing early functional rehabilitation and mobilization, and progressive strengthening of the tendon and surrounding musculature. Care should be taken to control tendon elongation which is a critical determinant of long-term functional outcomes. Techniques like BFRT and NMES are gaining traction for their potential benefits in muscle preservation and strength restoration post-operatively.
In conclusion, advancements in surgical and rehabilitation techniques for AT ruptures have significantly improved outcomes for high-level athletes. Adopting evidence-based practices and individualized care plans is crucial for optimizing functional recovery and ensuring a successful return to sport.