BACKGROUND AND PURPOSE
The posterior cruciate ligament (PCL) is one of the main knee stabilizers, primarily resisting posterior translation of the tibia relative to the femur. Additionally, the PCL acts as a stabilizer and prevents excessive tibiofemoral rotation, particularly between 60° and 120° of flexion.1,2 Composed of two bundles (anterolateral and posteromedial), the PCL plays a crucial stability role in knee flexion and extension, especially in movements that require a lot of stability, such as jumping and pivoting. While traditional literature demonstrates that these two bundles function independently, recent research suggests that they act synergistically.2,3
PCL injuries are often severe and have devastating long-term effects, such as degenerative changes in the medial and patellofemoral compartments and impaired lower extremity function. Isolated PCL injuries are rare, with 60–95% of cases involving capsuloligamentous injuries.4–8 Common mechanisms of PCL injury involve external trauma resulting from a posteriorly directed force on the anterior region of the proximal tibia with the knee flexed, often referred to as a “dashboard injury” resulting from motor vehicle accidents. In sports, isolated PCL injuries may result from a direct blow to the anterior tibia or a fall onto the knee with the foot in a plantar-flexed position. Noncontact mechanisms, such as hyperflexion or hyperextension, are less common.8–11
Diagnosis of a PCL injury relies on clinical history, physical examination, and imaging tests. After inspection, palpation, range of motion (ROM) assessment, neurovascular examinations, and provocative tests are used to evaluate the PCL integrity or any concomitant injuries. The combination of clinical tests, injury mechanisms, and symptoms such as pain, swelling, and joint instability is crucial for establishing a PCL injury diagnosis.8,11
Several treatment options have been described in the literature, enabling an individualized approach based on lesion patterns (acute or chronic), treatment adherence, and patient demands. The ideal treatment for PCL injuries to restore joint stability, promote joint functionality, and return to activities remains unclear in the scientific literature. Conservative treatment, typically recommended for acute and isolated PCL injuries (Grades I and II), involves using a brace for immobilization, controlling weight-bearing and swelling, restoring ROM, and recovering muscle strength.8,12–14
Surgical intervention is considered for symptomatic patients with complete injuries (Grade III) who do not obtain satisfactory results in conservative treatment, those with a high degree of joint instability, or those with associated intra-articular and capsuloligamentous injuries.13–15 Post-surgical complications may occur in up to 53% of patients and can include intra-articular hematoma, infection, reflex sympathetic dystrophy, anterior knee pain, neurovascular injuries, and graft failure, potentially resulting in pain and instability.15–17
Low risk of bias studies that investigate the effects of different treatments of PCL injuries are limited. However, whether post-surgery or as part of a conservative protocol, the approach focuses specifically on increasing the quadriceps muscle strength and restoring joint stability. Exercises based on quadriceps strengthening are the focus of treatment to maintain dynamic stabilization of the knee, avoiding tibial posteriorization.13,18
Currently, the isokinetic dynamometer is considered the gold standard resource for assessing muscle performance and could be considered for treating lower-extremity injuries, especially knee injuries.19,20 The isokinetic dynamometer allows the evaluation of parameters, such as muscle power, total work, and peak torque normalized by body mass (PT/BM). Isokinetic exercises are characterized by using a constant velocity that accommodates muscle work throughout the ROM.21,22
Another analysis that can be performed using isokinetic data is to divide the ROM into three phases: acceleration (A), load range (LR), and deceleration (D). LR is the phase with a sustained, set specific velocity. These three phases can provide some information, such as reaction time and ability to maintain velocity. These data can increase the clinical evaluation and implementation of specific protocols to optimize the treatment.23
Currently, no studies have investigated protocols using an isokinetic dynamometer for muscle strengthening as a form of conservative treatment in individuals with PCL injuries. Therefore, the primary purpose of this case report is to describe the effects of isokinetic exercises on the muscle performance and physical function of a soccer player with PCL injury and the second purpose is to observe the results compared to a matched control.
CASE DESCRIPTION
Subject Characteristics
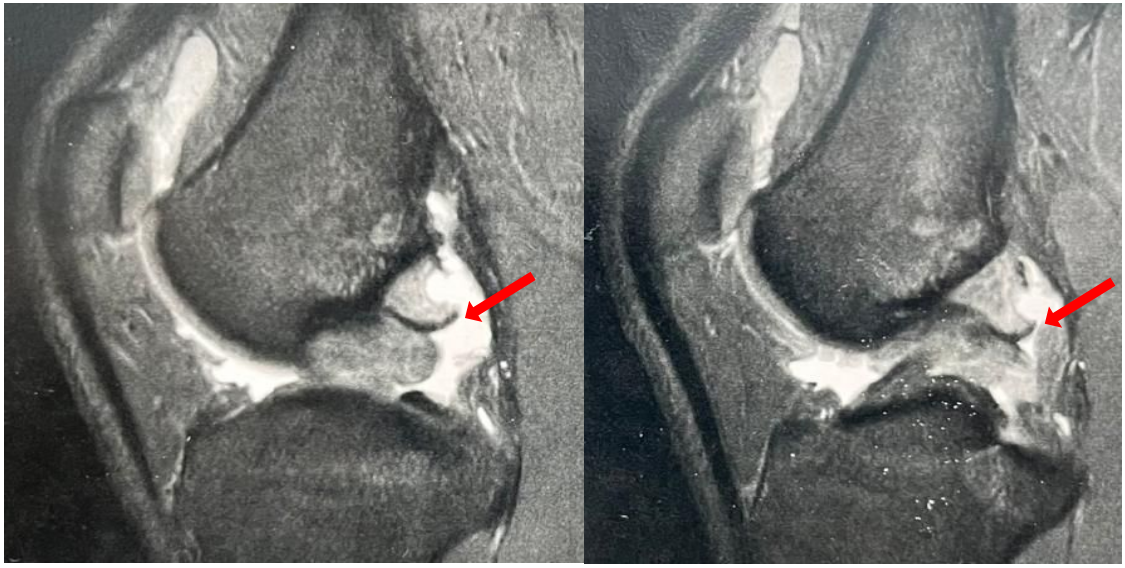
A 23-year-old male professional soccer player with a body mass index (BMI) of 22.1 kg/m², who plays as a left-back defensive specialist, was investigated in this case report. The participant reported spraining his non-dominant right knee while changing direction when running backward. Magnetic resonance imaging detected a Grade III PCL injury, accompanied by a partial rupture of the medial collateral ligament and a medial meniscal injury (Figure 1).

Preoperatively, the subject underwent a course of nonoperative management with a team of physical therapists, which was later deemed unsuccessful, leading to a recommendation for surgical consultation. According to the soccer team physical therapist and medical department, the initial and second phases of treatment (six weeks) were administered satisfactorily. The interventions included passive and active knee mobility exercises, quadriceps reeducation exercises (with or without neuromuscular electrical stimulation [NMES]), proximal hip strengthening exercises, bracing, weight-bearing precautions during gait, and cryotherapy. However, when progressing to functional exercises, strengthening, endurance, and neuromuscular control activities, the subject reported pain, instability, and a return of swelling, which hindered his treatment progress and return to sports. Consequently, surgical reconstruction and meniscal repair were recommended. Due to the risks associated with surgery and potential for complications, the subject opted for additional conservative treatment. Guided by the medical team, he was referred to the Laboratory of Biomechanics and Clinical Epidemiology at the University Hospital (Health Sciences Center) for a muscle performance assessment and to implement an innovative treatment that focused on increasing muscle strength.
The participants (the subject and a matched control) signed informed consent forms, and the study was approved by the IRB (#00768812.0.5231). Using the unaffected lower limb after ligament injuries as a control may have limitations, since muscle changes are not limited to the injured limb. Given this, another athlete from the same team, with similar anthropometric characteristics, was invited to participate and serve as a control for data analysis.
Initial Examination / Clinical Measures
The initial assessment consisted of a medical history followed by a physical examination, and a patient-reported outcome measure (PROM) to assess physical function. Two assessments were conducted pre- and post-treatment. The pre-treatment assessment occurred five months after the initial injury.
The anthropometric characteristics of the subject were as follows: age, 23 years; weight, 70 kg; height, 178 cm; and BMI, 22.1 kg/m2, and that of the control athlete were 21 years, 70 kg, 185 cm, and 20.8 kg/m2, respectively (used exclusively to compare the isokinetic performance).
The physical examination included the ROM, specific orthopedic tests (quadriceps active test, posterior drawer test, and posterior sag sign), and an examination muscle performance.11 The active flexion ROM was 120° and 0° extension. All specific orthopedic tests (quadriceps active test, posterior drawer test, and posterior sag sign) were positive. To assess muscle performance, the Biodex System 4® isokinetic dynamometer (Biodex Medical System Inc., Shirley, NY) was used in the concentric mode at angular velocities of 300°/s, 120°/s, and 60°/s, with a rest time of 90 s between each series. Finally, the Lower Extremity Functional Scale (LEFS) was chosen as a patient reported outcome measure. This instrument was used because of the absence of a specific PROM for PCL injury. This questionnaire consists of 20 items with responses from 0 to 4 points, with a maximum score of 80 points. The higher the score obtained, the better the participant’s physical function. The cut-off for clinically meaningful improvement is 11 (area under the receiver-operator curve, 0.96; 95% confidence interval [0.88;0.99].24
Procedures
Before the isokinetic test, a warm-up was performed on an ergometric bicycle for 10 min at a velocity of 30 km/h.25 The subject was positioned, seated on the dynamometer and stabilized by belts around his trunk, thighs, and ankle ipsilateral to the limb to be tested. The dynamometer axis was aligned with the lateral femoral condyle, and the ankle pad was positioned just above the medial malleolus. All calibration and gravity correction procedures adhered to the manufacturer’s instruction manual.26 The subject performed repetitions at each of the test velocities for familiarization prior to performing the test.
The subject was instructed to use maximum force during all repetitions, and verbal encouragement and visual feedback were provided. A coefficient of variation of < 10% for each series was considered acceptable, and a sampling frequency of 100 Hz was adopted.27 The results were presented compare involved, noninvolved, pre- and post-treatment, and are also compared to results from the control. Variables including peak torque (PT), peak torque normalized to body mass (PT/BM), angle of peak torque, and hamstring/quadriceps (H:Q) ratio were evaluated. The H:Q ratio was calculated by dividing the peak torque of the flexor by the extensor at 60°/s. A Matlab® program was used to analyze the percentage of LR according to the pre-stipulated ROM (0–90°), and the isokinetic variables were calculated during the sustained velocity phase (LR).28–30
Qualitative data were evaluated using 3D surface maps (Isomaps). The map was created using a Matlab® mathematical algorithm program, compiling the repetitions at each velocity based on the phase duration. The algorithm estimated the intrinsic geometry considering the torque (z-axis), joint angle (x-axis), and angular velocity (y-axis) in the same time interval. The z-axis defined the height of the map in relation to the force intensity, whereas the x- and y-axes formed the surface boundaries. Surface maps allow observation of the interaction between torque, velocity, and ROM. Three-dimensional surface map (3DTAV) analysis can help interpret isokinetic results and can be used to characterize muscle performance.29
INTERVENTION
Taking into account the history of the injury and data from the physical and functional examination, associated with the fact that the traditional conservative treatment did not achieve the expected result, an innovative treatment, based on isokinetic exercises, was proposed as the subject chose to decline surgical treatment.
The program consisted of 23 sessions over nine weeks. Each session was divided into a warm-up period (initially on an ergometric bicycle and, after the 6th week, on the dynamometer), followed by strengthening exercises in the isokinetic dynamometer, according to the weekly program stipulated based on the evolution of clinical signs presented by the subject, finishing with lower limb stretching exercises (Table 1). The strengthening exercises were performed only on the injured limb.
RESULTS
The percentage of sustained velocity (LR) based on pre-stipulated ROM, ROM, peak torque values normalized by body mass (PT/BM), and angle of PT (AngPT) are described in Table 2. For knee extension, PT/BM increased from 2.8 to 4 Nm/kg at 60°/s (control: 3.6 Nm/kg), from 2.0 to 3.4 Nm/kg at 120°/s (control: 2.9 Nm/kg), and from 1.5 to 2.0 Nm/kg at 300°/s (control: 1.9 Nm/kg). For knee flexion, PT/BM increased from 1.3 to 2.3 Nm/kg at 60°/s (control: 1.9 Nm/kg), from 1.6 to 2.1 Nm/kg at 120°/s (control:1.0 Nm/kg), and from 1.1 to 1.3 Nm/kg at 300°/s (control:1.2 Nm/kg).
Initially, the H:Q ratio for the affected limb was 69%, compared to 51% for the noninvolved limb. After the treatment program, the H:Q ratios improved to 57% for the affected limb and 46% for the unaffected limbs. The patient scored 71 points on the LEFS questionnaire in the pre-treatment assessment, indicating 88.7% lower-limb function. At the end of the treatment program, the score improved to 79 points, reflecting 98.7% of physical function.
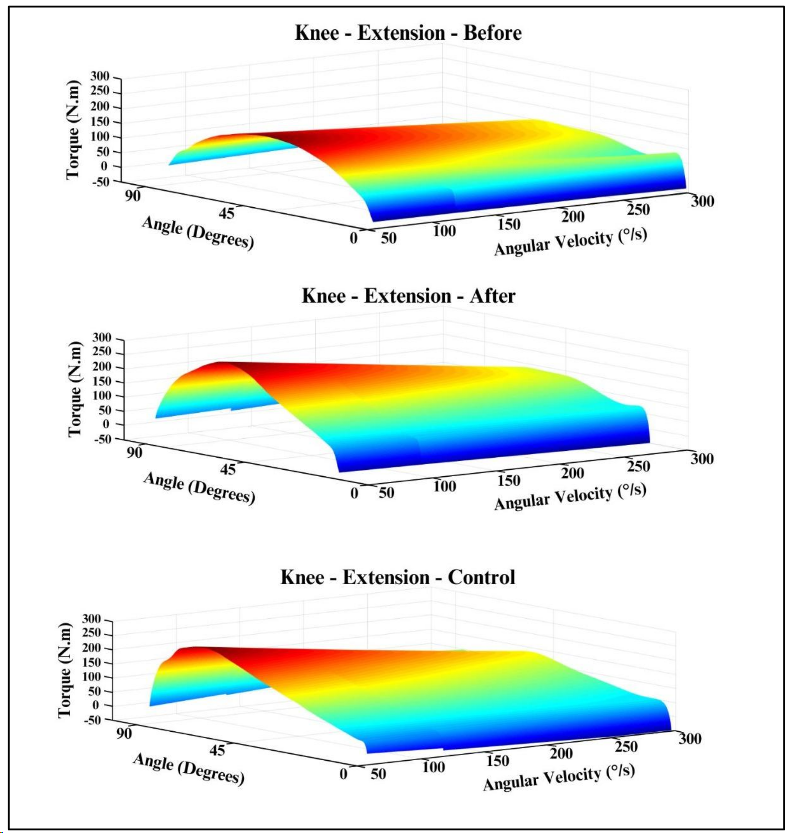
Figure 2 shows the 3DTAV of the affected knee extension compared to the control. The 3DTAV shows the patient’s improved ability to generate torque after the treatment program, exceeding that of the control athlete (color intensity is proportional to each surface in the entire ROM, with light gray/blue representing less torque).

DISCUSSION
Muscle strength measurement is crucial for evaluating and predicting muscle condition, alongside functional capacity. Studies support this concept, with isokinetic peak torque assessment being one of the most widely applied methods for evaluating lower extremity muscle strength in soccer players.31–33
To achieve satisfactory outcomes in both post-surgical and conservative treatments, recovery of quadriceps strength is crucial. Furthermore, knee stability during high-performance activities is vital to prevent posterior displacement of the tibia and mechanical stress on the PCL.13,18,34,35
This case report evaluated the effects of conservative treatment program, incorporating isokinetic exercises, on muscle performance and physical function in a soccer player with a PCL injury. Results indicated that for knee extension, PT/BM increased from 2.6 to 4 Nm/kg at 60°/s (control: 3.6 Nm/kg), from 2.0 to 3.4 Nm/kg at 120°/s (control: 2.9 Nm/kg), and from 1.5 to 2.0 Nm/kg at 300°/s (control: 1.9 Nm/kg). These values indicate a 42% increase in extensor torque generation at 60°/s. For knee flexion, PT/BM increased from 1.8 to 2.3 Nm/kg at 60°/s, from 1.6 to 2.1 Nm/kg at 120°/s, and from 1.1 to 1.3 Nm/kg at 300°/s. Comparative studies have shown that isokinetic strength performance profiles vary among elite soccer players based on field positions. For example, Śliwowski et al. indicated that the PT/BM of extensors at 60°/s for external defenders was 3.3 Nm/kg, while Delvaux et al. reported an average of 2.93 Nm/kg at 60°/s for quadriceps PT/BM in professional soccer players.31,36
The increased peak torque values can be attributed to the fact that isokinetic exercise is a muscle-strengthening modality that enables the development of maximal muscle tension throughout the ROM at constant velocity, thus recruiting a large number of muscle fibers, potentially requiring greater muscle performance compared to other strengthening modalities.37–39
The conventional H:Q ratio measured at an angular velocity of 60°/s in elite soccer players has been reported in several studies and has been used as a criterion for muscle imbalance and risk of injury in the knee joint.36,40,41 The pre-treatment H:Q ratio (69%) suggests a significant quadriceps weakness. After the isokinetic exercise program, this ratio dropped to 57%, approaching the values suggested by previous studies.41–43 Although the post-treatment H:Q ratio was slightly below 60%, some literature suggests that H:Q ratio imbalance in professional soccer players may be associated with high quadriceps strength and not low hamstrings muscle strength.40,42
The analysis of the isokinetic variables demonstrates that the affected limb incurred a decrease in the% LR (pre-treatment: 93.8%; post-treatment 92.8%). However, the values are higher than expected per the study of Mazuquin et al. Those authors analyzed the decomposition of these same variables in professional and under 17 soccer players and found an LR value of 83.2% for the dominant limb. The authors indicated that professional soccer players sustain the torque in a large ROM, showing greater muscular efficiency. Figure 1 shows a deficit in extensor torque generation in the affected limb pre-treatment. Post-treatment, the map demonstrates an improved torque generation capacity, surpassing that of the control.
As for the physical function, the score achieved in the LEFS questionnaire (79 points) post-treatment revealed that the subject returned to sports activities after the treatment program, reflecting 98.7% restoration of his lower-limb functionality. Although the LEFS questionnaire is a PROM, return-to-sports was primarily determined based on isokinetic performance values. Agolley et al. followed 46 athletes for five years after undergoing conservative treatment for Grade II and III PCL injuries. They found that the time to return-to-sports activity was approximately 10.6 weeks and after two years, 42 athletes continued their sports in the same category.44
Conservative management based on functional bracing and exercises is often reasonable for treating some athletes with PCL injuries. Although the PCL has an intrinsic ability to heal, residual posteriorization is a frequently observed disadvantage in conservative treatment. However, Shelbourne et al. reported that, on average, 14 years post-injury, patients had good subjective and objective outcomes not statistically significantly different between grades of PCL laxity. Most patients regained the functional ROM (and sufficient quadriceps strength) to return to activities of daily living, with 45% participating in jumping and pivoting activities.45
Recent research by Rasmussen et al. evaluated changes in patient reported outcomes using the International Knee Documentation Committee Subjective Knee Form (IKDC-SKF) over a two-year follow-up and muscle strength at an eight-month follow-up after exercise and support brace interventions for patients with acute PCL injuries. This study concluded that patients with acute isolated and multiligament PCL injuries treated with the physical therapy-led exercise and support brace intervention reported clinically relevant improvements from baseline to the two-year follow-up. Those authors acknowledged several limitations in the study, e.g., the lack of a control group.46
Some limitations of this case report can be described: a) the absence of performance-based functional tests alongside isokinetic variables for return-to-sports decisions; b) the absence of longer term follow-up assessments, c) a lack of evaluation of muscle performance in eccentric contraction/mode and other velocities, such as 180°/s, and d) the results found are unable to be generalized due to the nature of a case report.
CLINICAL IMPRESSION
The treatment for PCL injuries remains controversial. Surgical treatment can entail complications and conservative treatment has not shown robust results in clinical studies with a low risk of bias. The use of the isokinetic dynamometer, both for evaluation and treatment, has a high cost, however, professional soccer teams have previously used this type of resource and as there is a scarcity of clinical studies with a low risk of bias. The results of the current case report support an approach for managing a PCL injury in a professional soccer athlete that did not respond to conventional conservative treatment.
CONCLUSIONS
The use of an isokinetic exercise protocol with the isokinetic over the course of nine weeks of treatment, had a beneficial effect on maintaining physical function and improving extensor peak torque (42%), in addition to positively affecting the H:Q ratio of a professional soccer player with a posterior cruciate ligament injury, allowing for a successful return to sports.
Funding
The authors wish to thank the FINEP (MCT/AÇÃO TRANSVERSAL PRÓ-INFRA #01/2007 / #01/2009) for the funding to obtain the isokinetic dynamometer. KO and FQRC received doctoral financial support from CAPES (Funding Code: 001), PACS and RGM received a Fundação Araucária scholarship, and GRM and JRC also thanked the CNPq for their scholarships.
The authors report no conflicts of interest.