

INTRODUCTION
Hamstring strain injury (HSI) is a common injury in sports involving sprinting.1–3 For the prevention of HSI, sufficient muscle strength (especially eccentric muscle strength) is considered important to control the powerful external load on the hamstring that occurs from the end of the swing phase to ground contact during the sprinting.4,5 Recently, many studies have suggested a relationship between eccentric hamstring strength and HSI,6–8 and it is generally accepted that hamstring eccentric exercises are important for HSI prevention and rehabilitation in sports.
The Nordic Hamstring Exercise (NHE) is a typical hamstring eccentric exercise, and NHE training provides benefits such as increased eccentric hamstring strength and lengthening of muscle fascicle length that can reduce the risk of hamstring strain injury.9–11 In their systematic review, Van Dyk et al. concluded that the programs that include the NHE reduce hamstring injuries by up to 51%.12 However, the NHE as a HSI prevention exercise has a low adoption rate, with only approximately 13% in men’s professional football teams in Europe adopting this exercise.13 Low compliance may be related to athletes’ experience of muscle stiffness and soreness after NHE training. To eliminate these potential barriers to adopting NHE as a preventive exercise for HSI, it is important to develop appropriate exercise strategies in order to implement the NHE safely and efficiently.
NHE performance is generally evaluated by the eccentric force during NHE, which is the vertical force on the part holding the leg,14,15 and eccentric force during NHE is considered useful for predicting HSI risk.16,17 Previous authors have reported a small or no correlation between eccentric force during NHE and eccentric knee flexor torque measured by an isokinetic dynamometer,18,19 suggesting that some factors other than eccentric knee flexor strength contribute to NHE performance. Interestingly, during NHE, not only knee joint torque but also hip joint torque occurs, and muscle activity of the hip and trunk extensors, such as the erector spinae and gluteus maximus, is also observed,20–22 indicating the importance of hip and trunk extensor strength during NHE performance. The deadlift is a classic strength training used to strengthen the hip and trunk extensors,23–25 and similarities to NHE in hamstring muscle activity during exercise have also been reported26; however, the similarity of peak force between the two exercises has not yet been determined. Clarifying the relationship between eccentric force generated during the NHE and the one repetition maximum (1RM) of deadlift, which reflects the hip and trunk extensor strength, will provide new insights into the importance of hip and trunk extensor strength during the NHE, and may also help demonstrate the usefulness of deadlift as an appropriate exercise to perform before progressing to NHE.
Therefore, in the present study, the relationship between the eccentric force during the NHE and the 1RM of deadlift was examined. It was hypothesized that the eccentric force during the NHE would be correlated with the 1RM of deadlift.
MATERIALS AND METHODS
Participants
Forty-nine healthy young rugby players, who were the top players in their region, were recruited for the present study. Participants habitually performed resistance training, including of the knee flexors two to three times a week for at least one year, and had sufficient experience with NHE. None of the participants had experienced hamstring strain or knee-joint injury. A sample size calculation was performed using G*Power 3.1.9.6. Assuming a two-tailed test for the population correlation coefficient with an expected correlation coefficient of 0.4, a significance level of 5%, and a power of 80%, the required sample size was calculated to be 44 cases. This study was approved by the institutional ethics committee and was conducted in accordance with the principles of the Declaration of Helsinki. The study procedures and potential risks were explained to the participants, and each provided written informed consent before participating in the study.
Experimental design
This cross-sectional study was conducted over a single day. After the warm-up, the participants performed the NHE and 1RM deadlift, as explained below. The two tests were performed in random order with adequate rest between the two.
Eccentric force during the NHE
For eccentric force evaluation, each participant was placed in a kneeling position on a custom-made NHE device (4Assist Inc, Tokyo, Japan) with each ankle secured above the lateral malleolus with an ankle brace attached to a load cell sensor (Figure 1). The force acting on the ankle brace in the vertical direction was quantified using a load-cell sensor. Force data were synchronized and transferred at 1,000 Hz from a PowerLab16/35 data acquisition and analysis system (AD Instruments, Bella Vista, NSW, Australia) to a personal computer (VersaPro; NEC Corporation, Tokyo, Japan). Each participant was instructed by the examiner to gradually lean forward from the initial kneeling position at 90° knee flexion to a prone position over three seconds, with the arms crossed at the chest and hip joints fully extended, and the ankle was passively secured in the dorsiflexed position. Before testing, the participants practiced the NHE two to three times. To standardize the velocity of movement, the participants were instructed to lean forward at a constant angular velocity, as indicated by a metronome. Eccentric force data was corrected for body mass (N/BM), and the peak eccentric force of both legs and the total peak eccentric force of both legs were used for further analyses.

1RM deadlift performance
Before testing, the participants performed three rounds of warm-up trials with submaximal effort. The 1RM of the deadlift was calculated from the weight that could be raised three times (x kg) using the estimation formula (x kg / 0.93) and corrected for body mass (kg/BM)
Statistical analyses
The Shapiro–Wilk test was used to assess the normality of the measures. Since some parameters were not normally distributed, Spearman’s rank correlation coefficients were used to examine the relationships between the peak eccentric force during the NHE and the 1RM deadlift performance. The following correlation criteria were adopted: 0, none; r < 0.4, weak, r < 0.7, moderate; r < 0.9, strong; 1, perfect.27 Statistical significance was set at p < 0.05. Statistical analyses were performed using the SPSS software version 27 (SPSS Inc., Chicago, IL, USA).
RESULTS
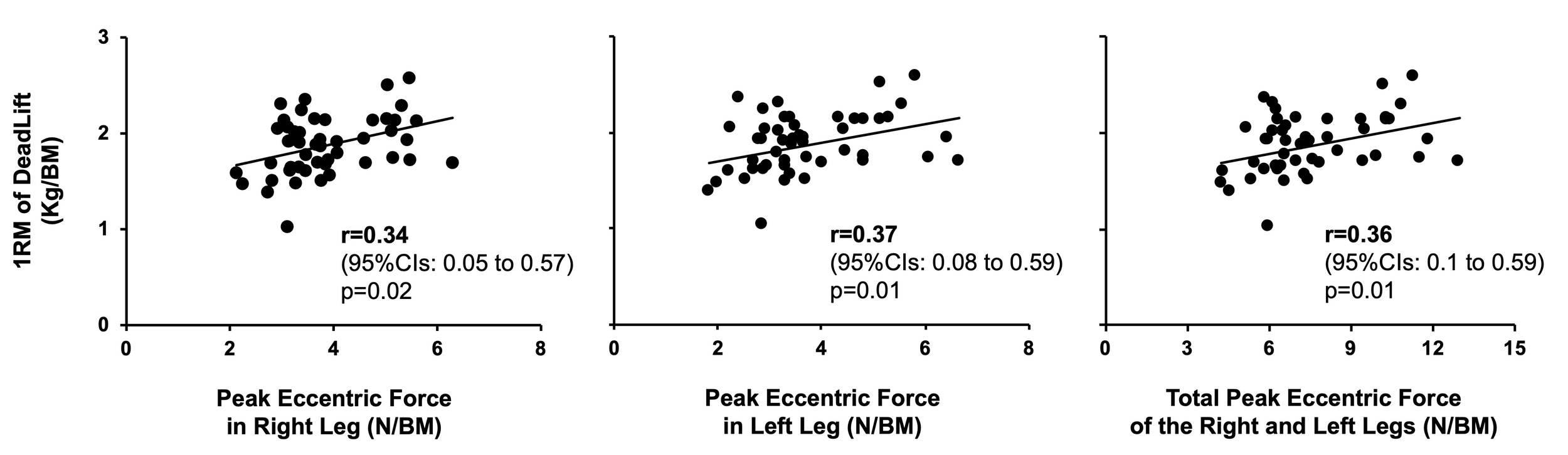
Participant’s physical characteristics are shown in Table 1. Table 2 presents the variables in peak eccentric force during NHE and 1RM of deadlift. Figure 2 shows the correlations between the peak eccentric force during the NHE and the 1RM of the deadlift. Notably, a weak but significant correlation was found between the 1RM of the deadlift and the peak eccentric force in the right (r = 0.34, p = 0.02) and left legs (r = 0.37, p = 0.01) and the total peak eccentric force of both legs (r = 0.36, p = 0.01).
DISCUSSION
The present study found weak correlations between the peak eccentric forces during NHE and the 1RM of a deadlift (r = 0.34–0.37). These results support the hypothesis.
Previous authors have reported a limited correlation between the eccentric force during NHE and eccentric knee flexor strength measured using an isokinetic dynamometer.18,19 van Dyk et al. found a weak correlation (r = 0.35) between eccentric force during NHE and eccentric knee flexion torque at 60 ̊/s, and the authors previously reported no correlations between the peak eccentric torque during NHE and peak eccentric knee flexion torque (r = 0.24).18 Taken together, this would indicate that NHE performance is not expected to reflect only knee flexor strength. Previous authors have indicated that hip joint torque was about half the knee joint torque,22 and muscle activity of the both the hip and trunk extensors20–22 occurred during the NHE. In addition, exercises emphasizing hip extension improve eccentric force during the NHE,10,28 suggesting an association between eccentric force during NHE and hip and trunk extensor strength. However, to the best of the authors’ knowledge, no previous study has considered the relationship between the eccentric force during NHE and hip and trunk extensor strength. This was the first study to examine the relationship between eccentric force of the hamstrings during NHE and the 1RM of deadlift, which both reflect hip and trunk extensor strength, and may provide new insights into the importance of hip and trunk extensor strength in NHE.
In the present study, the correlation between eccentric force during NHE and the 1RM of deadlift was weak (r = 0.34–0.37). The eccentric force during the NHE reflects the exerted muscle force during an eccentric muscle contraction, whereas the 1RM of deadlift reflects the exerted muscle force during a concentric muscle contraction. This difference in contraction mode may be reflected in the weak correlation. The degree of correlation between the eccentric force during the NHE and 1RM of deadlift was similar to that reported in a previous study between the eccentric force during the NHE and eccentric knee flexor torque measured using an isokinetic dynamometer (r = 0.35).19 Thus, lower-extremity muscle strength may not be a crucial factor in determining NHE performance. Previously, it was shown that individuals who were able to lean their bodies forward closer to the floor during NHE were able to exert greater eccentric force during NHE,18 suggesting the importance of ability to control NHE movements. Trunk extensor muscle activity has been observed during NHE21,22 and is thought to play an important role in controlling NHE movements. In the future, it will be necessary to examine not only the magnitude of lower limb muscle strength but also the magnitude of muscle activity in the trunk muscles during the NHE and whether the muscle activity patterns of the hamstring, trunk muscle group, and hip extensor muscle group during NHE affect the eccentric force produced during NHE.
The effectiveness of NHE for the prevention of HSI has been made clear in previous studies12; however, even in soccer, which has a very high incidence of NHE, the adoption rate of NHE for prevention is remarkably low (13%).13 As transient muscle damage to the hamstrings has been reported after the NHE,29 there are potential barriers, such as post-training muscle stiffness and soreness, which may contribute to a lower adoption rate. As it is difficult to control the NHE intensity and load on the muscles, the safe and efficient implementation of NHE in a phased training program requires exploring the exercises that may be performed before progressing to the NHE. Previous authors have suggested that the deadlift may be an appropriate exercise to consider for progressing to the NHE. The deadlift is typically considered for hip extensor muscle strength training. The electromyographic (EMG) activity of the hamstring during a deadlift is reported to be approximately 20–30% less than that observed during the NHE,26,30 and EMG activity above 60% of maximal voluntary isometric contraction was observed in the erector spine and lumbar multifidus during a deadlift, which are also active during in NHE.23,24 Moreover, Boyer et al., examined the muscle activation ratios of semimembranosus (SM/Hamstring), semitendinosus (ST/Hamstring), biceps femoris (BF/Hamstring) in total hamstring muscle activation as an index of the contribution of each muscle to the global activation of the hamstrings, and reported that the SM/Hamstring (r = 0.66; p = 0.005), ST/Hamstring (r = 0.42; p = 0.05), and BF/Hamstring (r = 0.60; p = 0.01) activation ratios were moderately correlated between NHE and stiff-leg deadlift.26 These results indicate that the muscle activation patterns during the two exercises are similar within participants and support the idea that the deadlift may be an appropriate exercise for progressing to the NHE. However, the present study showed only a weak correlation between peak eccentric force during the NHE and 1RM of the deadlift. Therefore, the similarity between the two exercises in peak force may play only a limited role in supporting the idea that the deadlift is an appropriate exercise to perform before progressing to the NHE. Considering the difficulty of the exercise and the load on the hamstring, the deadlift is often considered safer than NHE, but further studies are required to clarify its usefulness as an appropriate exercise to perform before progressing to NHE due to the differences in muscular action.
Some limitations of this study must be addressed. Although the 1RM of deadlift was measured in this study, variations in exercise form between individuals may have affected the contribution of each joint. To reduce form variation, it was necessary to select an exercise that is easier to standardize, such as the stiff-leg deadlift, which emphasizes hip extension. As the relationship between the exerted muscle force and deadlift is based on the force exerted during different contraction modes, it may be necessary to examine the relationship when the contraction mode is the same. In addition, the 1RM of deadlift is not a measure of pure trunk and hip extensor strength; therefore, it will be necessary to examine the relationship between hip extensor strength and trunk extensor strength in single-joint movement, and the eccentric force occurring during the NHE to clarify the contributions of trunk and hip extensor strength during the NHE.
CONCLUSION
The results of the present study indicate that weak correlations exist between the peak eccentric force during the NHE and the 1RM of deadlift (r = 0.34–0.37). These results may play only a limited role in supporting the idea that the deadlift is an appropriate exercise to perform before progressing to the NHE.
CONFLICTS OF INTEREST
There are no conflicts of interest to declare.
ACKNOWLEDGEMENTS
We would like to thank all the participants who volunteered as research subjects.