INTRODUCTION
Anterior cruciate ligament (ACL) injuries are the most common knee ligament injuries among athletes.1 The annual incidence rate is 68.6 per 100,000 person-years,2 and ACL injuries are estimated to increase further in the future.3 Following injury, many athletes undergo reconstructive surgery in the hope of return to sport (RTS) “at their pre-injury competitive level”.4 However, a significant portion of patients—approximately 40%—fail to RTS at their pre-injury competitive level after ACL reconstruction (ACLR).5 Hence, it becomes imperative to identify factors that hinder successful RTS at the pre-injury competitive level after ACLR.
One of the key physical functional characteristics associated with RTS after ACLR is asymmetry in the single-leg hop (SL hop) distance. The horizontal SL hop serves as a standard test to gauge physical readiness for RTS.6 However, previous studies examining the relationship between horizontal SL hop and RTS at pre-injury competition level have presented conflicting outcomes. Some studies demonstrated a statistical association,7–10 while others did not,11–13 resulting in an absence of consensus. Therefore, recent research highlights the necessity to reevaluate the use of SL hop asymmetry as a criterion for safe RTS.14
In recent years, vertical jumps (specifically, single-leg vertical jump [SL vertical jump] and single-leg drop jump [SL drop jump]) have gained prominence as crucial performance tests post-ACLR.14 Kinematically, vertical jumps exhibit higher knee joint power than horizontal jumps and, therefore, more accurately detect functional asymmetries after ACLR compared to SL hops.15,16 The SL drop jump is a commonly used plyometric exercise or test that relies on the adequate development of critical motor abilities such as explosive strength and stretch-shortening cycle capacity.17 Performance variables in SL drop jump include jump height, ground contact time, and the reactive strength index (RSI), calculated from their ratio. Previous authors have described significant group differences in SL vertical jump height and RSI in SL drop jump post-ACLR, despite the absence of significant differences in SL hop.17–19
Moreover, earlier studies investigating the risk of re-injury post-ACLR demonstrated that the contralateral injury group had a lower RSI during the SL drop jump compared to the non-contralateral injury group.20 However, to date, no study has established an association between those who do not successfully RTS (No-RTS) and vertical jumps post-ACL. Clarification of the association between No-RTS and vertical jumps post-ACLR would offer valuable insights into safe postoperative RTS.
Force plates and 3-dimensional analysis systems are necessary to accurately measure RSI. Although these evaluations are the gold standard, their use is limited due to cost and difficulty of use.21 In recent years, technology has improved, and RSI can be evaluated using infrared sensors and smartphone applications; their reproducibility is high and their validity has been demonstrated to be comparable with that of force plate measurements.22,23 Therefore, RSI measurement has become clinically friendly, and evaluation of RSI during a vertical jump after ACLR can provide objective data on recovery for professionals involved in postoperative care.
This study aimed to determine the association between vertical jump performance after primary ACLR using hamstring tendon autograft and RTS at a pre-injury competitive level. The study hypothesis was that participants who returned to pre-injury competition after ACLR who perceived that they had not achieved RTS at their pre-injury competition level would exhibit an excess asymmetry in performance variables during vertical jump compared to those who perceived that they had achieved it.
MATERIALS AND METHODS
Participants
Participants who underwent primary ACLR using hamstring tendon autograft between April 2012 and December 2020 were included if they met the following criteria: (1) aged between 16 and 45 years at the time of study participation, (2) engaged in sports with a modified Tegner activity scale score24 ≥ 5 before their ACL injury, (3) elapsed time of more than eight months since ACLR, (4) participated in sports after surgery, with physician’s permission, (5) failed to measure SL hop or vertical jump, and (6) expressed intention for RTS before surgery. Participants were excluded if they met the following criteria: (1) underwent surgery other than ACLR six months before reconstruction, (2) underwent multiple ligament reconstruction and lateral extra-articular tenodesis, (3) had a cartilage injury requiring surgery, (4) underwent ACLR previously, (5) had difficulty visiting the clinic due to distance or social reasons, or (6) had missing questionnaire data. Given the distinct characteristics of muscle strength and SL hop asymmetry after ACLR depending on the graft type, this study opted to unify the graft type as hamstring.25
A priori sample size estimation was performed using the G*Power software package (version 3.1.9.4, Kiel University).26 The input parameters were as follows: statistical test = means (difference between two independent means [two groups]), tail = 2, effect size = 0.8, α error probability = 0.05, power = 0.8, and allocation ratio = 0.6. The allocation ratio was determined based on the observed rate of return to sports after ACLR (approximately 60%).5,27 The target sample size was set at 56 participants (Yes-RTS group = 35, No-RTS group = 21). Ethical approval was obtained from the Ethics Committee (approval number: M2016-197). All participants provided written informed consent before participation in the study.
Procedure
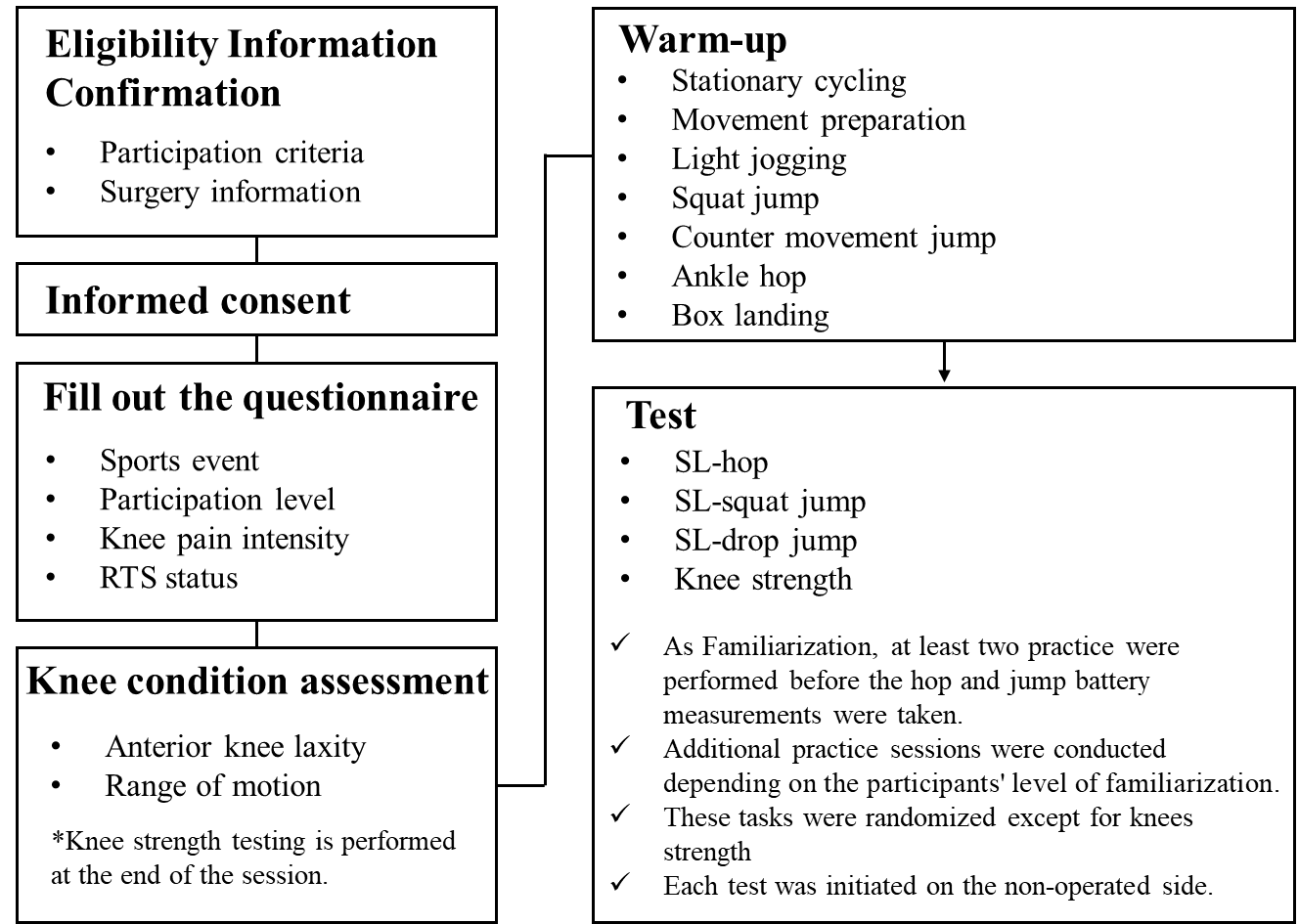
This cross-sectional study was conducted at a single center. Demographic and surgical data were obtained from medical records and questionnaires. Demographic data included age, sex, activity level (modified Tegner activity scale24), participation level, and injury mechanisms. Participation levels were categorized as recreational, competitive, or elite.28 Surgical data included graft type, presence of meniscal repair, number of months since surgery, date from ACL injury to surgery, and number of months from surgery to measurement. Knee condition, SL hop, and SL vertical jump and SL drop jump were measured on the same day. In addition, participants completed a questionnaire regarding their RTS status at the time of study participation. The measurement procedure is shown in Figure 1. The order of hops and jump batteries was randomized to reduce the effects of fatigue over time, and the rest periods between hop trials were not standardized, rather were determined by patient readiness.29 Each test was initiated on the non-operated side. Before commencing the test session, participants performed stationary cycling (5 min), light jogging indoors (30 s), movement preparation (calf raise, squatting, lunging), squat jump, countermovement jump, ankle hop, and box landing in accordance with previous study methods.23 Participants performed movement preparation, jump, hop and landing, 5–10 repetitions each.

Surgical Technique and Postoperative Rehabilitation
The autograft source was the hamstring (semitendinosus). Hamstring surgery involved anatomical double-bundle reconstruction. In cases where the semitendinosus alone proved insufficient as a graft tendon, the gracilis was added. All surgeries were performed by orthopedic surgeons specializing in knee joints. The surgical technique and postoperative rehabilitation protocol were based on previous research.30 Exercises for range of motion (ROM) and isometric muscle contraction commenced three days post-surgery. Initially, a straight-position knee-joint immobilizer (knee brace; ALCARE Co., Ltd., Tokyo, Japan) and crutches were used and then gradually phased out over four weeks post-ACLR. Jogging commenced three months post-ACLR, with a gradual increase in running speed. RTS was permitted upon meeting specific criteria: a minimum of six months post-ACLR, a limb symmetry index (LSI) of SL hop distance > 90%, and achieving sufficient knee strength recovery (i.e., isokinetic extension and flexion torque LSI > 85%, measured using an isokinetic dynamometer [BIODEX System 4, BIODEX Medical Inc., Shirley, NY] at 60°/s and 180°/s). Participants who underwent repair of the middle-posterior segment lesions of the meniscus were advised against deep squatting beyond 90° until three months post-ACLR.31
Knee Condition Assessments
In this study, knee conditions were evaluated, encompassing anterior knee laxity, ROM, strength, and knee pain intensity during sports activities. These assessment methods are considered standard with proven reproducibility.32–35
Anterior knee joint laxity
Anterior knee joint laxity was measured using a KT-1000 instrument (MEDmetric Corp., San Diego, CA, USA). The amount of forward tibial translation at maximum pull was measured twice, and the maximum value was recorded.36 The difference between the non-operated and operated leg values was then calculated.
Range of motion
Passive knee flexion and extension ROM were measured in increments of 1° using a goniometer.37 The assessment of knee extension was conducted with the patient’s heel elevated with a support, allowing for hyperextension when present.38 Normal extension of the knee was considered in the 0° position. A positive ROM score for extension was used for hyperextension. A negative ROM score for extension meant that the patient was unable to reach the 0° position.39 For flexion ROM, the cue was to flex the knee to maximum flexion with the heel on the support surface, using the assistance of hands rather than only the participant’s own muscle strength. The examiner verified that the participant’s hip internal/external rotation and knee valgus/varus were in the intermediate position before measuring the ROM. ROM deficit was defined as the angle obtained by subtracting the value on the operated side from that on the non-operated side.
Strength
Strength assessment was conducted using the Biodex isokinetic dynamometer. Extensor and flexor peak torques were evaluated at angular velocities of 60°/s and 180°/s. Peak torque was expressed as Nm divided by body weight (Nm/kg). Additionally, the LSI was calculated as follows: LSI= ([operated value]/[non-operated value])×100 %.
Knee pain intensity during sports activities
Participants were instructed to rate the intensity of their knee pain during sports activities on a numerical rating scale (NRS) of 0–10.40
Single-Leg Hop Test
The SL hop measurement method employed in this study was based on previous research.33 Participants stood on one leg behind a marked line (starting point), hopped forward as far as possible, and landed on the same leg. Arm swing/movement was not restricted in this study based on the results of a previous study41 that showed that work by the knee was not significantly altered by the presence or absence of an arm swing during a hop. Each participant completed three practice hops, followed by two successful trials. An unsuccessful hop was characterized by an additional hop on landing, early touchdown of the contralateral limb, and/or loss of balance. A successful trial was defined as one in which the failure criteria were not met, and the participant could maintain the posture for 3 seconds after landing. The distance from the starting line to the point where the back of the participant’s heel made contact with the ground after a single hop was recorded. The average distance between two trials was recorded. In addition, the LSI was calculated. Previous studies have reported high test-retest reliability (intraclass correlation coefficient [ICC]= 0.91, 95% confidence interval 0.87–0.94) and interrater reliability (ICC= 1.00, 95% confidence interval 1.00–1.00).42
Single-Leg Vertical Jump Test
SL vertical jump was measured using a force plate (260AA6; Kistler Instrument AG, Winterthur, Switzerland) with a sampling rate of 1000 Hz. The vertical ground reaction force (VGRF) data were filtered through a fourth-order Butterworth low-pass digital filter at a cut-off frequency of 50 Hz and normalized to body weight using software (IFS-4J/3 J, DKH). Participants stood on one leg of the force plate with the opposite hip and knee bent at 45° and 90°, respectively. The arm swing of the vertical jump was restricted in this study considering the results of a previous study that showed smaller work by the knee during vertical jumps with arm swing compared to vertical jumps without arm swing.43 To control for arm movements, participants crossed their arms, placing each hand in the opposite axilla. Additionally, counter-movements during jumping were restricted to eliminate the effects of the SSC and focus on concentric muscle contraction.44 The participant performed a vertical jump from a single-leg squat position and landed on the ipsilateral leg.44 A trial was deemed unacceptable if the sole of the opposite foot touched the force plate or floor, part of the sole of the foot fell outside the force plate during single-leg landing, the foot moved or slid after single-leg landing, or the arms were removed from the chest. Participants were instructed not to intentionally prolong their flight time upon landing. Each participant performed three practice jumps followed by two successful trials. The flight time during single-leg SJ was calculated. (Table 1).45
The average jump height (cm) was recorded, and the LSI of jump height was calculated. Moderate-to-excellent reliability was established using the flight time method.46,47 The ICCs (1, 2) for SLVJ on the operated and non-operated sides ranged between 0.96–0.99 and 0.92–0.98, respectively, demonstrated nearly perfect reproducibility in the previous study.19,48
Single-Leg Drop Jump Test
SL drop jump assessment methodology was based on previous studies.17,49 A 15-cm-high box was positioned in front of the force plate. Participants stood on the step using their designated leg, with the opposite hip at 45° and the opposite knee at 90°, maintaining neutral hip rotation. For the same reasons as for the SL vertical jump, the participants’ arm swing during the task was restricted. To control for arm movement effects, participants were instructed to cross their arms. After they stepped off the box, they completed a vertical jump as fast (with short ground contact times) and as high as possible. A successful landing was defined as maintaining stability for 3 seconds. Unacceptable trials included instances where the arms left the chest, the foot landed outside the force plate area, post-landing foot movement or sliding occurred, or the sole of the opposite foot contacted the force plate or floor. Each participant completed a minimum of three practice jumps followed by a single successful trial for the formal test. Notably, appropriate familiarization and the implementation of standardized warm-up and testing protocols required only one trial when evaluating RSI or jump height during the SL drop jump (ICCs [single measures] value > 0.90).50
The SL drop jump was measured using the force plate. Contact time, flight time, jump height, and RSI during the task were calculated based on a previous study (Table 1).17 Additionally, the LSI was calculated.
Return to Sports Status
Participants return to the same competitive level as before the injury was defined using two questions.11 The first question asked, “Have you returned to the same level of competition as before your ACL injury?” with participants providing a Yes or No response. This question has been used most frequently in prior studies.10,51–54 The second question was, “What is the subjective performance intensity of the sport you are currently participating in (assuming 100% of your pre-injury performance intensity)?” with participants indicating their response on a scale of 0–100%.30 This question is called the Postoperative Subjective Athletic Performance (PoSAP), in which participants were asked about their performance intensity when playing a specific sport. Ohji et al.30 reported that most post-ACLR patients with a PoSAP of 80% responded “Yes” to the dichotomous question. They noted that relying solely on this question tended to overestimate their RTS status. Therefore, in this study, participants who answered “Yes” to the dichotomous question and had a PoSAP of > 80% were categorized into the Yes-RTS group. The No-RTS group included patients who met none or one of these criteria.11
Statistical Analysis
The normality of each variable’s distribution was determined using a histogram and the Shapiro–Wilk normality test.55 Means and standard deviations were calculated for normally distributed variables, whereas medians (interquartile range) were calculated for non-normally distributed variables.
Differences in demographic data, knee strength, SL-vertical jump, and SL drop jump variables between the Yes-RTS and No-RTS groups were analyzed using a range of statistical tests: chi-square test, Fisher’s exact test, multiple comparison test (The Bonferroni method), unpaired t-test, or Mann–Whitney U test. Effect sizes (chi-square test = phi coefficient, Fisher’s exact test = Cramer’s V, t-test = Cohen’s d, Mann–Whitney U test = r) were calculated for each variable. Phi coefficient and Cramer’s V defined >0.5 as large effect.56 Cohen’s d defined 0.2 as small, 0.5 as medium, and 0.8 as large.57 The Mann-Whitney U test r was defined as 0.1 for small effect, 0.3 for medium effect, and 0.5 for large effect.57 The significance level for knee condition and performance tests (SL hop, SL vertical jump, and SL drop jump) was adjusted to less than 0.5% using the Bonferroni method to mitigate the risk of type I errors. This adjustment was made to account for multiple comparisons. Statistical analyses were conducted using SPSS version 28.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The study included 65 patients who underwent primary ACLR, with a mean age of 21.0 (5.0) years, of which 29 were female. The median postoperative duration was 13.5 months (interquartile range: 13.0 months), with 39 patients (60%) assigned to the Yes-RTS group (Table 2).
No statistically significant differences were observed in demographic or surgical data between the groups (Table 2). Group differences in knee conditions are shown in Table 3. The No-RTS group exhibited higher knee pain NRS scores during sports activities (p < 0.001, r = -0.45) compared to the Yes-RTS group. However, no significant differences were observed between the groups in terms of anterior knee laxity, ROM, or strength. Descriptive statistics for the operated and non-operated sides are shown in Table 4.
Regarding the performance tests (Table 5), no significant differences were observed in the LSI for SL hop and SL vertical jump. However, in the SL drop jump, the No-RTS group displayed lower LSI in RSI compared to the Yes-RTS group (p = 0.002, d = 0.81). Descriptive statistics for the operated and non-operated sides are shown in Table 6.
DISCUSSION
In this study, the relationship between No-RTS and vertical jump performance asymmetry after primary ACLR using hamstring tendon autograft was examined. As hypothesized, the No-RTS group had lower value in RSI symmetry during the SL drop jump compared to the Yes-RTS group. However, no statistical association was found between LSI in SL hop distance, SL vertical jump height, and RTS. Findings from this study partially supported the authors’ hypothesis.
The RTS rate among the study participants stood at 60% (39/65), consistent with a meta-analysis exploring RTS rates post-ACL (61.8%).5 The self-reported RTS rate for current study participants was 72% (47/65) when only answered whether or not they RTS (dichotomous question). In the present study, PoSAP were aggregated to prevent an overestimation of RTS at pre-injury competition levels. Notably, 40% of patients meeting standard sports participation criteria and resuming sports activities failed to reach their preinjury athletic status.
No significant differences were observed between the two groups in terms of LSI in SL hop distance and SL vertical jump heights. Previous studies indicate that vertical jumps have a more substantial impact on the knee joint compared to horizontal hops.58,59 Consequently, the initial hypothesis suggested tha a lower LSI in SL vertical jump height woud be seen in the No-RTS group compared to the Yes-RTS group. However, the study’s findings did not support this hypothesis. Among patients engaged in sports after ACLR, many exhibited significant symmetry improvement with a SL vertical jump height. SL hop in this study was 127.9 cm on the operative side and 129.6 cm on the non-operative side, and SL vertical jump was 12.6 cm on the operative side and 13.9 cm on the non-operative side. These results were consistent with those of similar previous studies.11,19 However, the values of these test batteries varied widely depending on the demographics of the participants and the method of measurement (arm swing or countermovement). Therefore, caution should be taken when interpreting the values.60–63
In the SL drop jump, the No-RTS group demonstrated a lower LSI in RSI compared to the Yes-RTS group. RSI serves as a valid measure of explosive strength and stretch-shortening cycle capacity, crucial for most sports.64 Therefore, achieving balanced RSI improvements is a critical factor for successful RTS post-ACLR. The RSI for the study participants’ was 0.33 on the operated side and 0.38 on the non-operated side, which falls within the range of data from previous studies measured at the same height (operated side: 0.28-0.34, non-operated side: 0.37-0.44).49,65–67 Although the sex and postoperative follow-up time differ from these previous studies, the data from this study can be used as a reference value.
The explanation for the lack of group differences in the LSI of SL vertical jump and the significant group differences in the LSI of SL drop jump is presumably due to differences in jumping characteristics. In the present study, to evaluate concentric muscle force capacity in SL vertical jump, counter movements during jumping were restricted to a minimum.19,44 On the other hand, the SL drop jump task was set to jump higher with a shorter ground contact time to evaluate the ability to exert explosive muscular force. The results of the present study suggest that explosive muscle exertion is more important for competitive performance in the post-ACLR.
When assessing knee conditions, the No-RTS group reported higher NPRS scores for knee pain than the Yes-RTS group. Persistent knee pain post-ACLR has been reported as a negative factor for RTS, and the findings from the present study align with those from previous studies.53,54 In previous studies, the presence of knee pain symptoms one year after ACLR was linked to a lack of physical or psychological readiness.68 Incorporating findings from previous studies, controlling persistent knee pain emerges as a challenge in postoperative RTS. The detailed etiology of pain in this study remains unknown, indicating the need for further evaluation. The values of ROM deficit in this study were very small in both groups. However, in a previous study, the standard error of measurement of ROM using a goniometer (flexion/extension: 3.41/1.62 degrees) was greater than that using a smartphone app (flexion/extension: 2.72/1.18 degrees).69 Future studies should consider measuring with tools with better accuracy.
When aiming for RTS after ACLR, it is important to progress gradually through criterion-based or task-based rehabilitation and ultimately pass the RTS test.70–72 Generally, the RTS test primarily encompasses knee strength and SL hop, with only a small percentage dedicated to vertical jump tasks.6,73 Based on these results, the functional aspects of the RTS criteria can be enhanced by adding the RSI of the SL drop jump as well as the distance data of the SL hop.
This study has some limitations. First, it only included patients who had undergone reconstruction using hamstring tendon autograft to control for specific characteristics,25 potentially overlooking differences that may be seen with other graft types such as bone-patellar tendon-bone or quadriceps tendon. The study’s recruitment process might also have introduced selection bias, as only respondents were included. Additionally, the previously utilized RTS criteria did not incorporate vertical jump tasks, which might have led to significant group differences in unassessed parameters. A detailed biomechanical analysis of vertical jump tasks, crucial for understanding lower extremity joint biomechanics, was not conducted.74 In this study, arm swing was not standardized for each motor task. Since hop distance and jump height differ with and without arm swing, caution should be considered when interpreting the results.41,43 This study did not include patient-reported outcomes related to RTS at a pre-injury competitive level, such as the International Knee Documentation Committee Subjective Knee Form. Therefore, the subjective knee function status of the study subjects was undetermined.54 Furthermore, the study’s conservative data correction using the Bonferroni method might have implications for type II errors. Future multivariate analyses with larger sample sizes are necessary to address these limitations. However, this is the first study to characterize asymmetry in vertical jump performance in RTS at their preinjury competitive level after ACLR. The strength of this study is that it demonstrates the importance of vertical jump performance assessment, which has been the focus of much attention in recent years. In addition, another strength of this study is the inclusion of potentially confounding knee condition variables in the analysis.
CONCLUSION
Patients unable to report achieving RTS after primary ACLR using hamstring tendon autograft are more likely to exhibit asymmetric performance, especially for explosive characteristics (e.g., RSI), suggesting the significance of assessing jump symmetry in evaluating post-ACLR rehabilitation success.
Conflicts of interest
The authors certify that there are no conflicts of interest with any financial organization regarding the material discussed in the manuscript.