ANTERIOR CRUCIATE LIGAMENT INJURIES
Anterior cruciate ligament (ACL) injuries are prevalent in athletic populations, with approximately 80,000 to 250,000 ACL injuries occurring annually in the United States alone.1 Approximately 100,000 individuals undergo ACL reconstructions (ACLR) annually, making it the sixth most common orthopedic procedure in the United States.1 The incidence of ACL injuries and ACLR have increased over the last two decades, particularly among young female athletes.2–4 The consequences of an ACL injury are substantial, with most injuries being season-ending and resulting in the most missed games compared to other injuries across competition levels.5,6 Additionally, only 69-81% of athletes return to sport, with only 55% returning to a competitive level.7–9 Moreover, there is a particularly high rate of ACL re-injury, reported as high as one out of five, with a six times greater likelihood of ACL injury compared to healthy controls.10,11 An ACL injury can also result in a significant economic burden, psychological consequences, and an increased likelihood of developing knee osteoarthritis.12–16 Consequently, further investigation regarding the factors that may predispose an individual to this injury and available strategies to screen and mitigate injury risk are warranted.
ACL INJURY RISK FACTORS
Up to 75% of sports ACL injuries occur without physical contact (i.e., non-contact) with another player or object, most often during deceleration and a change of direction (COD) through a planted lower limb.1,17,18 These injuries are most prevalent in multidirectional sports that require frequent COD movements, such as soccer, basketball, lacrosse, and football.19–22 Females participating in school-aged sports have a significantly greater risk of experiencing a non-contact ACL injury when compared to males at the same age and sport.19–24 Female athletes have been reported to have an ACL injury incidence rate (IR) of 1.88 per 10,000 athletic exposures (AEs) compared to 0.87 per 10,000 AEs among male athletes across sports such as basketball, lacrosse, and soccer.22 The overall injury incidence rate ratio (IRR) for female athletes compared to males is reported to be 1.40 to 3.00.20,22,25,26 IRR is the ratio of injuries per AEs in females compared to males. Considering these findings, clinicians should evaluate why certain populations are at a greater risk of ACL injury than others and what appropriate and actionable mitigation strategies may be.
When considering what factors may be involved in this sex disparity in injury incidence, one must acknowledge that injury risk is multifactorial in nature. A review by Ruddy et al.27 highlights the complexity of team sport injuries and the need to account for multiple variables when assessing injury risk rather than a reductionist approach. This complexity is particularly true for ACL injuries, with intrinsic (non-modifiable) and extrinsic (modifiable) factors influencing injury risk. There are various intrinsic characteristics more common in females that may promote a greater predisposition to an ACL injury, including hormonal influences, intercondylar femoral notch width, anterior knee laxity, and tibial plateau slope.28,29 However, these non-modifiable risk factors offer limited opportunities for strategizing and implementing ACL injury mitigation compared to their modifiable counterparts.
Poor neuromuscular control during landing and COD movements are common modifiable contributors to ACL injury risk.1,17,30–32 Neuromuscular control is defined by Herrington et al.33 as “the ability to deliver a movement in an ‘optimal’ manner which minimizes loading stresses or maximizes the distribution of loading stresses on the tissues.” Suboptimal trunk and lower extremity movement quality during COD or landing tasks have been identified as visible characteristics of non-contact ACL injury and are determinants of potentially hazardous knee joint loads that increase ACL loading.34–39 Specifically, a dynamic knee valgus movement during deceleration or COD can pose a multiplanar load to the ACL and, when it exceeds its load capacity, result in injury.17,34,40,41 A knee abduction moment (KAM) describes the kinetic forces applied to the knee during knee valgus.32,42 Several authors have identified an increased KAM, increased hip adduction, decreased hip and knee flexion, and increased hip internal rotation in females compared to their male counterparts in both cutting and landing tasks common in sports participation, which may partially account for the greater relative ACL injury risk observed in females.35,43–49
Several studies using video analysis have identified knee valgus as a prominent movement pattern during sport-related ACL injury, with some authors reporting knee valgus during 81-88% of non-contact ACL injuries.34,36,37,50 Additionally, frontal and sagittal plane trunk positioning, lateral foot width placement, knee flexion angle, and penultimate foot contact braking have been demonstrated to significantly influence knee joint loading during COD tasks.51 These findings have also been recognized for second ACL injuries, with Paterno et al.30,31 reporting increased lower extremity neuromuscular control deficits and knee valgus during postural control and landing tasks among those going on to experience a second ACL injury compared to those who did not. Collectively, these findings suggest that specific movement characteristics and quality deficits, particularly with increased KAM, can potentially lead to increased strain on the ACL.
ASSESSING MOVEMENT QUALITY
The assessment of tasks associated with ACL injury (i.e., jump landing and changing direction) is crucial for mitigating first and subsequent ACL injuries, especially in female athletes participating in multidirectional sports. While a review by Arundale et al.52 highlights that no test can solely predict ACL injury, the utilization of movement screening may offer insight into the presence or absence of specific movement patterns associated with ACL injury, which, in theory, increases the relative risk of injury. Several strategies have been investigated and recommended to identify modifiable movement patterns associated with ACL injury risk.36,44,50,53 With better insight into movement quality, clinicians can implement targeted exercise-based knee and ACL injury prevention strategies to promote better movement control and injury risk reduction, an approach outlined by Dos’Santos et al.42 supported by strong evidence in the Exercise-Based Knee and ACL Injury Prevention Clinical Practice Guidelines.54 Furthermore, an assessment of movement quality can also serve as an important component of a testing battery when making return to sport decisions. While the use of return to sport testing has inconsistent predictive value in determining reinjury after ACLR, this finding should only bolster the need to ensure the use of comprehensive and individualized testing.55,56 Several review publications recommend assessing movement quality as part of a larger testing battery to quantify an athlete’s readiness for return to sport after ACLR.57–61
MOVEMENT ASSESSMENT METHODS
Researchers have demonstrated the use of 3-dimensional (3D) movement analysis coupled with force plate technology to assess kinetic and kinematic variables, serving as a reference standard for other measures of movement quality.53,62–65 A 3D movement analysis can allow for a thorough evaluation of an athlete’s neuromuscular control during sport-related movements, with KAM serving as a significant predictor and surrogate measure for ACL injury.32 While certainly the gold standard, utilizing 3D movement analysis requires extensive time, equipment, trained staff, and costs that are not always practical or realistic for those who are within a clinical setting working with a greater number of athletes, fewer staff, and fewer resources.32 As an alternative to 3D movement analysis, 2-dimensional (2D) video analysis has been proposed as a means of assessing movement quality. McLean et al.66 compared 2D and 3D movement assessments to screen for movements associated with ACL injury risk. Their study demonstrated strong correlations between 2D and 3D assessment of knee valgus during side-step and side-jump maneuvers. Several other authors have proposed clinic-friendly qualitative 2D video or real-time assessment tools to identify movement patterns associated with ACL injuries, including different variations of a single leg squat,67,68 the Drop Vertical Jump (DVJ),32,69 the Landing Error Scoring System (LESS),62,70 the Tuck Jump Assessment (TJA),71,72 and the Vail Sports Test.73,74
TASK SPECIFICITY
While the various 2D video and real-time assessment tools presented offer clinical utility, they are predominantly limited to assessing vertical landing or squatting mechanics. Indeed, these tasks are important and have application, particularly for screening athletes who participate in jump-landing sports such as basketball, volleyball, and netball. However, none of the included assessments focus on COD movements. This is pertinent as changing direction is biomechanically different from jump-landing, is a common movement in multidirectional sports, and directional changes are a prominent mechanism for ACL injury.17,34,37,40,41,75 Movement assessment may be task-dependent, with several studies demonstrating differences in movement quality between drop landing and COD tasks.76–78 An individual who displays sub-optimal mechanics or higher knee joint loads during landing may not necessarily display poor mechanics and higher knee joint loads during COD and vice versa.76–78 Cowley et al.79 identified that basketball and soccer players had increased knee valgus with a 45-degree COD compared to the drop vertical jump. Additionally, King et al.80 reported that biomechanical differences during sidestep maneuvers were identified nine months after ACLR in a group of 156 subjects. These findings suggest that a qualitative assessment of movement during a COD task is warranted to screen for potential first and second ACL injury risk among athletes who must replicate these movements in their sport.
Despite the evidence favoring the utilization of a qualitative 2D assessment of COD, two literature reviews reported that this is rarely assessed in clinical practice after ACLR.58,81 Burgi et al.58 suggest that assessing movement quality or other performance-based tests may be less commonly used than impairment-based measures (like strength and knee laxity) because of the potential need for equipment, large amounts of space, and lack of testing standardization. However, the authors point out that impairment-based measures may not relate as strongly to sports participation as performance-based measures. The specificity of sport-specific movement testing requires consideration, given the frequency of COD actions in multidirectional sports and the propensity to generate hazardous mechanical loads with poor movement quality.
ASSESSING CHANGE OF DIRECTION MOVEMENT QUALITY
Authors commonly use terms such as COD, agility, quickness, and cutting, often with no consistency in definition and context.82 The Essentials of Strength Training and Conditioning textbook by Haff and Triplett83 defines COD as a situation when an individual must utilize “skills and abilities needed to change movement direction, velocity, or modes.” Dos’Santos et al.84 identified several COD strategies, including a sidestep, crossover cut, split step, pivot, and shuffle step. There are also multiple means of formally assessing COD. As previously mentioned, while often the gold standard, 3D movement analysis and force plates are not always realistic in clinical settings.32 By contrast, Welling et al.85 propose various on-field tests to consider after ACLR. However, of the tests identified, only one of the proposed tests formally assesses athletes for movements that may predispose them to an ACL injury.63,64 Furthermore, work conducted by Nimphius et al.86 provides an overview of over 40 tests of non-reactive and reactive COD that can be used to assess an athlete’s performance, typically through time to completion. However, while the authors advocate using qualitative movement assessment in conjunction with quantitative performance, none of the included tests offer a formalized or objective means of doing so.
Several methods of objectively assessing 2D movement quality during a COD task have been proposed, with varying methodologies and populations. The Cutting Movement Assessment Score (CMAS),42,63,64 the Expanded Cutting Alignment Scoring Tool (E-CAST),87,88 and tests proposed by Della Villa et al.,65 Di Paolo et al.,53 and Weir et al.89 all utilize 2D video analysis to assess COD movements.89 Each assessment entails subjects performing between a 45 and 90-degree side step maneuver or a transition to a backward sprint, with movement quality later assessed using frontal and sagittal plane 2D video.
Among these 2D COD assessments, the CMAS and the E-CAST have demonstrated the most promising concurrent validity compared to 3D movement analysis, as well as inter-rater and intra-rater reliability.63,64,87,88,90–92 Additionally, these assessments can be set up and performed in a way that is feasible for clinical practice, requiring minimal equipment. As for the remaining tests by Weir et al.,89 Della Villa et al.,65 and Di Paolo et al.,53 some considerations may make their clinical utility challenging. For example, the 2D movement analysis by Weir et al.89 has fewer studies investigating its reliability and requires the use of manual measurements and digitization, which can be time-consuming. Tools proposed by Della Villa et al.93 and Di Paolo et al.53 both require more complex use of vectors through force platforms in addition to measuring 2D angles during video analysis. Thus, for the purpose of this commentary, the authors will focus on qualitative movement screening tools that require subjective evaluation of techniques and postures.
THE CUTTING MOVEMENT ASSESSMENT SCORE (CMAS)
The CMAS is a validated screening tool that utilizes a 9-item scoring rubric (Appendix 1) to assess an athlete’s movement quality during a 45-90° COD maneuver.42,63,64 A higher score in this assessment represents the presence of a greater number of movements associated with ACL injury. Each of the nine items included in the CMAS, operationally defined by Dos’Santos et al.,42 is based on technical determinants of KAM during COD movement and has been demonstrated as having a significant influence on knee joint loading associated with ACL injury.51,63,64
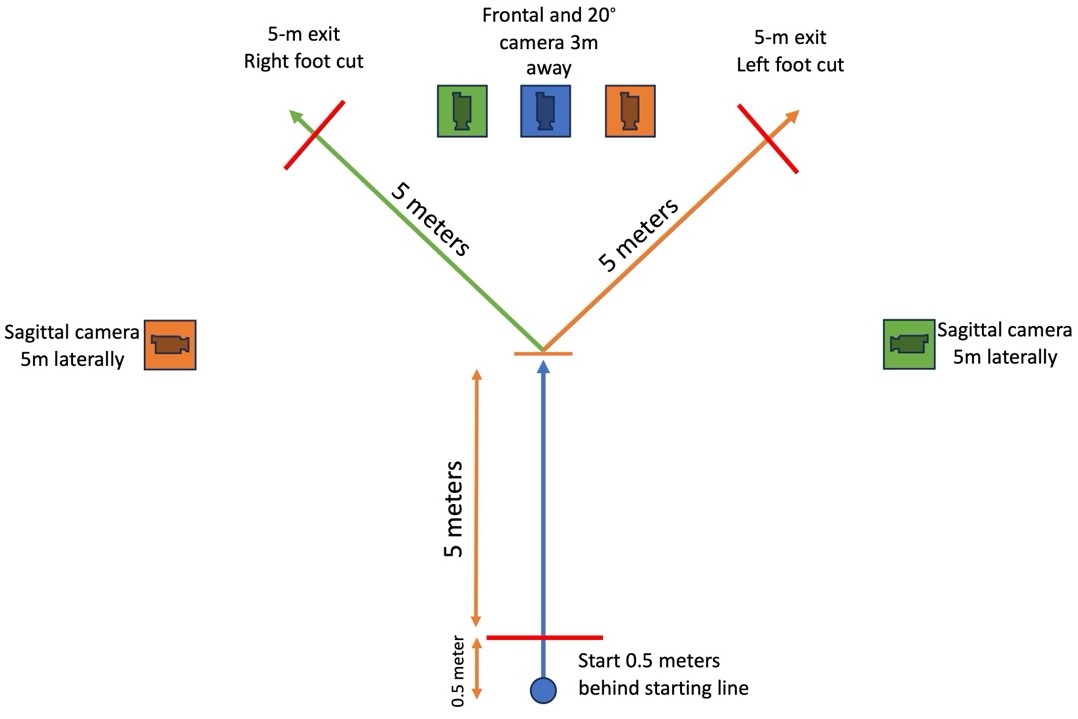
The CMAS can be performed with two high-speed cameras, cones, and the CMAS grading rubric, making it a more clinically practical tool than 3D movement analysis.42 In the testing procedure, subjects sprint 5 meters “as fast as possible” and perform a 45-90° side step cut at a designated area under video recording (Figure 1).42 Video sampling should be recorded using a minimum of two cameras capable of recording at least 100 frames per second (fps), a feature available for most smartphones and tablets.42 Dos’Santos et al.42 recommend using an additional camera 20° from the frontal plane view to reduce parallax error in subjects who pre-rotate. However, in a more recent study, Jones et al.94 identified excellent reliability for total CMAS scores with only two camera angles, as long as one included the sagittal plane view. Practitioners should evaluate 2-3 trials per limb for each athlete, with video footage ideally viewed in software that enables videos to be played at different speeds and be viewed frame-by-frame.42
_as_demonstrated_in_dos_santos_et_al.jpeg)
Several studies have reported the concurrent validity of the CMAS in identifying movements associated with ACL injury compared to 3D movement analysis.42,63,64 The overall inter-rater and intra-rater reliability of the CMAS has been moderate to excellent, with only one study by Aparicio-Sarmiento et al.95 identifying poor reliability of the CMAS. Their findings may have been confounded by insufficient training regarding the use of the CMAS.95 A study by Jones et al.94 also assessed the reliability of the CMAS using sports scientists and medical practitioners, including physical therapists. They identified good to excellent inter-rater agreements across all practitioners for total scores (K = 0.63-0.84), offering promising implications for using the CMAS across disciplines. A summary of the CMAS validity and reliability is provided in Table 1. Dos’Santos et al.42 further proposed a stratification of injury risk based on a subject’s total score: low risk is a CMAS ≤3; moderate risk is a CMAS 4-6; and high risk is a CMAS ≥7, with athletes displaying scores ≥ 7 displaying greater knee joint loads and postures associated with ACL loading compared to athletes with lower scores.
THE EXPANDED CUTTING ALIGNMENT SCORING TOOL (E-CAST)
The E-CAST is a validated screening tool that uses a 6-item dichotomous scoring rubric (Appendix 2) to assess movement quality during a 45° COD maneuver, with a higher score representing a greater number of movements associated with ACL injury.88,91 A score of “1” is awarded for each item when the movement fault is present and the total score is determined.51,87 The E-CAST is an expansion from the 4-item Cutting Alignment Scoring Tool (CAST) that originally only included a frontal plane assessment of trunk lean, cut width, and knee valgus.87 The expanded version now includes sagittal plane assessments of knee flexion angle and ankle plantar flexion.88 Butler et al.92 compared the use of the E-CAST qualitative scoring rubric against a quantitative version requiring 2D kinematic measurements and found no significant differences between the two, suggesting that either can serve as a reliable means of assessing movement quality.
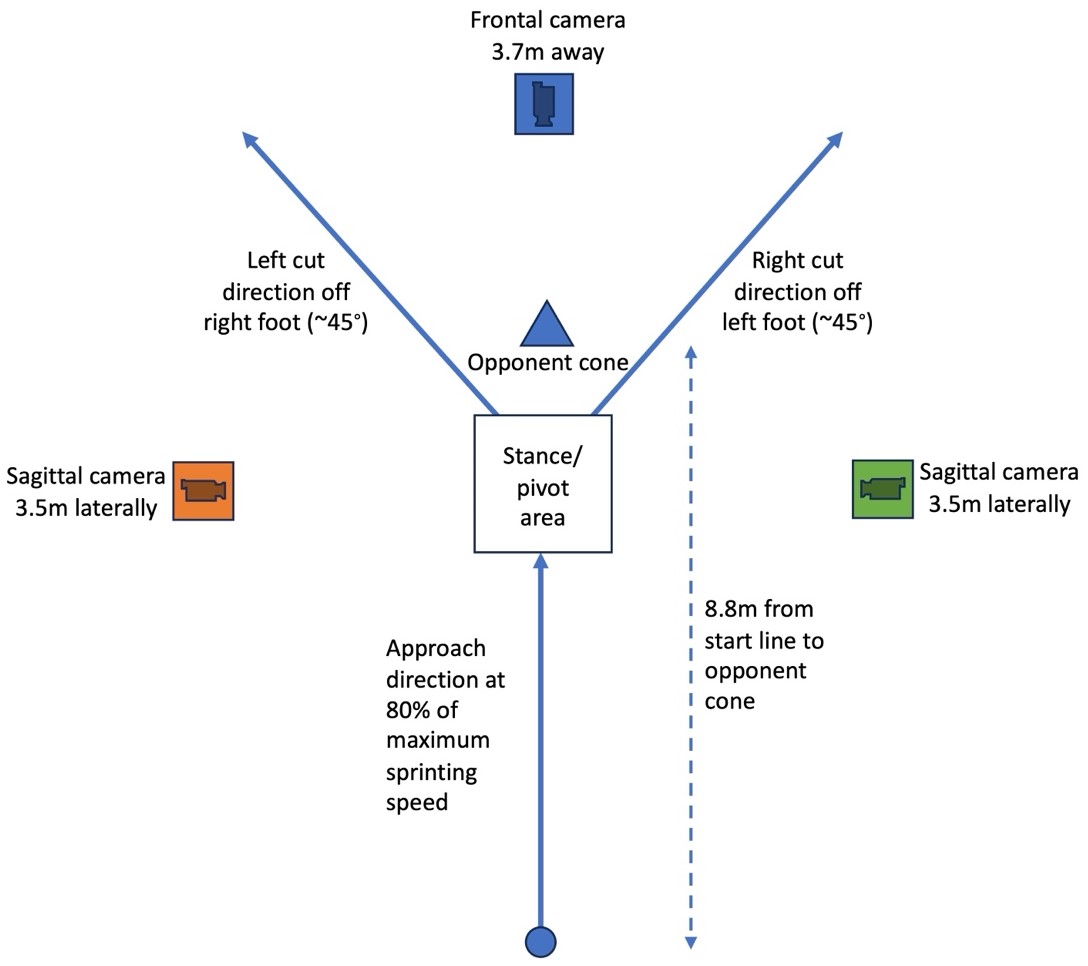
The E-CAST can be performed in a means similar to that of the CMAS using two high-speed cameras, cones, and the E-CAST grading rubric, making it more practical than 3D movement analysis.92 Subjects sprint 8.8 meters at 80% of their maximum speed towards an “opponent cone” placed just beyond the pivoting area (Figure 2). A side step cut is performed at a 45° angle under video recording.87 Previous investigations of the E-CAST recorded video at 60fps with 1080p quality that was later slowed down by 50% for video analysis.87 Subjects completed three trials per direction, with one randomly selected for analysis.87,91

Butler et al.88,92 have demonstrated the concurrent validity of the E-CAST with 3D movement analysis as well as good inter- and intra-rater reliability (ICC=0.752 and ICC=0.821).88,91 The original 4-item CAST demonstrated good inter-rater and intra-rater reliability (ICC=0.808 and ICC=0.753) among medical doctors, physical therapists, and athletic trainers.87 However, the utility of the E-CAST has only been assessed with physical therapists as the administrators and raters.88,91,92 A summary of the E-CAST validity and reliability is provided in Table 1.
The CMAS and the E-CAST can both potentially serve as a practical and insightful standardized assessment of ACL injury risk with COD movements. Given their clinic-friendly utility and objective information about COD movement quality, implementing one of these assessment tools is merited to screen for both first ACL injuries and after injury as part of a return to sport testing battery. While The CMAS and the E-CAST have similar qualities, they also carry noteworthy differences. For example, they each have a different number of items (9 vs. 6), with the CMAS including an assessment of penultimate foot contact and foot rotation, each correlated with knee joint loads.51,63,64,88 Further examples of the differences between the CMAS and the E-CAST are outlined in Table 1. Each clinician must assess the unique needs and movement characteristics of the individual athlete they are working with, their respective sport, and the set up most conducive to the clinician’s setting.
LIMITATIONS
A significant limitation of the presented 2D COD movement analysis tools is that there is currently no prospective evidence showing they can predict injury. While the evidence strongly supports the concurrent validity and reliability of the presented measures, a further direction of research should be determining their predictive validity, particularly for ACL injury. Despite mixed validity for the utilization of return to sport testing as a whole, it is still advisable to screen for movements associated with ACL injury in sport-specific movement patterns, as opposed to limiting screening to time from injury and basic clinical examination measures.58,98–102 Some investigations have suggested that COD biomechanical issues may still be present longer than strength deficits post-op ACLR and that improved movement quality during return to sport testing is associated with a decreased risk of second ACL injury.80,101
Additional limitations of the provided movement analysis tools are the potential barriers related to space, time, and cost. The CMAS requires an open space that is roughly 8x10 meters, with the E-CAST requiring roughly 13x7 meters. Many clinicians may not have access to an open area this size if they are limited to a small office already filled with treatment tables and equipment. Also, performing all the required practice trials and valid trials does take time, an indispensable resource in clinical practice. However, Dos’Santos et al.42 have reported completing six CMAS trials in groups of athletes as large as twelve in less than 15 minutes. This suggests that, with experience, testing can be completed in a reasonable time. Lastly, clinicians must consider equipment costs. Utilizing timing gates and high-end cameras comes at a significant economic cost that may not be attainable for practitioners. Fortunately, the test setup can be completed with cones and with the use of any recording device capable of recording at a higher frame rate, a feature available on all iPad and iPhone devices. When considering these limitations, not all clinics may be capable of conducting these tests. Patients may need to be referred to specific testing sites with the appropriate space and equipment, in line with recommendations by Unverzagt et al.59
CONSIDERING ADDITIONAL VARIABLES
Marques et al.103 offer insight into the application of COD movement assessment after ACLR. In their review, they do not emphasize a specific tool such as the CMAS or E-CAST, but they do identify key variables to consider when utilizing field and laboratory-based COD testing, such as planned vs. unplanned, approach velocity, and cutting angle.
Planned vs. Unplanned Movement
An additional consideration for the assessment of COD movement quality should be whether the COD is planned or unplanned. Sports participation often requires an athlete to process multiple sources of information and stimuli when executing sporting actions. In the context of COD, athletes often need to respond to an external stimulus, such as an opponent or a ball, that requires externally directed attention.104 Several researchers have suggested that this external focus on unplanned stimuli increases neurocognitive loads, presenting a particular after ACL injury given changes in neuroplasticity and neurocognitive compensation.104–108 Sheppard et al.82 propose that “In order to be considered ‘reactive’ agility, the movement should not only involve a change in speed and direction, but must also be an open skilled task, involving a reaction to a stimulus.”
The performance of COD tasks under reactive conditions has been proposed as a uniquely different task compared to pre-planned COD, entailing different cognitive challenges in response to spatial and temporal stimuli.82,109,110 Unplanned COD may be more representative of sports participation, given the requirements in team sports to respond to an external stimulus, such as an opponent or ball, without pre-planning. Without a reactive element, movement assessment tools only replicate a portion of the conditions and scenarios common in sports and ACL injuries. While most ACL injuries are non-contact, the majority occur with externally directed attention and increased neurocognitive loading, typically with an opponent or ball.36,50 Several authors have described that knee movement mechanics and timed performance differ in unplanned and planned movements.111–115 Specifically, increased KAM and internal rotation moments have been identified at the knee under unplanned conditions compared to planned conditions, both associated with increased risk of ACL injury.111,113,116 Moreover, the 2016 Consensus on Return to Sport and additional authors have suggested that utilizing unplanned movements may be superior to incorporate over planned tasks alone.57–60 Separate reviews by Grooms et al.108 and Wilk et al.60 recommend utilizing neurocognitive and reactive testing to assess return to sport readiness after ACLR. The combined recommendations of these authors suggest that the formal assessment of movement quality under unplanned movements is warranted. However, while unplanned COD may hold many benefits, there are challenges with producing a valid, standardized sport-specific stimulus that has good reliability.
A study by Needham and Herrington90 investigated differences in CMASs between planned and unplanned sidestep maneuvers for female soccer players. They identified significantly greater total CMASs for unplanned COD maneuvers (5.53±0.71) compared to planned maneuvers (3.55±0.85, p<0.012). The findings of this study match previous results that unplanned movements may reveal a higher number of movement patterns associated with ACL injury risk.111,113 This study suggests that a 2D COD movement assessment tool can offer utility in assessing both planned and unplanned conditions and that only assessing planned conditions may not wholly represent an athlete’s injury-risk profile.
There are noteworthy challenges with the implementation of unplanned movement assessment. There is often a tradeoff between ecological validity and standardization when selecting a stimulus for unplanned movement. In the study by Needham and Herrington,90 a soccer ball pass was used to cue the subjects in their cutting direction. Their approach may promote greater ecological validity compared to light or sound-based stimuli. However, as acknowledged by Needham and Herrington,90 this approach does carry limitations in its consistency of timing and trajectory, thus potentially influencing subsequent reaction times and movement patterns. By contrast, the utilization of light stimuli is easier to regulate but is lacking in sport specificity. Additionally, caution and a stepwise progression must be utilized when integrating unplanned COD maneuvers given the potential for increased knee joint loads, particularly in the context of return to sport testing after injury.
Approach Velocity
One additional variable that is pertinent in the assessment of COD is the velocity at which the individual enters into the COD task (i.e., approach velocity). Reviews by Marques et al.103 and Dos’Santos et al.117 highlight that approach velocity significantly influences COD speed and biomechanics. Kristianslund et al.118 demonstrated that increased KAMs are seen with higher approach velocities compared to lower velocities among female athletes during COD maneuvers. Further studies have found that when subjects performed COD maneuvers with higher approach velocities, they exhibited greater knee joint stiffness and peak knee valgus.119–121 An investigation on injury mechanisms for ACL injuries in handball by Olsen et al.34 also identified that non-contact ACL injuries commonly occurred at high approach velocities during COD tasks. When considering this in practical application, approach velocity should be considered when assessing movement quality, as those moving at faster speeds may be more likely to exhibit more potentially hazardous movement mechanics.103,117 As a potential means of mitigating injury and improving standardization in movement assessment, Vanrenterghem et al.121 suggest that velocity should be standardized to 4 meters per second.
Cutting Angle
Both Dos’Santos et al.117 and Marques et al.103 highlight that cutting angle is also a pertinent consideration when assessing COD movement quality. These authors identify that sharper COD angles (90 vs 45°) result in increases in knee joint loading and require lower approach velocities for optimal execution (i.e., COM angle deflection). Dos’Santos et al.117 identifies this as the “angle-velocity trade-off,” whereby faster approach velocities can compromise the COD execution. Given the established correlation between approach velocity and COD movement quality, it must be accounted for as a variable for execution performance and should be considered when screening COD movement quality.
OPPORTUNITIES FOR INTERVENTION
The clinical assessment of COD movement quality to determine ACL injury risk would be limited in value if there were no opportunities for measurable improvement. Fortunately, COD movement quality has been shown to be modifiable. Clinicians should first utilize a cutting assessment tool to identify movement patterns associated with increased injury risk. While this may have standalone value in making return to sport decisions, clinicians should also use their findings to formulate impairment-based neuromuscular interventions to address underlying movement patterns. For example, testing results may indicate movement deficits related to poor trunk control, increased knee valgus, or a lack of knee flexion. Interventions aimed at improving muscle strength and neuromuscular control can be prescribed to mitigate the identified movement patterns.
Neuromuscular training has been demonstrated to improve proprioception and decrease biomechanical deficits.122,123 These strategies can vary considerably but generally include unilateral and bilateral lower limb and core exercises with visual, verbal, and/or tactile feedback to improve trunk and knee control.122,123 This approach can be integrated through foundational exercises, plyometrics, and cutting maneuvers. A review by Buckthorpe124 provides recommendations for a movement retraining progression after ACLR, beginning with foundational movement training, then progressing to high-load ‘sport-type’ movement retraining, and lastly, integrating sport-specific movement retraining.
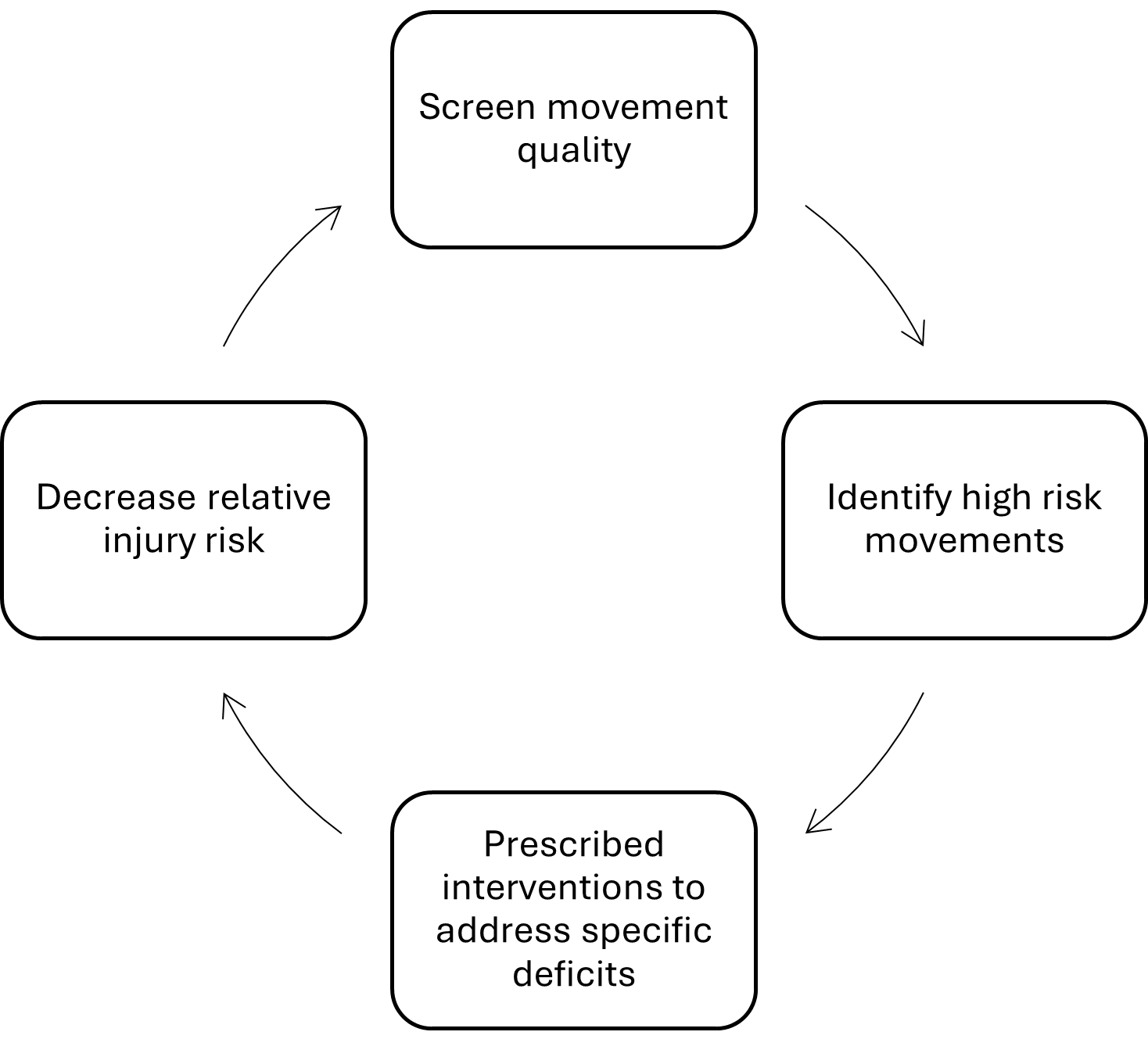
Studies by Olivares-Jabalera et al.125 and Dos’Santos et al.126 investigated the effectiveness of separate six-week technique modification programs to improve cutting and jump-landing movement quality among soccer players. Both studies identified significant pre-to-post improvements in CMAS scores after six weeks of COD movement training with individualized feedback from a practitioner. Additionally, a study by Nijmeijer et al.127 identified improvements in CMAS scores when subjects were provided video and verbal feedback, particularly when they were given autonomy to select the timing in which they received it. These findings indicate that COD movement quality can be improved with task-specific training. Additionally, movement assessment can serve as a valuable test-re-test measure to track modifiable risk factors associated with ACL injury risk. Dos’Santos et al.128 describe this process for movement assessment, treatment, and reassessment, depicted in Figure 3. This process can be completed multiple times over the course of an individual’s episode of care or season to track patient improvement and reduce injury risk.

SUMMARY
ACL injuries are formidable and consequential injuries in athletics that are influenced by considerable intrinsic and extrinsic risk factors.5,6,12–16 Of these risk factors, an individual’s movement quality has been demonstrated as a significant variable associated with ACL injury risk, particularly among female athletes in multidirectional sports.1,17,19–23,26,30–32 While there are various means of assessing movement quality, an assessment during a COD maneuver provides task-specific insight that is a prevalent mechanism of ACL injury.76–78 The CMAS and the E-CAST both provide valid, reliable, and objective means of assessing movement quality during COD tasks worth considering when screening for ACL injury and re-injury risk.42,63,64,88,91,92,94 Additionally, variables such as planned and unplanned movement, approach velocity, and cutting angle should all be considered as pertinent influences on task performance and injury risk and must be considered when screening and profiling movement quality.82,103–110,117
Conflicts of interest
The authors report no conflicts of interest.