INTRODUCTION
Isometric strength testing is used extensively in sport and healthcare settings to test a participant’s physical capabilities during clinical decision-making processes.1,2 As hamstring strain injuries are one of the most prevalent injuries in sports that require high-speed running3,4 measurements of maximal isometric knee flexion are important to assess for hamstring dysfunction. This measure can be used to highlight muscle imbalances between limbs,5 as well as monitor for risk of re-injury.6 Having highly reliable and repeatable measures to work with is important to justify return to play decisions that practitioners are required to make, as well as guide progression through rehabilitation protocols.
A plethora of different dynamometry devices are available on the market which are often selected according to ease of use, cost, and portability.7,8 Isokinetic dynamometry (IKD) is currently suggested to be the “gold standard” measurement of strength in research and clinical practice,9 however, this equipment is not portable, which may limit its use in certain field-based settings. To address this potential issue, portable fixed-framed dynamometry systems have recently come to market. Kangatech (KT360) (KangaTech Ltd, Melbourne, Victoria, Australia) is a portable fixed-frame dynamometry system that utilizes a stainless-steel frame with detachable dynamometers and can be positioned to assess varied muscle groups across different planes of motion.10 The system has a multitude of standardized protocols to measure the isometric strength in different fixed positions. Because the KT360 system is a novel device, there is a paucity of evidence surrounding its reliability as has been established for other portable or fixed frame dynamometry measurement tools.11 A recent study evaluated the test-retest reliability of the KT360 system prior to the addition of a 360° rotational frame.10 This study found that Interclass correlation coefficient (ICC) for left knee flexion was 0.927 and 0.923 for right knee flexion. More recently, high test-retest reliability (ICC 0.895-0.974) was found in hip adductor strength with standard error of measure (SEM) and minimal detectable change (MDC) % ranging from 0.59-2.25 and 1.63-6.26, respectively.10 While this provides some initial reliability estimates for the portable fixed frame system, there are currently no studies available estimating the reliability since the 360° rotational frame was released into the market, and none that have considered the testing protocol of 90° hip and knee flexion. Furthermore, there are currently no studies that have estimated the inter-rater reliability of the equipment. As the pressure of keeping athletes in play and delivering results continues to increase within sporting environments, sports teams have a strong economic incentive to invest in injury prevention and rehabilitation.12 Having reliability estimates will help develop practitioners to make an informed decision on whether to integrate such equipment into multidisciplinary sports science and medical departments.
It was hypothesised that the KT360 system would demonstrate a high threshold of reliability when measuring maximal strength produced during the isometric knee flexion protocol based on the results of previous literature.10,11 The aim of this study was to determine the inter-and intra-rater reliability of the KT360 fixed frame dynamometry system when measuring maximal isometric strength of the knee flexor muscles.
MATERIALS AND METHODS
A cross-sectional study design was used. Ethical approval was granted by the School of Health Ethics committee at Leeds Beckett University (ethics number: 98113) and complied with the Declaration of Helsinki on Human Research international standards.
Participants
Healthy, university level athletes were recruited to take part in the study using a convenience sampling method. All participants had to be over the age of 18, have membership with University Athletic Union, train >2 times a week, and regularly take part in sporting competitions. Participants were excluded from the study if they had any current or recent lower limb injury (within the prior six months), had induced caffeine sixty minutes prior to any measurements being taken, had completed strenuous exercise forty-eight hours prior to the day of testing, or did not score a pass on the health screening questionnaire as recommended in previous research.13 Prior to the commencement of the study, participants were provided with a participant information sheet which fully explained the study process. All participants were required to complete a study consent form.
Procedure
Both raters were present for all testing days. Prior to the commencement of the study, both raters had undertaken two days of familiarization and training with the KT360 equipment from an experienced user who had undergone training from the manufacturer. To prevent bias, a method of simple randomization by flipping a coin was implemented to select which rater began the testing process. A computerized random number generator (using Microsoft random number generator software) picked the order in which measurements were taken for each participant.
Prior to strength measurements, demographic and anthropometric data was collected. Body mass was measured using an electronic scale (SECAAlpha770, Birmingham, UK) to the nearest 0.1kg, pre-calibrated with a 5Kg dumbbell. Height was measured using a stadiometer (SECA Alpha, Birmingham, UK) to the nearest 0.1 cm. Limb length measurements were then collected and inputted into the KT360 system. Left and right leg length was measured laying in a supine position, by measuring from the anterior -superior-iliac spine (ASIS) to the medial malleolus.14 Fibular length was measured from the apex of the head of the fibula to the apex of the lateral malleolus while laying supine.15 Participants were identified by a numerical value to ensure anonymity.
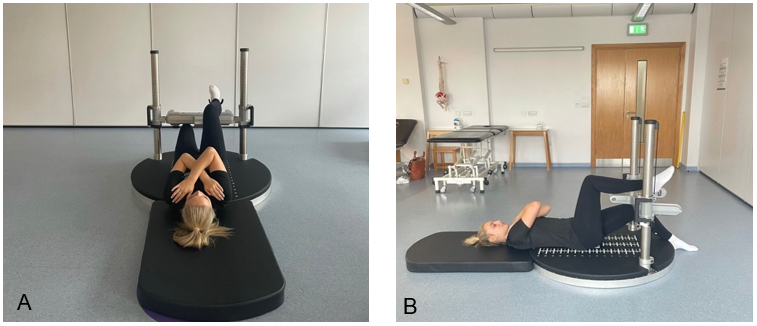
A standardized warm-up was then completed. This consisted of a 15-minute stationary cycle (40% VO2 max), followed by 3 sets of 10 reps bodyweight squats and 2 sets of 8 reps of isometric hamstring curls (90° hip, 90° knee; 50% 1RM load), holding the contraction in mid-range for 5 seconds using the KT360 pads to meet the participants resistance.16 The participants knee flexion was then tested in both the right and left limbs. This was measured in supine with arms across the chest, aligned pelvis, and neutral knee position, with knees over toes. The leg being tested was placed at 90° of hip and knee flexion measured with a goniometer and positioned so the ankle of the cuff was aligned with the lateral malleolus, the housing was rotated so the cuff was flush with the achilles tendon, this angle was noted for the re-test. The resting foot was flat with the heel pressed against the base of the platform. Images of the testing position is shown in Figure 1. The test was performed at 90° knee flexion as previous studies including Electromyography (EMG) measurements indicate that maximum hamstrings EMG amplitude is achieved in the mid-range knee flexion angle.17The 90° hip flexion angle is associated with producing optimal range for force production through the knee joint.18 In this position, the knee flexors are not fully elongated or contracted, enabling the muscles to produce peak torque.18

Each participant had a familiarization repetition where they sustained a five second contraction at 50% effort, followed by 30 second rest. The knee flexors were tested twice with the participant accelerating into a maximal isometric contraction as quickly as possible and then maintaining for a five second period with a 30 second rest between tests.11 The rater not collecting the data was blinded to the results by waiting outside the testing room. The resting period between the second test for Rater 1 and the single test for Rater 2 was five minutes as previous studies have suggested that this is sufficient time to facilitate recovery between tests.19
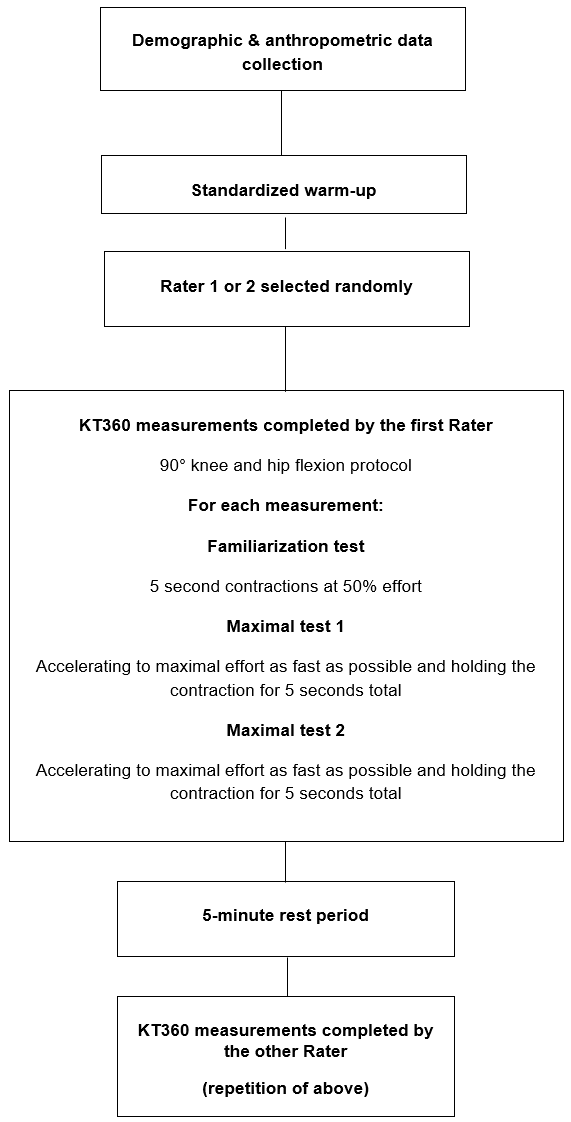
Motivational cues given by both raters during testing included ‘push’ to maximal effort as soon as possible straight after the ‘3, 2, 1 Go’ visual display on the KT360 tablet. This verbal encouragement has been suggested in previous research to increase motivation to encourage subjects to exert maximal strength.20 A standardized script of instructions to explain the protocol was used to ensure consistency within and between raters. A schematic of the study testing procedure can be found in Figure 2.

Data analysis
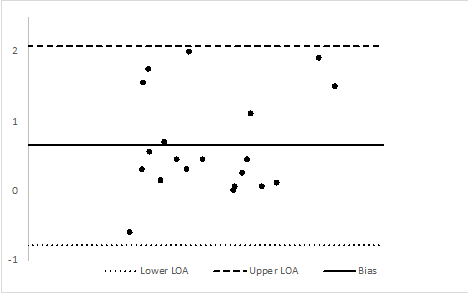
Data were transferred to Microsoft Excel, (Microsoft Corp, Redmond, WA, USA) and statistical analysis was conducted using SPSS version 27. The distribution of data was assessed for normality using the Shapiro-Wilk test. The intraclass correlation coefficient (ICC) was used for the analysis of relative reliability.21 The type of ICC model used for this was the two-way design as multiple raters obtained measures of each participant.22 Interpretations of the results were as follows: a <0.1= trivial; >0.1 to 0.3= small; >0.3 to 0.5= moderate: >0.5 to 0.7= large; >0.7 to 0.9= very large; and >0.9 to 1.0,= almost perfect.23 Standard error of measurement (SEM) was calculated using the following equation: standard deviation (sd)*(√1-ICC), the SEM% was: (SEM/mean)*100.11 The minimal detectable change (MDC) was calculated using the formula: 1.96*√2*SEM.11 Finally, Bland-Altman analyses were used to determine the levels of agreement for intra-and inter-rater measurements.23 The difference of the two paired measurements was plotted against the mean of the two measurements. The limits of agreement were calculated as follows: Lower Limit, mean difference – (1.96 x standard deviation of difference); Upper Limit, mean of difference + (1.96 x standard deviation of difference). Data was interpreted as recommended by previous research19 whereby 95% of the data points should lie within ±2SD (2 standard deviations) of the mean difference.
RESULTS
A total of twenty (n=20) participants completed the study (age= 21.65 ± 3 years, weight= 74.465 ± 30kg, height= 170.1 ± 7.0cm).
Intra-rater reliability
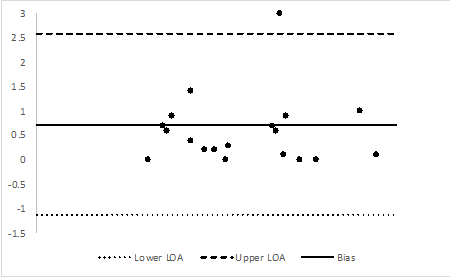
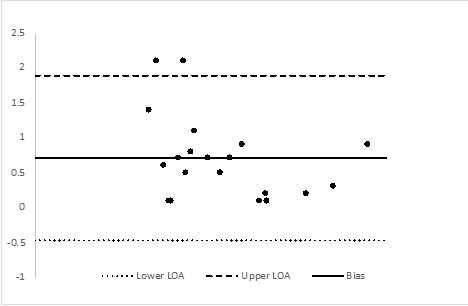
The ICC for the data was ‘almost perfect’ between all measurements. Table 1 presents the ICC, SEM, SEM%, and MDC values. Figure 3 displays a Bland-Altman analysis. Bilateral levels of agreement were found to be +/- 2 standard deviations (SD) of the interval of agreement bilaterally for knee flexion. Levels of agreement (LOA) and bias are as follows, left knee flexion: upper 2.596, lower -1.136, bias: 0.73; right knee flexion: upper 1.881, lower: -0.471, bias: 0.705.
Inter-rater reliability
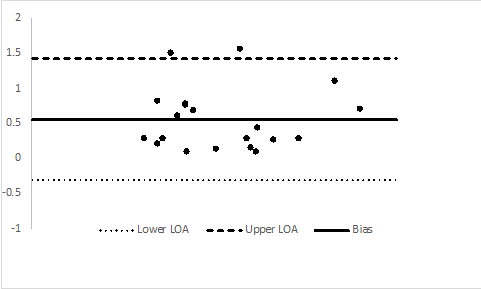
The ICC values were all ‘almost perfect’ between Rater 1 and Rater 2. The results are shown in table 1. Figures 3-6 show the results of the Bland Altman analyses. Bilateral levels of agreement were found to be +/- 2 standard deviations (SD) of the interval of agreement bilaterally for knee flexion. Levels of agreement (LOA) and bias are as follows left knee flexion: upper 2.080, lower -0.780, bias: 0.65; right knee flexion: upper 1.410, lower: -0.325, bias: 0.542.




DISCUSSION
The aim of the study was to evaluate the intra-rater and inter-rater reliability of the KT360 dynamometry system when measuring the maximal isometric strength of the knee flexors. The ICC analysis shows principal findings that data collected on two occasions by the same rater and by two different raters had values between 0.98-0.99 on interclass correlational analysis. The SEM, SEM%, and MDC values ranged from 0.45-0.69 kg, 1.72-2.71%, and 1.87-2.31kg, respectively. High levels of agreement for inter-rater and intra-rater reliability were demonstrated in all measurements, with 95% of the differences shown to be less than two standard deviations away from the mean.
Prior to the commencement of this study, it was hypothesised that reliability would be high, as previous studies using the KangaTech system prior to the addition of a 360° had yielded excellent test-retest reliability when measuring isometric hip and knee flexor strength.10,11 Prior researchers have suggested that the original KangaTech model had very high reliability for left and right knee flexion (ICC 0.92),11 which is in line with the present study where ICC values of 0.99 were recorded in both left and right limbs. Further research comparing the reliability of the KT360 when testing in different positions such as those used in these previous studies10,11 (prone with 30° and 45° hip and knee flexion with a foam roller under the pelvis and 90° hip and knee flexion) would also be a welcome addition to the KT360 literature.
Previously, researchers have considered handheld dynamometry (HHD) as a portable and low-cost alternative to estimate maximal isometric strength.24,25 The efficacy of using HHD at joints such as the knee where larger forces can be produced has been questioned,26 although implementing best-practice techniques such as external stabilization when using HHD has been shown demonstrate acceptable reliability.24 Researchers measured the inter-rater and intra-rater reliability of maximal isometric knee flexion at a 90° hip and knee position in both seated and prone positions with clinician stabilization, using the Hoggan MircroFET2 HHD.26 The authors reported ICC values of 0.92 (0.75-0.97) and 0.89 (0.69-0.96) for the seated protocol and 0.90 (0.76-0.96) and 0.94 (0.82-0.98) for the prone protocol.26 The MDC values were for the seated protocol were 27.3N (2.78kg) and 29.4N (2.99kg) and for the prone protocol were 24.3N (2.47kg) and 22.7N (2.31kg). In the present study, ICC values of 0.99 (0.98-0.99) were reported for both inter- and intra-rater data, showing that when comparing both studies, the KT360 produces higher relative reliability for both inter-rater and intra-rater reliability. Furthermore, the present study reported MDC values of 2.13-2.31kg and 1.87-2.10kg, indicating that the fixed-frame device produces a smaller amount of measurement error compared to a HHD system. Future studies are needed to directly compare the level of agreement between KT360 and HHD in a range of muscle groups and testing positions.
Isokinetic dynamometry (IKD) is suggested to be the gold standard measurement of strength within sports science and clinical practice.9 When comparing results from the present study and previous studies that have measured isometric knee flexion strength with other dynamometry devices, the KT360 device shows higher values. ICC values for intra-rater reliability of isometric knee flexor strength using the Cybex II IKD was 0.93 compared to 0.92 when measured with the ‘BTE technologies’, a portable fixed frame dynamometer.27 This highlights that the ICC values were 0.06 and 0.1 higher when using the KT360 compared to the IKD and 0.07 and 0.03 compared to ‘BTE technologies’ dynamometer used in the study.27 This shows that the KT360 is a reliable tool for measuring the strength of knee flexors and is comparable to IKD devices. Further research evaluating the level of agreement between the KT360 to IKD at a fixed angle on the same subjects would provide further evidence regarding validity regarding whether the different types of equipment could be used interchangeably in sporting and healthcare settings.
Despite this study representing reliable results of high absolute agreement, inter-rater and intra-rater reliability, limitations require highlighting. The 90° hip and knee protocol was selected from the variety of standardized protocols available on the KT360 system. Although specific joint angles were chosen in relation to previous research suggesting these testing positions serve to achieve peak torque,13,28 some hip extension movement may have occurred during testing due to the nature of the maximal contraction of the hip flexors, which may affect the results found in the study. Attempts were made to mitigate this with verbal cues and familiarization. However, further research using this protocol with an additional fixation around the hips and trunk would be required to discover if this did influence the data collected in the present study. Furthermore, the sample utilized was a convenience sample of healthy university level athletes between the ages of 19-23. Therefore, data may not be extrapolated to non-sporting or injured populations. Further investigations are required to determine if equivalent findings exist in different age groups or populations.
CONCLUSIONS
Almost perfect inter-and intra-rater reliability was demonstrated when testing isometric knee flexion with the KT360 as well as low SEM, SEM%, and MDC values. This suggests that the protocol used in the study is worthy of consideration when repeat measurements of isometric knee flexion are required in non-elite sports populations.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Conflict of interest
The authors declare that they have no conflicts of interest.
Funding statement
This research did not receive any specific funding. However, the research was performed as part of the authors employment and/or academic qualification at Leeds Beckett University.