INTRODUCTION
The hamstring strain injury (HSI) is a major concern in high-speed running-based sports. In football (soccer), for instance, a review including thirteen studies and 3,868 players with two million sport exposure hours demonstrated that HSI accounted from 4% to 13% of all injuries.1 Despite the advances in injury prevention by the scientific community over the last few decades, elite football teams have been unsuccessful in significantly reducing the incidence of HSI.2 This results in significant setbacks for both the teams’ performance and the financial health of the clubs.3 It is also noteworthy that around one in every five injured players experience a HSI recurrency, with more than two-thirds occurring within the initial two months of returning to sport.2 This underscores the importance of refining processes within injury rehabilitation and return-to-play stages, including the implementation of reliable measures for assessing hamstring function.
Diminished muscle strength has historically been considered a potential risk factor for HSI.4 Prospective cohort studies conducted in various sports have yielded inconsistent results,5 possibly because they correlate in-season injuries with muscular strength measured at a single point during the preseason.6 Despite the uncertainties provided by scientific literature, chief medical officers of elite football clubs recognize muscle strength-related deficits as playing a pivotal role in HSI,7 and hamstring strength assessments have been widely used to screen athletes with a higher injury risk.8 These assessments have also been esteemed in the context of HSI rehabilitation, with clinical practice guides recommending their utilization in decision-making regarding the patients’ progression.9 In addition, strength tests are the most common return-to-play criteria adopted following a HSI in elite athletes.10 Therefore, strength assessments have become a routine practice for prevention and rehabilitation of HSI.
Hamstring strength has been assessed through isokinetic dynamometry or specialized devices (e.g., Nordic curl test), as well as isometrically using handheld dynamometers and load cells. However, the expense associated with such equipment is a hindrance for professionals dealing with athletes at potential risk or in rehabilitation following an HSI. The Single Leg Bridge Test (SLBT) emerged as a portable and cost-effective option for assessing hamstring function in both the clinical setting and the field of play. Briefly, this test involves performing a unilateral bridge exercise with the tested leg supported on a 60 cm-high platform until the task failure (more details in the Methods section). The SLBT reliability enable its use in the sport context, with intratester intraclass correlation coefficient (ICC) values of 0.77–0.89 and intertester ICC values of 0.89–0.91.11 Furthermore, this test gained prominence since Freckleton et al.12 found that Australian football players who experienced in-season HSI exhibited lower preseason SLBT scores. From there, studies have used the SLBT to assess hamstring function in healthy subjects,13–15 as well as to help clinicians in decision-making on the athletes’ rehabilitation progress and return to sport following HSI.16,17
It is noteworthy that recent evidence does not support the SLBT as a valid tool for assessing the hamstring’s maximum strength.18–20 Gasparin et al.18 were the first to document a lack of correlation between the SLBT score and hamstring concentric or eccentric isokinetic peak torques. This observation was echoed by Robaina et al.19 and Murakami et al.20 in their respective studies involving isometric and eccentric maximum strength tests. Thus, there is compelling evidence against the use of the SLBT as a surrogate for assessing maximum strength of the hamstring muscle group. Conversely, the SLBT has often been advocated as a measure of ‘hamstring endurance’.12,14,15 It seems plausible that muscular endurance (i.e., the ability to resist fatigue) is the dominant factor due to the nature of repetitions to failure in the SLBT. However, the relationship between the SLBT score and hamstring endurance is still unknown. Therefore, the primary objective of the present study was to examine the correlation between the SLBT score and isolated hamstring endurance in healthy men. Secondly, this study aimed to examine the correlation between limb symmetry index (LSI) provided by the SLBT and hamstring endurance test results.
MATERIALS AND METHODS
Study Design
In this cross-sectional study, volunteers were evaluated at the research laboratory on two separate occasions, with a minimum interval of 48 hours between visits. During each visit, participants carried out either the SLBT or the hamstring endurance test on the isokinetic dynamometer. The sequence of assessments was randomized. A single evaluator conducted all SLBT sessions while another conducted all isokinetic test sessions. Evaluators were blinded to the results of the test conducted by their colleague. This study was approved by the Federal University of Health Sciences of Porto Alegre ethics committee (#5.589.245) and all volunteers provided informed consent before starting study participation.
Participants
Volunteers were recruited through advertisements on social networks linked to the university community. To be included in this study, the volunteers had to meet the following criteria: male subjects, aged between 18 and 35 years, who regularly participated in individual or team sports, or engaged in resistance training, with at least three sessions per week. Volunteers with history of knee or hip surgery, musculoskeletal injuries in the lower limbs in the three months prior to data collection (including hamstring strain injury), or any contraindications to perform maximal strength tests and/or muscular endurance tests (e.g., heart failure, arterial hypertension, and physical disability of the lower limbs) were not included.
Procedures
Participants were asked to avoid vigorous exercise 24 hours prior to tests and not to use analgesics and/or anti-inflammatory drugs 48 hours before the procedures. They were also instructed not to consume stimulant substances (e.g., caffeine) on testing days. Data collection sessions began with a standardized warm-up protocol, consisting of a five-minute exercise on a cycle ergometer at a cadence of 60 to 80 rpm and a self-selected load corresponding to moderate intensity. During the warm-up, participants received instructions about the tests, and all their questions were addressed. A minimum rest period of five minutes was provided between tests for each limb. The second limb was assessed only after the participant confirmed full recovery from the previous tests and indicated readiness to exert a new maximal effort.
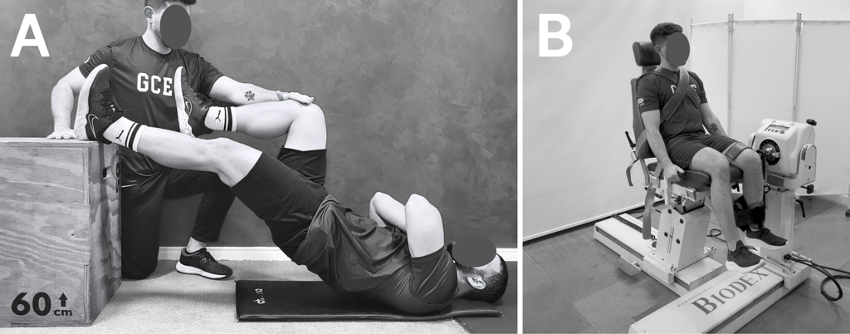
Single Leg Bridge Test (SLBT): The SLBT (Figure 1-A) was conducted in accordance with the protocol described by Freckleton et al.12 After the standardized warm-up, participants were instructed to lie down on the ground, placing the heel of the limb being tested on a 60 cm high box. Employing a goniometer, the limb being tested was set to an approximate 20° knee flexion angle. Participants were directed to fold their arms across their chest and press the tested side heel on the top of the box, lifting their pelvis off the ground until their hip reached a fully extended position at 0°. A practice repetition was performed to familiarize participants with the proper execution and to establish the target height for the upward movement. This target height was measured using a one-meter scale and used for both limbs. During the SLBT execution, repetitions were considered valid if the volunteer performed the upright movement until the contact between their non-tested knee and the rater’s hand, positioned at the predetermined target height. Thereafter, they had to touch their buttocks to the ground with no noticeable pause before the next repetition. Additionally, the contralateral thigh was kept as perpendicular to the ground as possible to prevent any momentum from swinging. If the correct form was compromised, a warning was issued, and the test was finished at the next fault. Participants were encouraged to perform as many repetitions as possible until failure.
_and_positioning_adopted_for_the_hamstring_endurance_t.png)
Hamstring endurance test: The isolated hamstring endurance was evaluated using an isokinetic dynamometer (Biodex System 4; Biodex Medical System, Shirley, NY). After the standardized warm-up, participants were positioned on the isokinetic dynamometer in accordance with the manufacturer’s guidelines (Figure 1-B). Considering the inevitable involvement of gluteal muscles in hip extension movements, the isolated hamstring endurance was tested through a maximum-intensity protocol of repeated knee flexion actions.21,22 For specific familiarization, the volunteer performed 10 submaximal concentric knee flexion-extension repetitions at an angular velocity of 120°/s throughout a 90° range of motion. Following a one-minute rest interval, participants completed the hamstring endurance test, which involved 30 concentric knee flexion repetitions performed at maximum intensity, with an angular velocity of 120°/s and a range of motion of 90°. After each repetition, the participant actively returned to the starting position (knee extended) using low-intensity quadriceps contractions. Throughout the test, participants were encouraged to exert their maximal strength from the first to the last repetition.
Outcomes
The ‘SLBT score’ was documented as the number of valid repetitions executed in each limb during the SLBT execution. The isolated hamstring endurance was assessed through two variables provided by the isokinetic dynamometry: peak torque and work. The ‘peak torque fatigue index’ was determined as the percentage reduction in peak torque along the endurance test. It was calculated by dividing the mean peak torque value obtained from the final five repetitions by the mean peak torque value from the initial five repetitions. The ‘work fatigue index’ was calculated as the percentage decline in work along the endurance test. It involved dividing the work executed during the last third (i.e., final 10 repetitions) by the work performed during the first third (i.e., initial 10 repetitions) of the endurance test. For both SLBT and hamstring endurance test, the LSI was calculated using the following equation: (left limb / right limb) x 100.
Statistical Analysis
Descriptive statistics was used to describe the participants’ performance through mean, standard deviation (SD), 95% confidence intervals (CI), and minimum and maximum values. The Shapiro-Wilk normality test was used to analyze the distribution. Correlations between SBLT scores and isokinetic fatigue indexes were assessed through Pearson’s and Spearman’s correlation coefficients for normal and non-normal data, respectively. A similar statistical approach was used to assess correlation between the LSI found in the SLBT and the hamstring endurance test. The following correlation criteria were adopted: 0.69 or less, poor correlation; 0.70 to 0.79, fair correlation; 0.80 to 0.89, good correlation; and 0.90 to 1.0, excellent correlation. Statistical significance was set at 5% (p<0.05).
RESULTS
Forty healthy, physically active men (mean age: 25 ± 2 years, mean weight: 83 ± 8 kg, mean height: 176 ± 1 cm) participated in this study, resulting in a total of 80 limbs evaluated. Fifteen participants were recreational athletes of a range of sports: running (n=6), soccer (n=2), crossfit (n=1), volleyball (n=1), basketball (n=3), Olympic weightlifting (n=1) and sport climbing (n=1). Some of these recreational athletes routinely practiced more than one sport. The other 25 volunteers were only engaged in resistance training.
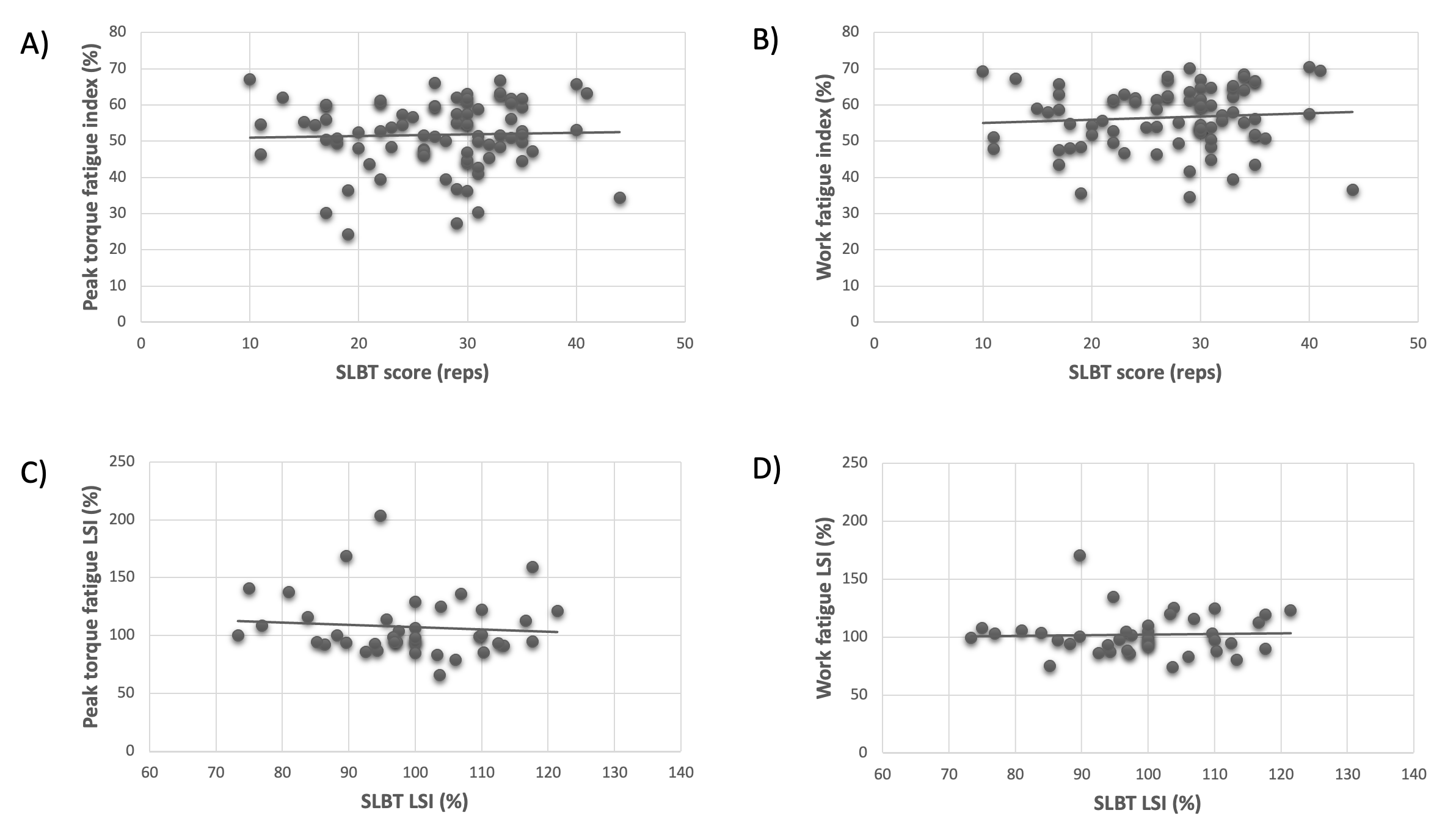
There was no significant correlation between the SLBT score and the hamstring fatigue indices provided by peak torque or work (p>0.05 for both; Table 1). Similarly, the LSI found in the SBLT was not significantly correlated with LSI found in hamstring endurance test (p>0.05; Table 2). Scatter plots on Figure 2 further demonstrate the failed association between the SLBT scores and the isolated hamstring endurance.
_and_.png)
DISCUSSION
This study aimed to investigate the correlation between the SLBT score and isolated hamstring endurance. There was no significant correlation between the SLBT score and the fatigue indices provided by peak torque or work measurements. Additionally, the between-limb performance symmetry in the SLBT score, assessed through LSI, did not show a significant correlation with those found in the hamstring endurance test.
The SLBT previously shown to be unable to represent hamstring maximum strength.18–20 Conversely, considering the nature of repetitions to task failure in the SLBT, the hypothesis that this test would show an acceptable correlation with muscular endurance appeared reasonable. Hence, the current study used the gold standard tool to assess muscular strength-related variables and implemented a testing protocol under highly controlled conditions in a laboratory environment to evaluate isolated hamstring endurance.21,22 To broaden the scope of the analysis, the current study employed both torque and work as methods for measuring muscle endurance. In both instances, the protocol proved effective in inducing muscle fatigue, as indicated by average values of approximately 52% (95%CI 50% to 54%) and 57% (95%CI 55% to 58%) drop in torque and work over the course of the 30 maximum-intensity repetitions, respectively.
The results of the present study contradict those who promote the SLBT as a measure of hamstring endurance.12,14,15 It is reasonable to consider some factors that may have played a role in these results. First, it should not be ignored that fatigue is a task-dependent phenomenon.23 Hence, a protocol involving a predetermined number of maximum-intensity isokinetic contractions may elicit a different fatigue response compared to a protocol continuing until task failure in an exercise with fixed resistance (in the case of SLBT, using the volunteers’ body mass). The volunteers were acquainted with the tasks involved in the SLBT and the isokinetic endurance test, but they did not have the opportunity to undergo multiple assessments to refine their execution strategy for each test. The instructions and verbal stimuli were aimed to volunteers perform as many repetitions of SLBT as possible up to failure and to maximally contract their hamstring muscles in every isokinetic repetition throughout the endurance test. Nevertheless, the perception of discomfort and fatigue triggered by each test is individual-specific, influencing the volunteer’s responses during the execution of each test.
Concurrently, and possibly with a greater relevance to the results, the contribution of gluteal muscles to the hip extension movement during the SLBT should be highlighted. The gluteus maximus is considered the most relevant hip extensor.24 Specifically during unilateral bridge exercises, studies have found similar activation levels between gluteus maximus and hamstrings25 or higher activation for gluteus maximus compared to hamstrings.26 In addition, the middle segment of gluteus medius and the posterior segment of gluteus minimus also exhibit high activation during the unilateral bridge.27 Therefore, gluteal muscles probably played a key role in the SLBT score, while they had no ability to contribute to the volunteers’ performance on the isokinetic endurance test, due to isolated knee flexion actions. In addition to the gluteal muscles, bridge exercises involve stabilizing muscles in the lumbopelvic region.25 Hence, these trunk muscles status may also influence the SLBT score.
Sprinting seems to place the highest demands on the hamstrings,28 and this muscle group is essential for horizontal force production during sprinting actions.29 Interestingly, in a situation of repeated sprint-induced fatigue, the gluteus maximus seems to assume a relatively more significant role than the hamstrings in horizontal force production.30 It has been hypothesized that gluteus maximus, as the primary hip extensor muscle, may compensate in a synergistic manner during sprinting for potentially altered hamstring muscle function due to fatigue.30 Applying this hypothetical scenario to the SLBT, the fatigue of the gluteal muscles would likely have a more decisive impact on the number of single-leg bridge repetitions before task failure than the hamstrings. This reinforces the notion that the current results might have varied if the isokinetic endurance test had incorporated repetitive hip extension movements instead of knee flexion. Conversely, since the SLBT has been described as a measure of hamstring endurance,12,14,15 the chosen protocol of repeated knee flexion actions emerged as the only way to assess hamstring endurance without involving other hip extensor muscles.
It is reasonable to speculate that the SLBT is likely a test assessing the endurance of the hip extensors. If this is correct, the SLBT score should not be attributed solely to the condition of the hamstrings or gluteal muscles in isolation. From a practical perspective, an athlete with well-functioning hamstrings may still struggle with the SLBT if their gluteal muscles are unable to effectively perform the task. Therefore, implementing a hamstring strengthening program focused on knee-dominant exercises, such as Nordic curls, might not be an effective approach. Conversely, a satisfactory SLBT score for an athlete undergoing HSI rehabilitation does not necessarily indicate that hamstring function has fully recovered. The role of the gluteal muscles in hip extension may be a critical factor for satisfactory performance, making a return-to-play decision after HSI based solely on the SLBT premature. Therefore, even if future studies validate the potential association between the SLBT and the hip extensors’ endurance, practitioners should be aware that this test may not distinguish whether a low score is attributable to the gluteal or hamstring muscles.
The authors acknowledge some limitations of the present study. First, these findings pertain to the performance of male recreational athletes, and caution should be exercised when extrapolating them to high-performance or female athletes. Second, none of the participants had previous experience with the SLBT or isokinetic testing, but the experience of some participants in specific sports may have positively influenced their performance in the SLBT due to their greater familiarity with the task. Third, conducting additional sessions to familiarize volunteers with each test was not feasible in this study. Conversely, the same evaluators conducted all assessments, with one responsible for the SLBT and the other for the isokinetic test, ensuring that volunteers received consistent instructions and verbal stimuli. Lastly, the SLBT necessitates evaluators with the ability to analyze technique, provide feedback, and count repetitions. Therefore, it is possible that some inherent errors in this assessment may have occurred in determining the test interruption due to task failure.
CONCLUSION
There was no significant correlation between the SLBT score and isolated hamstring endurance assessed isokinetically. Similarly, the between-limb symmetry found in the SLBT was not significantly correlated with those found in the endurance test. Therefore, the SLBT does not appear to be a suitable tool for measuring isolated hamstring endurance in healthy men.
Competing Interests
The authors have no conflicts of interest to declare.
Acknowledgements
BMB thanks CNPq-Brazil for the research productivity fellowship.
RAF and DMM thank CAPES-Brazil for scholarships.