BACKGROUND
Within a larger framework in the decision process for return to sports, recommendations for overhead athletes are reported considering normalized shoulder strength and scapular mechanics, range of motion (ROM), and successful completion of a plyometric program.1 However, many clinicians find it challenging to accurately measure shoulder strength due to limitations in equipment and expertise.
Shoulder strength assessment generally consists of isometric testing in neutral positions via manual muscle testing (MMT), handheld dynamometry (HHD), or isokinetic dynamometry (ID). Normative values for external rotation (ER) and internal rotation (IR) strength using HHD has been obtained in healthy adults,2,3 and physically active collegiate male and females.4 Studies indicate that HHD provides an assessment of shoulder IR/ER strength assessment that is highly correlated to assessments performed with ID.5 The concern, however, with MMT and HHD testing is that reliability of these methods is highly dependent on clinician size and strength.6 Additionally, because the testing position is static, HHD lacks the assessment of dynamic components associated with upper extremity movements required during overhead sports.7 In addition to torque output as a measure of strength, ID can capture endurance deficits and strength ratio imbalances which are predictors of shoulder injury.8 Ellenbecker demonstrated a significant difference in bilateral IR and ER strength measures between MMT grades and isokinetic dynamometry, widely recognized as the gold standard for measuring muscle strength and muscle endurance.9
Understanding the balance between the strength of agonist and antagonist muscles is crucial in evaluating and rehabilitating overhead athletes due to the intricate muscular activation patterns necessary for stability of the glenohumeral joint.7 One strategy for strength testing of the shoulder in multiple positions throughout the range of motion is ID. Multiple authors have reported normative isokinetic strength assessment data for athletes involved in judo,10 tennis,11,12 badminton,13,14 and volleyball.15 In baseball, isokinetic strength testing has been performed in high school athletes,16 collegiate athletes,17,18 and professional athletes,19 yet limited information is available regarding normative values of isokinetic shoulder strength in youth athletes.
Gaps remain in the literature, particularly regarding the establishment of normative values for younger, skeletally immature athletes and how these values differ across various stages of development. The purpose of this review was to examine the existing literature concerning the application of isokinetic shoulder strength testing in rehabilitation and clinical decision-making processes among youth athletes who perform repetitive overhead activities.
METHODS
This literature review was conducted in accordance with the recommendations of the "Preferred Reporting Items for Systematic Reviews and Meta Analysis extension for Scoping Reviews (PRISMA-ScR).20
Search Strategy
The literature review was performed with the databases PubMed, and EBSCO Host, which provides a range of databases, e-journals and e-books. Search terms included in the search strategies included phrases such as: “isokinetic dynamometry AND shoulder,” “isokinetic dynamometry AND shoulder AND youth athlete.” (See Appendix A for full search criteria). The search was limited to full-text available human research published between 2000-2024, including participants ages <18 years associated with an organized, overhead sport, and published in the English language. Exclusion criteria were articles pertaining to any neurological condition, and athletes designated as collegiate or professional.
RESULTS
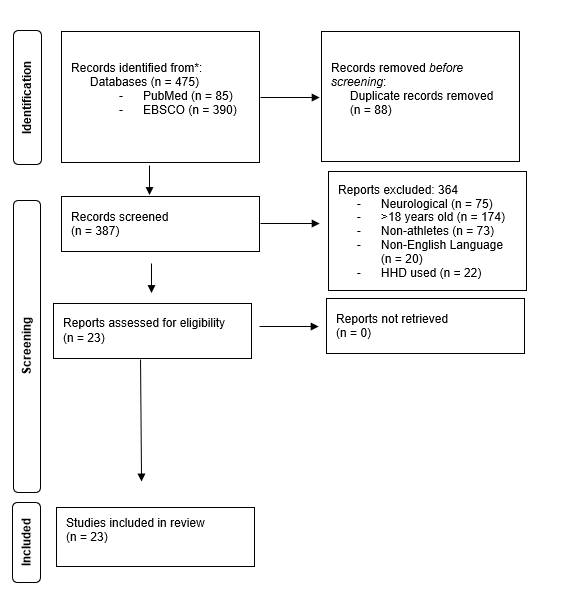
Electronic database searches identified 475 total studies. The scoping review included 23 studies21–43 after duplicate removal, title/abstract screen, and full text review.
The PRISMA diagram (Figure 1) outlines the search process in its entirety.

Isokinetic Dynamometry (ID) in Youth Repetitive Overhead Athletes
Of the included studies, volleyball was the most common overhead sport where ID was used for assessment.27,29–31,38,43 The second most common sport was swimming21–25 followed by handball,33,34,39,41,43 baseball,26,28,32,37 tennis,40,42,43 weightlifting,36 and basketball.31 In the articles that fit the inclusion criteria, two pertained to symptomatic patients,31,35 whereas the remaining articles looked at isokinetic normative values, or the effects of repetitive sport specific movements. Table 1 describes the use of ID in various sports along with the variety of parameters used for testing ID.
Isokinetic Testing Position
Testing positions throughout studies varied, but trends are seen when testing the upper extremity (UE) of youth athletes with ID as illustrated in Table 1. The most utilized testing position for shoulder IR/ER is the seated position with the shoulder abducted to 90 degrees and the elbow flexed to 90 degrees, commonly known as the 90/90 position. It is postulated that this position, more than the arm at a neutral position, specifically addresses muscle function often required for an overhead athlete.44 The use of the 90/90 position also demonstrates strong intraclass coefficient for test/re-test reliability.45 Ellenbecker has discussed using a modified position of 30 degrees shoulder abduction, 30 degrees shoulder forward flexion, and 30 degrees diagonal tilt of the dynamometer to determine tolerance of the UE strength test prior to using the ID at a 90/90 position.7 Additional alterations to the 90/90 positions used in research are the seated 90/30 (90 degrees elbow flexion and 30 degrees shoulder abduction),37 seated 90/45 (90 degrees elbow flexion and 45 degrees shoulder abduction),36 seated 90/30 with 90 degrees of shoulder abduction and 30 degrees of shoulder flexion,30 and the 90/90 supine position.40–43
Speeds Used for Testing
Table 2 provides information regarding the variations in the speeds used for testing youth athletes. Most studies assessed participants at multiple speeds for different outcome measures or for different sports-related contexts. Common speeds for assessment of isokinetic peak torque both concentrically and eccentrically include 60 deg/sec,22–25,27,29,30,32–34,38–41 90 deg/sec,28,31,37,39,43 120 deg/sec,26,36,41 180 deg/sec,21–25,28–30,32,37,38,40,42 240 deg/sec,27,33,34,36,39 300 deg/sec,38,42 and 360 deg/sec.36
Objective Measures from Isokinetic Dynamometry
Peak Torque
In many studies pertaining to the use of ID in youth athletes, peak torque, normalized via body weight, was the primary objective measure.26,27,29,40 Peak torque is then used to compute measures of bilateral symmetry, using left and right values, and unilateral strength ratios using shoulder external and internal rotation strength values. Research indicates that repetitive sports-related movements lead to discernible discrepancies in peak torque between shoulder external rotation (ER) and internal rotation (IR) strength when comparing the dominant and non-dominant arms in athletes. Repetitive motions during youth sports such as volleyball,27,38,43 swimming,21–25 and tennis40 result in increased IR peak torque in the dominant arm of the athlete. Variations exist among age groups within the same sport as evidenced by youth handball athletes demonstrating higher ER and IR peak torque in the dominant arm compared to non-dominant arm in athletes with a mean age of 17.6 years.41 Conversely, younger players (mean age of 14.6 years) showed no statistically significant difference between ER and IR peak torque.39 In a study of healthy teenage baseball players, Dupuis found greater concentric ER strength in the dominant arm at speeds of 90°/sec and 180°/sec.28 In contrast, Mickevičius observed decreased ER strength among younger baseball players (average age 11.6 years) who had a history of shoulder pain.35 It has been hypothesized that differences in peak torque output results in higher likelihood of overuse type injuries in youth athletes.24,27,41
ER:IR Ratio
Eight studies21–25,35,40,42 used concentric external rotation to concentric internal rotation strength ratios during for their objective measurements whereas six studies28,30,31,34,41,43 investigated various forms of eccentric to concentric ratios between ER and IR.
Comparison of shoulder agonist and antagonist muscle groups helps identify specific muscular imbalances.7 Variations in the dominant arm’s external rotation to internal rotation (ER:IR) ratios are frequently observed, particularly in cases where imbalances occur in the shoulder’s agonist-antagonist muscle relationships. These imbalances can signify weaknesses that heighten athletes’ vulnerability to injury.24,40 Ideal ER:IR has been defined as 66%, which remains constant throughout the velocity spectrum46; however, this ratio is described in skeletally mature athletes.7
A common theme in youth overhead athletes is decreased ER:IR ratio in the dominant arm21–24,34,40–42 due to the theorized increase in IR peak torque because of sport specific repetitive motion. Although these imbalances do not result in changes in athletic performance, there is fear that if not addressed in the younger athlete they can result in overuse type injury.40
There are unique variations of the ER:IR used in ID assessment of youth athletes as evidenced by discussion of ER:IR acceleration and ER:IR deceleration described by Yildiz in youth volleyball players.43 The concept eccentric to concentric ER:IR is defined as the ratio of balance for muscle activity where the shoulder medial rotators eccentrically control external rotation, while lateral rotators eccentrically control internal rotation, ensuring optimal shoulder function.47 This explanation is similar to Dupuis’ definition of Dynamic Control Ratio (DCR) in youth baseball players.28 Both Yildiz and Dupuis investigate the eccentric and concentric relationship of the ER:IR ratio of the shoulder. In each case, the ER:IR ratio into the acceleration phase (concentric ER to eccentric IR) was observed to be higher in the dominant arm,28,43 whereas the ER:IR ratio into the deceleration phase (eccentric ER to concentric IR) is lower in the dominant arm of the youth volleyball athlete,43 but no difference existed in the youth baseball athlete.28
DISCUSSION
This scoping review highlights the use of isokinetic dynamometry of the youth overhead athlete to obtain multiple objective measures. In adolescent overhead athletes, the repetitive nature of sport-specific movements imposes unique demands on the dynamic muscular control of the glenohumeral joint. This demand is highlighted by fluctuations in the external rotation to internal rotation peak torque ratio, a phenomenon hypothesized to significantly impact the vulnerability of the shoulder complex to injury.21–25 Various studies support this hypothesis, including symptomatic athletes35 and those with glenohumeral internal rotation deficits.31
In sports like baseball, dynamic muscular control of the glenohumeral joint is essential, particularly given the substantial stress experienced across the upper extremity joints during pitching. The angular velocities of shoulder internal rotation and elbow extension can range from 1,000 deg/sec to 7,200 deg/sec in youth and collegiate pitchers, respectively, from maximum external rotation through the acceleration phase.48,49 While ID testing velocities of 240 deg/sec do not fully replicate these speeds, they still yield valuable data on shoulder musculature function at higher isokinetic speeds.50 Table 3 provides a detailed breakdown of these different sport-specific findings.
GAPS IN THE LITERATURE
ID studies of youth athletes skew towards specific sports such as volleyball and swimming. Limited information is available regarding the use of ID for assessment of athletes participating in youth baseball. In reviewing the ages of participants recruited for ID articles in youth athletes, the youngest subjects were 11 years old. However, pitching and repetitive throwing in baseball often begins as early as 6-7 years of age. Studies included in a systematic review suggest that starting repetitive pitching at 10 years of age or younger increases the risk of upper extremity-related injury.51 In most sports, children are playing and specializing in sport positions at a much younger age than captured in this review, but changes in shoulder IR strength between dominant and non-dominant arm has been seen in youth throwers under the age of 10 using HHD.52 Understanding dynamic strength values and muscular balance relationships with measurements from ID in skeletally immature athletes and the changes that occur with repetitive overhead motions can assist in developing injury prevention, rehabilitation programs, and return to sport decision making for youth throwing athletes.
LIMITATIONS
Only studies in English languages were included in the review and the range of articles searched were between 2000-2024. Also, no quality assessment of the studies was performed, which may limit the impact of the findings.
CONCLUSION
Isokinetic dynamometry as an assessment in youth overhead athletes provides insights into shoulder strength (torque) and strength ratios. There is variety in the assessment parameters utilized in the included studies of youth athletes in various sports. By precisely evaluating isokinetic strength, clinicians can gauge the shoulder’s dynamic control, facilitating the tailored design of training programs. Isokinetic assessments allow for detailed analysis of power and the balance between agonist and antagonist muscle groups during movement, enabling the identification of specific strength impairments and guiding targeted interventions to enhance upper extremity loading tolerance for repetitive overhead activities.
Conflict of Interest
The authors declare that they have no conflicts of interest related to the content of this manuscript.