
INTRODUCTION
Shoulder pain is a common issue among overhead athletes participating in baseball, volleyball, tennis, swimming, and handball, with reported prevalence rates ranging from nine to forty-nine, depending on the sport and study.1–3 The repetitive overhead movements and high biomechanical demands associated with these sports increase the risk of shoulder injury.4
Several risk factors for shoulder pain in overhead athletes have been identified, including male sex, a body mass index over 25, age between 20 and 25 years, training for more than 16 hours per week, limited shoulder range of motion, and strength deficits in rotator cuff muscles.1,3,5,6
In various overhead movements, such as a tennis serve, a volleyball spike, and a handball throw, the kinetic chain consists of a sequence of coordinated actions that contribute to the generation of velocity and force applied to the ball.4,7,8 The kinetic chain is initiated by the lower extremities with a push-off from the ground, engaging the muscles of the calves, quadriceps, and gluteal muscles, leading to the extension of the hips, knees, and ankles. The force produced by the lower limbs is then transferred to the core musculature. The core serves as a critical intermediary, stabilizing the trunk and facilitating efficient transfer of energy from the lower to the upper body. The rotational movement of the trunk generates force that is transferred through the torso and into the arms amplifying the power of the overhead movement. The lower extremities and trunk are responsible for approximately 55% of the kinetic energy delivered during a baseball throw.4 Proper scapular control is essential for optimal shoulder mechanics, requiring coordinated motion of the scapulae with the arm. During overhead motion, the shoulder undergoes a combination of external then internal rotation, abduction and flexion. As the arm reaches the overhead position, the elbow extends, while the forearm muscles regulate the wrist’s position and motion, ensuring the hand is correctly aligned for the desired action.
Each segment in the kinetic chain must be functional to minimize the risk of shoulder injury and ensure optimal performance.4 A 20% reduction in energy production by the trunk can increase the load on the shoulder by up to 34% to maintain the same performance level.8 Such deficits may arise from poor technique, muscle weakness or imbalance, limited range of motion (ROM), or previous injury.4,8 Therefore, limitations in hip ROM, thoracic rotation, hamstring and quadriceps extensibility, and core neuromuscular control have been highlighted as factors leading to shoulder injuries.9–11
Researchers have also suggested that injuries are interrelated across different regions of the body. For instance, Finch et al. reported that one in eight injuries in Australian Football players occurs as a subsequent injury, regardless of the initial injury’s location.12 Similarly, a systematic review by Toohey et al. identified an association between a history of anterior cruciate ligament (ACL) injuries and subsequent hamstring injuries. They also found that a previous muscle injury, involving the hamstrings, quadriceps, adductors, or calves, was linked to an increased risk of subsequent injuries at different anatomical sites.13 These findings highlight the interconnected nature of injuries, particularly those originating in the lower limbs, suggesting that an initial injury can predispose athletes to additional injuries elsewhere in the body.
Even when an athlete is deemed fully recovered, initial injuries can result in tissue adaptations and neuromuscular alterations, which may predispose them to further injuries.14,15 Asker et al. have postulated that a history of shoulder or elbow injuries could serve as a potential risk factor for subsequent shoulder pain.1 However, the impact of pain within other regions of the kinetic chain on the risk of subsequent injuries has not been extensively studied. Therefore, the purpose of this systematic review was to evaluate the association between pain in the shoulder, trunk, and lower limb among overhead athletes.
METHODS
Study Design
This systematic review followed the COSMOS-E (Conducting Systematic Reviews and Meta-Analyses of Observational Studies of Etiology) and PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).16,17 It was prospectively registered with PROSPERO, registered PROSPERO 2023 CRD42023398806. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023398806.
Eligibility Criteria
Studies were considered for review if they met the following criteria: 1) inclusion of overhead athletes (e.g., tennis, baseball, badminton, handball, volleyball, American football, javelin, water-polo, cricket, basketball) without age restrictions, 2) investigation of injury or pain in shoulder and lower limb or trunk, 3) had data related to or could calculate the calculation of odds ratio (OR) or relative risk (RR), 4) availability in French or English. Studies were excluded if they focused on interventions aiming to reduce the risk of shoulder pain.
Information Sources and Search Strategy
A systematic search was conducted in July 2023 in the following databases: PubMed/MEDLINE, Science Direct and CENTRAL/Cochrane. The search terms included keywords and MESH (Medical Subject Heading) as shown in Appendix 1. Research review and review article filters were selected for Science Direct. Each column was combined with Boolean operators (AND and OR). Additionally, a hand search was conducted through the bibliography of relevant articles. See Appendix 2 for details.
Selection Process
All identified articles were added to the Rayyan® software which assisted in removing duplicates. Two independent reviewers (ML and FL) screened and assessed the eligibility of studies based on title and abstract. Full-articles were then retrieved and read to determine whether they were to be included. Disagreement was resolved with a third reviewer.
Data Collection Process and Data Items
ML conducted data extraction which was subsequently verified by FL. Extracted data included metadata (author, publication date, country), population characteristics (number of persons included, age, sport, level and training load), study design, pain or injury locations, effect estimation and confidence interval. Authors were contacted in cases where data were missing.
Study Risk of Bias Assessment
The risk of bias was evaluated using Cochrane ROBINS-E (Risk of Bias In Non-randomized Studies - of Exposure) tool.18 This tool assesses seven domains of bias: confounding, measurement of the exposure, selection of participants into the study, post-exposure interventions, missing data, measurement of the outcome and selection of the reported result. Each bias domain is addressed using a series of signaling questions judging the risk of bias of each domain (low risk, some concerns, high risk of bias, very high risk of bias).
Synthesis Methods
Search results were illustrated in a flow diagram and the characteristics of each study, along with their results, were summarized in tables. A random-effect meta-analysis was performed when at least two studies evaluated the association between shoulder pain and pain in another joint. The analysis was conducted using RevMan 5.4 ® software. The meta-analysis used the inverse variance Der Simonian and Laird method. The overall odd-ratio (OR) with 95% confidence interval (CI) were calculated. An OR of 1,0 indicates that there is no difference in odds between the groups whereas an OR > 1,0 indicates an increase in odds among the exposed athletes.19 Heterogeneity was assessed using the I² statistic. It was considered high when I² was greater than 50%.19 A qualitative synthesis was performed when it wasn’t possible to pool the results due to high heterogeneity.
Reporting Bias Assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to rate the quality of each association. This tool evaluates risk of bias, inconsistency, indirectness, imprecision, publication bias, large effect, dose-response and antagonistic bias and delivers recommendations (high, moderate, low or very-low certainty of evidence).
RESULTS
Selection of Studies
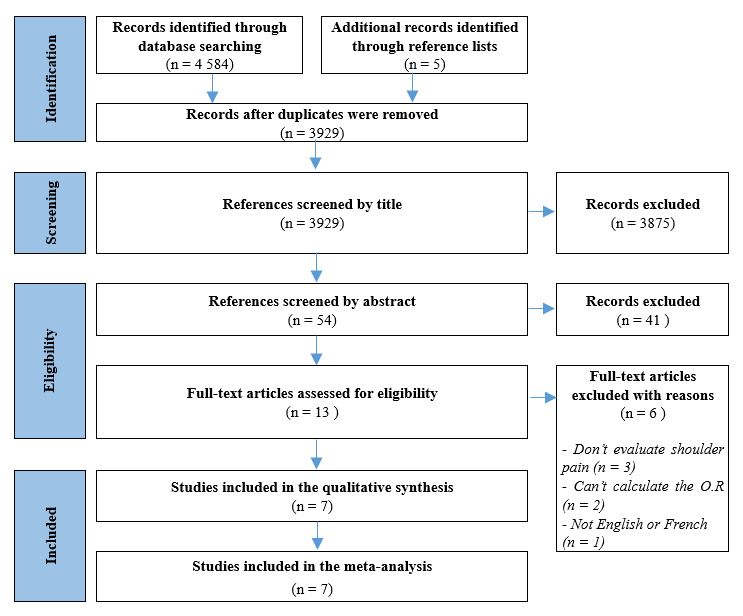
Overall, the search strategy identified 4 584 articles with an additional five studies were found by checking the references of other articles. After screening articles based on title and abstract, 13 articles were identified and thoroughly examined. Ultimately, seven articles met the inclusion criteria for the systematic review.20–26 Of these, six studies were cross-sectional and one was a longitudinal study. All studies were included in the meta-analysis. See Figure 1.
Characteristics of Included Studies
Overall, 5785 athletes were included in this review. Patients were aged between seven and 28 years old and played water-polo, basketball, baseball, softball, handball, tennis, badminton and volleyball. The play level was heterogenous, ranging from the last division to the international level. Every study assessed the association of shoulder pain with other body region. Five studies evaluated low back pain,21,23–26 two evaluated hip pain,20,23 three evaluated knee pain,23,24,26 and two evaluated ankle and foot pain.22,23 Every study used questionnaires for data collection.
The characteristics of each study are detailed in Table 1.
Study Risk of Bias Assessment of Included Studies
Two studies were rated as having a high risk of bias while five were deemed to have some concerns. The poorer quality observed was primarily attributed to the lack of consideration for confunding factors, the subjective nature of outcome/exposure measurement through questionnaire, and issues related to the selection of participants. (Table 2)
Synthesis of Results
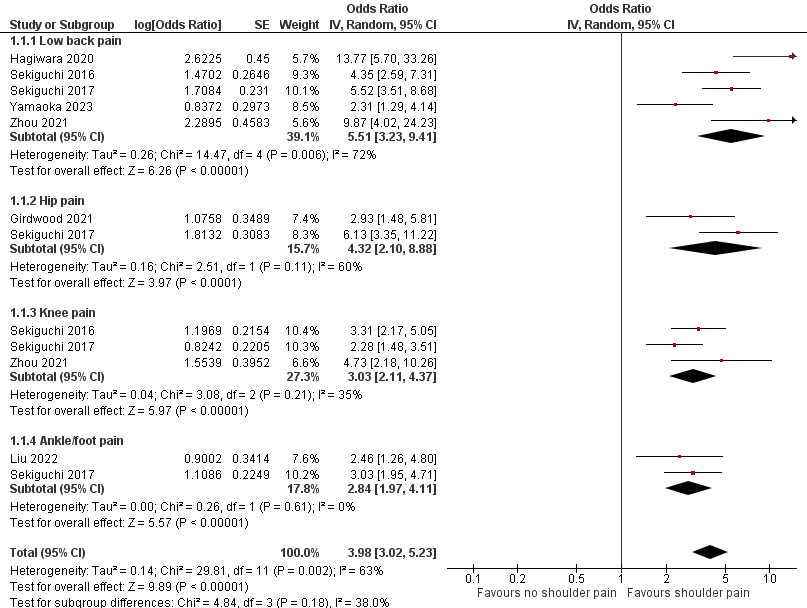
The association between shoulder pain and back pain, hip pain, knee pain and ankle/foot pain were assessed through meta-analysis. Shoulder pain demonstrated a significant association with back pain (five studies, OR = 5.51, 95% CI [3.23-9.41], high heterogeneity), hip pain (two studies, OR = 4.32, 95%CI [2.10-8.88], high heterogeneity), knee pain (three studies, OR = 3.03, 95%CI [2.11-4.37], low heterogeneity), ankle/foot pain (two studies, OR = 2.84, 95%CI [1.97-4.11], low heterogeneity). (Figures 2)

Quality of Evidence
The quality of evidence according to GRADE is presented in Table 3. Reasons for downgrading are cited in the table’s legend. The overall quality of evidence for the association of shoulder pain, back pain and knee pain was rated as low. Additionally, the evidence was considered very low for the association between shoulder pain and hip pain as well as shoulder pain and ankle/foot pain.
DISCUSSION
Results Interpretation
The aim of this systematic review was to evaluate the association between shoulder pain and trunk/lower limb pain in overhead athletes. There is low to very low evidence of an association between trunk/lower limb pain and shoulder pain, but overhead athletes with trunk or lower limb pain appear to be two to five times more likely to also suffer from shoulder pain compared to those without pain in the kinetic chain.
The overhead movement is a sequential motion supposed to be initiated with the proximal segments and ending at maximum speed with the distal segments secondary to the summation of accelerative forces generated by the previous segments in the kinetic chain.4,7,8 A breakage, also known as a dysfunctional segment, in the kinetic chain increases the demand on the subsequent segments to maintain the functional ability or performance, a process known as the catch-up phenomenon.8,27 While this concept is well-known and described in numerous studies and reviews, the consequences of this catch-up have not been thoroughly studied.4,7,8
This systematic review suggests the existence of a relationship between shoulder pain and trunk/lower limb pain. Only two studies included in the systematic review evaluated the causal relationship between these pain.22,25 Yamaoka et al. showed that in the year following low back pain a baseball player was 2.31 times more likely to suffer from shoulder pain. According to the concept of the kinetic chain, functional factors such as poor lumbopelvic control have been brought out.9,28,29 However, not all studies generalized these conclusions. For example, Machado et al. concluded in a meta-analysis of 65 studies in 2023 that there was low evidence of no association of trunk/lower limb strength, endurance, vertical jump or balance measures with shoulder pain. Yet, overhead athletes with shoulder pain were performing worse in trunk stability and endurance in tests like side bridge or trunk flexors/extensors.30 This suggests that despite the lack of a direct association with shoulder pain in some measures, like vertical jump or balance, core stability remains a critical factor for performance and injury prevention in overhead athletes. Some authors have also emphasized the role of the anatomy of the latissimus dorsi—particularly its insertions to the thoracolumbar aponeurosis, iliac crest, scapula, and bicipital groove—as a contributing factor to shoulder pain following low back pain.21 Due to its attachments, the latissimus dorsi muscle is responsible for shoulder adduction, extension, internal rotation, as well as lumbar extension and lateral flexion.31 It is the only muscle that connects the upper body to the lower body. Laudner and Williams have found that swimmers with a latissimus dorsi muscle that presented high resistance to deformation were more prone to have scapular movement dysfunction.32 Scapular movement is an integral part of the kinetic chain, and any disruption may reduce the efficiency of energy transfer.4
This systematic review indicates an association between shoulder pain and pain in distal body regions. While the results of the meta-analysis showed that the dysfunctional proximal segments had a higher probability of provoking shoulder pain, knee and ankle pain could also alter the kinetic chain dynamic. The ankle and foot play a significant role, as it has been recognized that foot arch posture is associated with shoulder and elbow surgeries.33 Liu et al. demonstrated that kinetic chain disruption can occur after an injury.22 However, the rehabilitation process following these injuries remains unclear. Secondary or subsequent injury can occur years after the initial injury/pain due to compensatory mechanisms. Even a well-rehabilitated injury can affect surrounding tissues in both the short and long term, increasing the athlete’s susceptibility to further injury.34
Clinical Implications
There is evidence that a subsequent injury causes greater time loss and medical attention than a first injury.12,13 Therefore, it is essential to reduce the risk for subsequent injury by managing return-to-sport after a first injury and to treat any pain seriously the overhead athletes may feel while playing.
During the assessment of an injured overhead athlete, physiotherapists must consider every link in the kinetic chain. A shoulder injury can be the consequence of a modification in the motion pattern in the kinetic chain, just as lower limb or trunk pain/injury can lead to another injury if the kinetic chain has not been properly addressed. Shoulder ROM, rotator cuff strength, and functional test like the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) or the Upper Limb Rotation Test (ULRT) can be performed to assess shoulder function within the kinetic chain.27,35,36 The CKCUEST is designed to assess upper extremity strength, stability, endurance, and coordination in a closed kinetic chain, where the hands maintain contact with a fixed surface throughout the movement. It requires the coordinated activation of various upper body and core muscles, and its performance has been shown to correlate with shoulder function and injury risk, making it a valuable tool for both injury prevention and rehabilitation. Similarly, the ULRT evaluates dynamic shoulder mobility, stability, and coordination, with a specific emphasis on rotational movement of the upper limb. This test provides clinicians and coaches with insights into the functional rotational range of motion of the shoulder, enabling the identification of movement limitations or asymmetries that may contribute to injury or dysfunction. It is also valuable to assess functional movement during the lunge test or leg squat test to identify any dysfunction in the kinetic chain.37 Nagamoto et al. evaluated the association between baseball players with a history of shoulder or elbow pain during or after playing baseball and their ability to deep squat. Although it may not be directly associated, their performance was adversely affected.38 This shows that after a shoulder injury the entire athlete has to be considered. Clinicians have to treat the injury, maintain or restore strength and mobility in the kinetic chain, and incorporate kinetic chain exercises as soon as possible in order to guide the athlete in returning to sport. As previously explained, it is essential to rehabilitate the entire movement to mitigate the risk of the catch-up phenomenon. Moreover, injury can lead to changes in the cortical areas of the brain, altering neuronal processing even after the patient has physically recovered.39 Consequently, incorporating motor imagery, gradual exposure to movement, and external cues during rehabilitation are crucial for addressing both the physical and neurological aspects of recovery.27
The Van Mechelen model is a widely adopted framework for injury prevention, consisting of a four-step approach: identification of the problem, determination of risk factors and injury mechanisms, implementation of a preventive intervention, and evaluation of the intervention’s effectiveness.36 However, the prevention of any injury in overhead athletes cannot be fully addressed with the Van Mechelen model, as its linear approach cannot capture the complexity of injuries with a single risk factor.36,40 This systematic review underscores the association between trunk and lower limb pain and shoulder pain in overhead athletes, reinforcing the concept that injuries arise from a combination of risk factors. As previously noted, potential risk factors for overhead athletes include training volume, BMI, age, ROM deficits, strength deficits, sport-specific techniques, core endurance deficits, muscle extensibility, and a history of shoulder or elbow injuries.1,3,5,6,9–11 The presence of a single risk factor does not predict the occurrence of shoulder pain. Bittencourt et al. proposed a more “complex system approach” where all determinants (intrinsic, extrinsic, modifiable, non-modifiable) interact with each other in unpredictable and unplanned ways, creating a web of determinants.40 It enables the identification of patterns between determinants, the characteristics of the phenomenon and the emerging trends that arises from the web of determinants. This approach could facilitate the development of individualized risk profiles by evaluating each determinant throughout the rehabilitation process, leading to a better understanding of subsequent injuries. In line with the complex system approach, this systematic review proposed an initial interaction between lower limb/trunk pain and shoulder pain in overhead athletes. Thus, coaches or trainers should identify overhead athletes at risk for subsequent injuries when they first perceive any discomfort or pain. To detect injuries at an early stage, medical staff needs a reliable surveillance method that encourages athletes to disclose any discomfort. Surveillance programs usually define an injury using time-loss or medical attention criteria.41 In 2014, the Oslo Sports Trauma Research Center (OSTRC) questionnaire was created to declare all complaints, offering a better assessment of overuse injuries. Therefore, an all-complaint based surveillance method is a crucial tool for monitoring overuse injuries, allowing sports professionals to identify early signs of injury, assess severity, and develop strategies to prevent further complications.42
Limitations
This systematic review presents several limitations. First, the included population is not representative of the overall overhead athlete population. The mean age of athletes is low and although age was assessed as a confounding factor and statistics were adjusted, the results might still be underestimated. Adolescents often exhibit a higher susceptibility to overuse injuries compared to younger children.43 Secondly, the definition of pain or injury may have differed between authors. In this systematic review, only Liu et al. and Zhou et al. defined pain or injury in the questionnaire, which introduces heterogeneity in exposure and outcome assessments. Additionally, the data were collected through self-reported questionnaires, which introduce the potential for recall bias, possibly affecting the accuracy of the responses. Also, while adjusted results were included in this study when available, the confounding factors taken in consideration were not consistent across studies. For the majority of the studies, gender, age, BMI, team level, hours of training per week and per weekend were considered. Furthermore, the study by Sekiguchi et al.23 included athletes with shoulder and elbow pain, which could have biased the results. Finally, due to the design of the included studies, it was not possible to determine a causal relationship between shoulder pain and trunk/lower limb pain; only associations between these factors can be concluded.
To establish a causal relationship between shoulder pain and trunk/lower limb pain, future longitudinal studies should be implemented with a clear definition of pain/ a painful event and assessment should be standardized using an all-complaint questionnaire.
CONCLUSION
This systematic review highlights, with very low to low certainty, a significant association between shoulder pain and trunk/lower limb pain. Overhead athletes with trunk or lower limb pain appear to be two to five times more likely to also suffer from shoulder pain compared to those without pain in the kinetic chain.