

INTRODUCTION
Handball is a vigorous team sport characterized by physical contact and collision between players, rapid change of direction, and powerful, repetitive throwing. Shoulder problems are common among handball players with a reported prevalence of 17-36% and most shoulder problems are defined as overuse injuries.1–5 The prevalence of shoulder problems defined as substantial (causing moderate or severe reductions in sports performance or complete inability to participate6) has been reported to be 5-12%.3–5
An increasing number of studies have attempted to identify possible risk factors for shoulder problems in handball, due to their high prevalence and impact on sports participation.1,3,7–9 Their main findings have indicated that potential risk factors for shoulder problems include decreased strength of the external rotators1,3,7 (ER) and internal rotators1 (IR) in the throwing shoulder, scapular dyskinesis,1,3 and a low ER/IR strength ratio.7 The posterior rotator cuff (infraspinatus and teres minor) has been shown to be very active during the deceleration phase of the throwing motion, indicating the importance of ER strength and a high ER/IR ratio.10 Decreased total rotation range of motion and a sudden increase in training load have also been identified as possible risk factors.3,7,8 However, a study aiming to confirm previously identified risk factors for overuse shoulder problems was unable to do so regarding ER strength, total rotation range of motion, or scapular dyskinesis.9 Furthermore, a recent systematic review on risk factors for shoulder problems in overhead athletes showed limited or conflicting evidence for a variety of factors like participation level, sex, biomechanics, and external workload.11
Recent studies investigating the prevalence of shoulder problems and possible risk factors have primarily examined factors related to the shoulder girdle.1,3,4,7–9,12 However, overhead throwing is a complex movement involving the whole body and the kinetic chain. The kinetic chain has been described as a linkage of multiple body segments that transfer forces and motion through the body and throwing velocity is generated via the acceleration provided through the lower extremity and the trunk muscles.13,14 Efficient force transmission from the lower extremities, through the pelvis and the trunk and to the upper extremity, called “the proximal to distal sequence”, is considered very important for throwing performance in sports.14–16 Kibler´s biomechanical analysis of the tennis serve showed that 51% of the total energy production originates from the lower extremities and the trunk, while only 13% is generated at the shoulder.17 Furthermore, studies on baseball players have shown high levels of activity in the gluteus maximus and medius muscles and a positive association between gluteal activity and pelvic axial rotation during a pitching motion, reflecting the importance of the kinetic chain for throwing performance.18 During throwing, deficits proximally in the kinetic chain may increase the loads on the more distal segments, such as the shoulder, which might lead to the development of shoulder problems.19
Without participation in a sport, however, non-participation-related risk factors like reduced strength or non-efficient force transmission through the kinetic chain may be of limited importance. A study by Moller et al. showed that a weekly increase of 20-60% in handball load (training and competition hours - described as a participation-related risk factor) led to increase of shoulder injury rate in players who had other underlying risk factors (non-participation-related) like diminished ER strength and scapular dyskinesis, indicating the contribution of sport participation towards increased injury risk.8 The complexity and the chaotic nature of the game of handball presents difficulties for monitoring participation-related shoulder load (PSL) such as the number of throws. A new way of monitoring PSL (number of throws, playing position etc.), was therefore introduced in the “2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels”. The consensus suggested the use of the modified Borg rate of perceived exertion scale to track the athlete´s weekly PSL in sports like handball.20
To the author’s knowledge, the influence of lower body strength and trunk rotation power (TRP) on shoulder problems in handball players has not previously been investigated. Moreover, the interaction between PSL and non-participation-related risk factors, like reduced lower body strength and TRP, has not been investigated in handball players. Hence, the aim of this study was to assess: 1) The association between pre-season lower body strength, TRP and shoulder strength measurements and shoulder problems among handball players, and 2) Whether pre-season strength and power measurements influence the association between PSL and severity of shoulder problems.
The hypotheses were that: 1) Handball players with low pre-season strength and power values would report more shoulder problems when followed through a regular season, and 2) Players with low pre-season strength and power values would report more severe shoulder problems as PSL increased through a regular season.
MATERIAL AND METHODS
Study Design and Participants
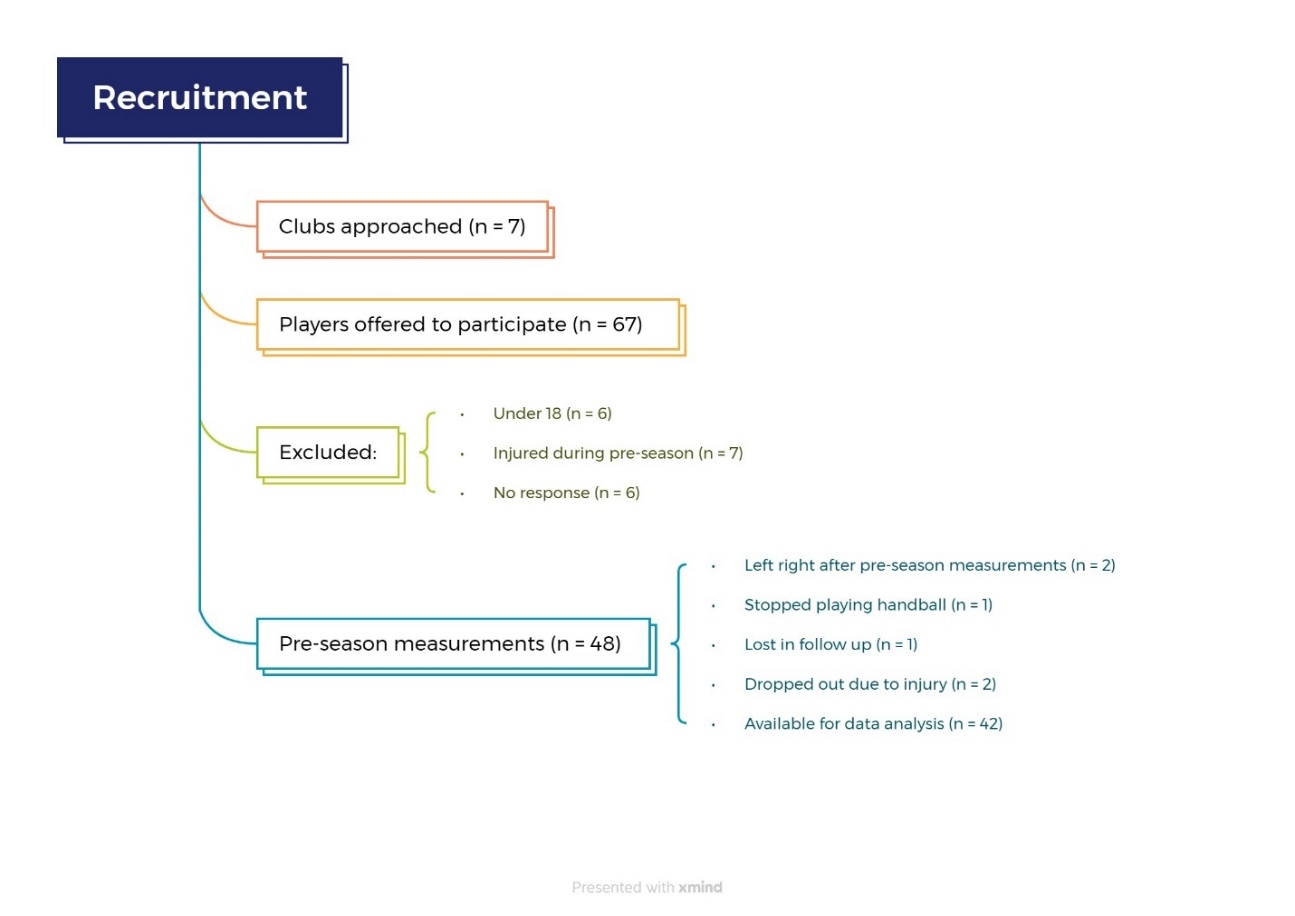
Seven clubs from the top Icelandic men’s handball division were approached in June 2022 and invited to participate in this prospective study. Players 18 years and older were eligible for the study, irrespective of previous or current shoulder problems. Players who were away from full participation and training due to injuries during the pre-season data collection period were excluded from the study. No other exclusion criteria were used. Pre-season strength and power measurements were conducted in August and September 2022. The measurements took place at the Research Center of Movement Science at the University of Iceland. A flowchart of the study recruitment and data collection is presented in Figure 1. Prior to data collection players received information about the study and signed a consent form. The study was approved by the National Bioethics Committee (VSN-22-084).

Isometric Mid-thigh Pull
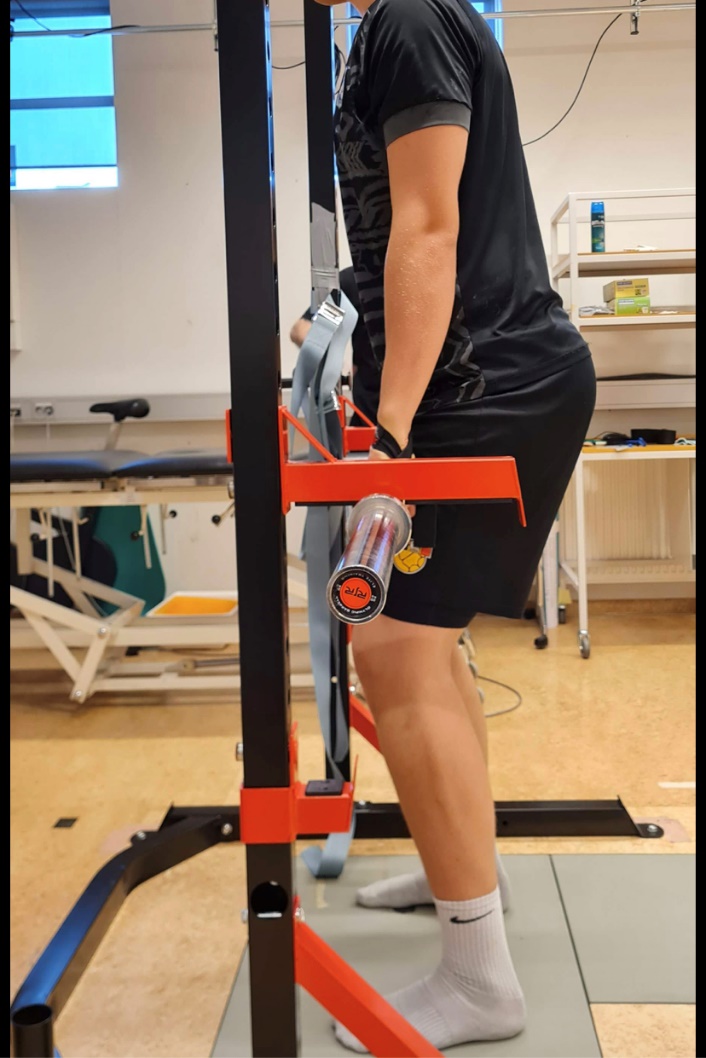
Lower body strength was measured with the Isometric mid-thigh pull (IMTP), a well-established and reliable test for lower body peak force measurements (Figure 2).21 Peak force of the IMTP has been shown to correlate highly with one repetition maximum squat and deadlift, indicating its appropriateness for measuring lower body strength in laboratory settings.22,23 Participants finished a standardized warm up routine and got three familiarization trials (at 50%, 75% and 90% subjective effort). During testing, knee and hip angles were standardized (between 125-145° and 140-145° respectively) as recommended by Comfort et al.24 Participants held a 20 kg weightlifting bar in a fixed position with their hands strapped to the bar with weightlifting straps to minimize the effect of their grip strength, while positioned on a force plate (AMTI, Watertown, Massachusetts, USA) to measure the vertical component of the ground reaction force, sampling at 100 Hz. Participants were encouraged to push as hard and as fast as possible down into the force plate and all got verbal encouragement during each trial. Three trials were performed, and in cases where peak force (PF) values exhibited an increase between the second and third trial, extra trials were conducted until the PF values differed by less than 250 N.24 The trial with the highest absolute PF value, including participant´s body weight, was used for data analysis.

Trunk Rotation Power
TRP was measured with a pulley machine in a seated position with the hips and knees in 90° flexion.25 Participants were instructed to keep the elbows straight in front of the body at shoulder height and the trunk in an upright position and to avoid all side bending motion, while rotating 5% of their body weight through 180° as fast as possible (Figure 3). Prior to conducting the measurements, participants completed a standardized warm-up routine and underwent two familiarization trials. A non-slip mat was placed under the participants´ feet and buttocks to prevent any sliding on the floor or on the plinth. Only left-side rotation was measured for right-handed players and right-side rotation for left-handed players. The acceleration of the weight was measured with inertial sensors (Movella dot, Henderson USA), placed on the top of the weights in the pulley machine and raw data were collected through the Movella dot app (Movella dot, Henderson USA). The acceleration values were then converted to power (W=(a+g)*t*F) (W=watt, a = acceleration, g = gravity, t = time, F = is the force, and represents the weight of the pulley). Three trials were performed and the trial with the highest absolute power value was used for data analysis.
A reliability analysis was done as this method differed slightly from the original version by Andre et al.25 Fourteen physiotherapy students were measured with 24-48 hours in between measurements to determine the test-retest reliability. The results showed good reliability, an ICC (3,3) value of 0.874, standard error of measurement (SEM) of 5.17, coefficient of variation (CV) of 17% and MDD90 of 12.03.

Shoulder Strength
An externally fixed handheld dynamometer (HHD) (Lafayette Instruments, USA) was used to measure maximal isometric IR and ER strength of the dominant shoulder in a supine position, with the shoulder in 90° abduction and 0° rotation (Figure 4).8,26 A towel was placed under the distal end of humerus to keep the upper arm in the horizontal plane. Participants finished a standardized warm up routine and got one familiarization trial.12 Participants were instructed to maintain stability in their torso, upper arm, and elbow and to avoid any substitution. They were given instructions to exert maximum force upon cue and maintain it for a duration of three seconds. Stabilization was provided to the HHD and to the upper arm by the examiner (KA) and participants got verbal encouragement during each trial. The average value from the three trials was used for data analysis.26

Self-Reported Measures
Self-reported data were collected and managed using REDCap electronic data capture tools hosted at University of Iceland, with the Oslo Sports Trauma Research Center Overuse Injury Questionnaire (OSTRC-O2)27 emailed to all participants once a week throughout the regular season or for 31 weeks. An automatic reminder was sent to non-responders after two and four days. The OSTRC-O2 questionnaire has been widely used in handball related research and is specially designed to document the extent of overuse injuries in sports.3,4,6,9,27 The participants were asked about shoulder problems in their dominant shoulder with shoulder problems referring to any pain, ache, stiffness, clicking/catching, swelling, instability/giving way, locking, or other complaints related to the dominant shoulder. The questionnaire included four questions about whether shoulder problems had affected participation, training/competition, or performance, and whether participants had experienced any pain in the dominant shoulder related to handball for the prior seven days. Each question had four response options, scored on the scale 0-8-17-25, 0 representing no problem and 25 maximum level. The scores from each of these four questions were then summed to calculate a weekly severity score on the scale 0-100. The average OSTRC-O2 severity score of each participant was calculated by dividing the total score from all the questionnaires answered throughout the season by the number of times answered. The group prevalence of shoulder problems was calculated by dividing the total number of times any participants reported any problem (anything but the minimum value in any of the four questions) with the total number of questionnaire respondents that week. The individual prevalence of shoulder problems was calculated by dividing the total number of times each participant reported a problem (anything but the minimum value in any of the four questions) by the total number of that participant´s questionnaire responses. The group and individual prevalence of substantial problems was calculated in the same way, respectively, for shoulder problems that had caused moderate or severe reduction (score 17 or 25 on questions no. 2 and/or 3 on the OSTRC-O2) in training/competition or performance or total inability to participate (score 25 on question number 1 on the OSTRC-O2).27
Additionally, the authors added a question to the weekly questionnaire that asked the participants to rate the weekly PSL on a modified Borg rate of perceived exertion scale, by answering the question “On the scale 0-10, how hard was the recent week on your throwing shoulder?” as recommended by Schwank et al.20
Outcome Measures, Data and Power Analysis
The outcome measures were: 1) The association between the pre-season strength and power measurements and OSTRC-02 results (individual prevalence, individual substantial prevalence, and severity score); 2) The influence of pre-season strength and power measurements on the association between PSL and the OSTRC-O2 severity score.
All statistical work was done in Microsoft Excel and Jamovi statistical software (2023). The Shapiro-Wilk test was used to check the data for normality. The Spearman´s rank correlation coefficient was applied to examine the association between variables in the first outcome measures, while a mixed model ANOVA was conducted to analyze the second outcome measure. An a-priori power analysis was conducted, indicating a sample size of minimum 46 participants to achieve 80% power for a correlation value of 0.4 for the association between the pre-season measurements and the OSTRC-O2 results. The p value was set at 0.05 for all analyses.
Participants were asked not to answer the questionnaire if they were away from regular training and/or competition because of an injury. Some participants who got injured during the season nonetheless continued to answer the questionnaire while they were away. They were contacted by one of the authors (KA) and information gathered about the type of injury and the time they were away, and appropriate questionnaire data removed from the data analysis.
RESULTS
Participants
A total of 42 male handball players participated in this study. Participants’ demographics can be found in Table 1. Two players had a history of previous surgery of the throwing arm and 19 had a history of major lower limb injury, e.g., fracture, muscle tear, tendon rupture, ligament tear and meniscal injury.
Self-reported Shoulder Problems and PSL
The average response rate for the OSTRC-02 questionnaire was 87%, with 16 players having 100% response rate,14 players having a response rate above 80% and 12 players below 80%. The average group prevalence of shoulder problems was 27% (95% CI 19.8-35.2, range 0-100%) and the average group prevalence of substantial shoulder problems was 4% (95% CI 1.75-7.77, range 0-52%). Fifteen players reported substantial shoulder problems at some point during the season. Of those, 12 players reported them less than five times. The average OSTRC-02 severity score was 7.58 out of 100 (95% CI 5.31-9.84, range 0-31). Forty-eight percent of the participants had an average OSTRC-O2 severity score <5 and 21% <1. The average PSL rated by players was 4.1/10 (95% CI 3.68-4.40, range 1.5-7.5).
Pre-season Measurements and their Association with the OSTRC-O2 Results
The average pre-season ER/IR ratio and the average absolute peak values for ER, IR and IMTP strength and TRP can be found in Table 2. The only strength variable that significantly correlated with OSTRC-O2 prevalence of shoulder problems was pre-season ER strength (rs = -0.34, p = 0.029). No significant association was found between any of the pre-season measurements and the average OSTRC-02 severity score (rs range: -0.22 to -0.11; p values range: 0.16 to 0.51) or between the pre-season measurement and prevalence of substantial shoulder problems (rs range: -0.01 to 0.12, p values range: 0.44 to 0.96).
Influence of Pre-season Measurements on the Association Between PSL and the OSTRC-O2 Severity Score
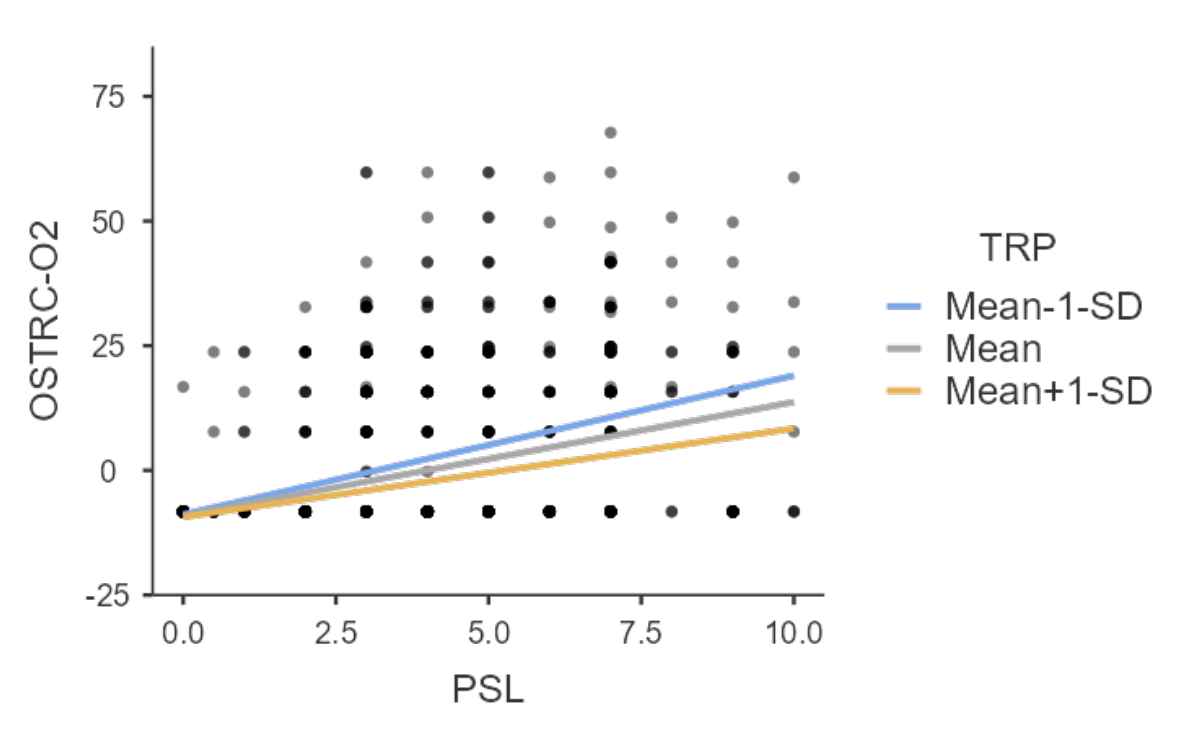
The mixed model ANOVA showed a main effect between the PSL and the OSTRC-O2 severity score (p<0.001). With higher PSL, a higher OSTRC-O2 severity score was observed. An interaction was found between the PSL and pre-season TRP in terms of their influence on the OSTRC-O2 severity score (p=0.017). With higher PSL, a higher OSTRC-O2 severity score was observed among players with pre-season TRP more than one standard deviation (SD) below the group’s mean. Conversely, with higher PSL, the OSTRC-O2 severity score was lower for players with greater pre-season TRP (Figure 5).

DISCUSSION
The main findings of this study indicate that the relationship between PSL and severity of shoulder problems through a regular season may be influenced by TRP, as low pre-season TRP might make the throwing shoulder more vulnerable for higher PSL during a season. Conversely, the findings indicate as well that high pre-season TRP might have a protective effect on the throwing shoulder when the PSL is high. A weak and significant negative correlation was also found between pre-season ER strength and the OSTRC-O2 prevalence of shoulder problems. This is, to the author’s knowledge, the first prospective study that shows that low pre-season TRP is linked to high severity of shoulder problems in handball players as the PSL is increased during the handball season.
Self-reported Shoulder Problems and PSL
The overall average OSTRC-O2 severity score of 7.58 is considerably lower than that of 29 and 35 (intervention and control group, respectively) reported by Andersson et. al.4 The group average prevalence of shoulder problems was 27%, which closely aligns with the 28% reported by Clarsen et al.3 but was higher compared to Andersson et al. who reported an average prevalence of 17% and 23% for their intervention and control group, respectively.4 The intervention group in the study by Andersson et al. had participated in a shoulder exercise program throughout the season aiming at reduced prevalence of shoulder problems which might explain the lower prevalence compared to results presented here.4 The group prevalence of substantial shoulder problems in this study was 4%, which is notably lower than the 12% reported by Clarsen et al.3 but similar with those found by Andersson et al.4
This is the first study to use the modified Borg rate of perceived exertion scale to monitor PSL in throwing athlete so no direct comparison to other studies is available but the average PSL throughout the season was rated 4/10 or “somewhat hard”.28 The authors of the “2022 Bern Consensus Statement on Shoulder Injury Prevention, Rehabilitation, and Return to Sport for Athletes at All Participation Levels” were not able to come to an agreement about whether monitoring internal vs external load was more important for risk or injury management for shoulder injuries.20 Monitoring factors like the number of throws, type of throws or throwing velocity is not practical because of the chaotic nature and unpredictability of the game of handball. In contrast, internal measures like the modified Borg rate of perceived exertion scale offer a simple but useful way to monitor PSL for handball players.
Pre-season Measurements and their Association with the OSTRC-O2 Results
The negative correlation found between the pre-season ER strength and the OSTRC-O2 prevalence of shoulder problems is consistent with previous studies linking reduced ER strength to shoulder problems in handball players.1,3,7 The angular velocity of the shoulder IR during a handball jump throw has been measured at 5039 °/s which underscores the importance of ER strength to absorb the load during the deceleration phase.29
The pre-season ER/IR shoulder strength ratio of 0.94 is higher than the cut off values of 0.75 and 0.89 that have been used to identify youth and adult handball players at increased risk of sustaining a shoulder injury.1,8,26,30 Moreover, the pre-season ER and IR absolute strength values were higher by more than 5 kg than the aforementioned reference values for adult handball players and pre-pitching ER strength in collegiate club baseball pitchers.30,31 This shows that this cohort as a whole had high shoulder strength, particularly for ER, at pre-season. These high strength values may reflect participants´ greater fatigue tolerance as ER strength measures have been shown to decrease immediately after intense throwing.31 Players with high ER strength may therefore be able to tolerate more throwing load before fatiguing which might have a protective effect for overuse injuries.
This is the first study to use the IMTP to measure lower body strength in handball players, so no direct comparison is available. The pre-season IMTP PF in this study was higher by roughly 800 N than PF values reported for 33 senior male professional rugby players and higher by more than 200 N than PF values reported for u21 Academy rugby players,32,33 indicating high levels of lower body strength in this group of participants. High levels of lower body strength likely increase the athletes´ ability to utilize the more proximal segments in the kinetic chain during the throwing motion. Utilization of proximal segments might have a protective effect on the throwing shoulder as efficient force transmission from the more proximal segments to the distal segments has been shown to be very important for the throwing motion.14,16,17
Exercise interventions aimed at preventing sport injuries highlight the effectiveness of strength training in reducing overuse injuries in sports by nearly half.34 The high ER/IR ratio and high absolute ER strength, IR strength and IMTP PF reported here might therefore explain the low average OSTRC-O2 severity score, low prevalence of substantial shoulder problems and lack of correlation between the pre-season measurement and the OSTRC-O2 severity score and prevalence of substantial shoulder problems.
Influence of Pre-season Measurements on the Association Between PSL and the OSTRC-O2 Severity Score
The influence of PSL on the OSTRC-O2 severity score throughout the season was affected, at least to an extent, by the pre-season TRP. These results are consistent with the previous findings showing an exacerbated effect of an increase in handball load on shoulder injury rate in players with low ER strength and scapular dyskinesis.8
The interaction between PSL and pre-season TRP in terms of their influence on the OSTRC-O2 severity score indicates the importance of the kinetic chain for shoulder health as the TR is believed to play a significant role in energy transfer to the throwing arm.35 A study on baseball pitchers showed that professional pitchers rotated their trunk significantly later within the pitching cycle compared to lower-level pitchers and had lower shoulder IR torque during throwing.36 Authors have speculated that the lower shoulder IR torque might be a function of that later trunk rotation timing, which makes professional pitcher able to use effective transfer of momentum from the larger, more proximal segments in a more efficient way as explained by the “proximal to distal sequence”.16,36 Hence, handball players with more TRP may need less time to generate the rotational energy needed for throwing. They may thereby be able to rotate the trunk later during the throwing motion and consequently minimize the load placed on the shoulder. In contrast, to make up for lower TRP, or due to fatigue, players with lower TRP might initiate the TR earlier, causing higher contribution from the distal segments for throwing and lead to increased load on the shoulder. These speculations, however, need to be investigated further.
This is the first study to use the seated TR test to measure TRP in any throwing athletes, so no direct comparison is available. No cut-off score calculation was done in the reliability analysis, so whether players with pre-season TRP one SD below the group´s mean really had a TRP deficit remains a speculation. However, the MDD90 for the test was 12.03 and the SD for the group´s mean was 12.3. The difference can therefore be considered a meaningful magnitude of TRP. As there was a weaker relationship between the PSL and the OSTRC-O2 severity score for players with TRP one SD above the mean, higher TRP can be considered to have a protective effect for shoulder problems. Further research is needed to investigate more detailed TRP reference values and appropriate cut-off scores in handball players. Until then our version can serve as a comparison for future research using the same testing and calculation methods.
Limitations and Methodological Considerations
The main limitation in this study is a small sample size which reduces statistical power. Controlling the participants´ training load and intensity in the days leading up to the pre-season measurements was not feasible as each team had its own pre-season training schedule. Participants were allowed to make appointments for data collection when convenient, regardless of their training schedule. Therefore, some may have been fatigued, which might have influenced their capacity to generate maximum force and power during data collection. Some players reported mild discomfort during the ER strength measurements which might have influenced the absolute strength values. However, it is common for handball players to continue to throw despite mild discomfort3,4 and as those particular players did not indicate that this mild discomfort limited their ability to exert maximum force during testing, these values were included in the pre-season data analysis of the player´s shoulder profile. The shoulder isometric strength measurements done by Cools et. al, used for comparison earlier,30 were performed in a sitting position with the shoulder in 90° of abduction and neutral rotation. In this study the shoulder strength was measured in supine position while maintaining the same neutral rotation at the shoulder. Different test positions have been used in research studies1,3,8,9,26,30 which may influence the outcome, so direct comparisons need to be made with that in mind. Despite different measurement positions the pre-season ER/IR ratio in this study was similar to the reference values for male handball players reported by Cools et. al.30
The OSTRC-O2 questionnaire and the PSL ratings inquired about the players’ subjective experience of shoulder problems and PSL over the preceding seven days, which introduces potential recall bias. Finally, the natural variation in the training and match load through the season might have had a lowering effect on the average OSTRC-O2 severity score, prevalence of shoulder problems and the PSL, but because of the total length of the follow up (31 weeks) that effect, if any, is believed to be minimal. Only one participant reported an acute injury to the shoulder during the season which influenced the average OSTRC-O2 score and the prevalence of shoulder problems for that player. The overall score for that player was <8 so the effect of that acute injury on the overall score is believed to be minimal.
CONCLUSION
The results indicate that the overall high fitness state in this group of handball players might have had a protective effect on shoulder problems. However, while the results support the importance of TRP and ER shoulder strength in relation to shoulder problems in handball players, they also highlight the influence of shoulder load due to participation. Professionals working with handball players should monitor the PSL of their players and consider whether the key factor in maintaining a healthy shoulder might be to look beyond the shoulder.
Conflict of Interest
The authors declare no conflict of interest. The conduct of this study was approved by the National Bioethics Committee of Iceland and funded by the University of Iceland Research Fund.
Acknowledgement
Dr. Thorarinn Sveinsson for his assistance during the statistical analysis.