INTRODUCTION
Overuse injuries demonstrate a high incidence in competitive swimmers.1 Studies on previous injuries in competitive swimmers revealed that shoulder and lumbar area injuries rank first and second overall, respectively.2–4 Injury histories are obtained and physical examination is conducted in swimming and various other sports to investigate the occurrence of injuries.2–7 The shoulder and lumbar injury rates per 1,000 practices (1,000 athlete exposures [AEs]) have been reported to be 0.51 and 0.24 for male and 0.29 and 0.60 for female swimmers, respectively.4 Specifically, shoulder impingement and joint capsular laxity, or lumbar intervertebral disc injuries are common causes of overuse injuries in swimmers.8 Strength training exercises for the rotator cuff, scapular stabilizers, and core muscle exercises have been demonstrated to be preventive for shoulder and lumbar injuries.8 Previous authors have examined the effects of exercise program prescriptions for competitive swimmers. They revealed a positive 14-year downward trend in disability occurrence in swimmers after an exercise program to prevent lumbar injury.2 However, other previous studies revealed that a six to eight-week shoulder injury prevention program caused physical function changes but no reduction in shoulder pain9,10 and that the effectiveness of exercise programs may differ between shoulder and lumbar injuries. Therefore, to further reduce injury risk, it is recommended that exercises tailored to individual injury histories and physical function be provided, in addition to general conditioning programs.
This study aimed to investigate the effects of implementing physical examination and providing an exercise program in reducing the occurrence of new shoulder and lumbar area injuries over one year. Moreover, the authors hypothesize that these efforts would decrease injury rates.
METHODS
Design
This cohort study investigated the effects of implementing exercise programs on competitive swimmers.
Participants
This study included 31 high school and college male swimmers. Swimmers who missed > one month of practice because of trauma or illness were excluded from this study. All participants were briefed under the declaration of Helsinki, and they signed written informed consent obtained by the team coach. For subjects under 18 years of age, written consent was obtained from a parent or guardian and the subject. The ethics committee of Hanna Central College of Rehabilitation approved this study (Registration number: HCCR-002).
Physical examination and exercise program
Competitive swimmers under go an examination of physical function (the physical examination) and an interview is completed regarding their their injury history. The first measurements were taken at the start of the season in September and repeated a year later in September. Both measurements were carried out by 11 physiotherapists and 2 athletic trainers. We attempt to provide an exercise program based on the results. The team’s physiotherapist designed the exercise program. Swimmers were interviewed during the first physical examination about their injuries in the previous year. An injury was considered “pain that lasted for > three weeks or that caused the patient to stop practicing.” Additionally, the hours of practice on weekdays and weekends were obtained.
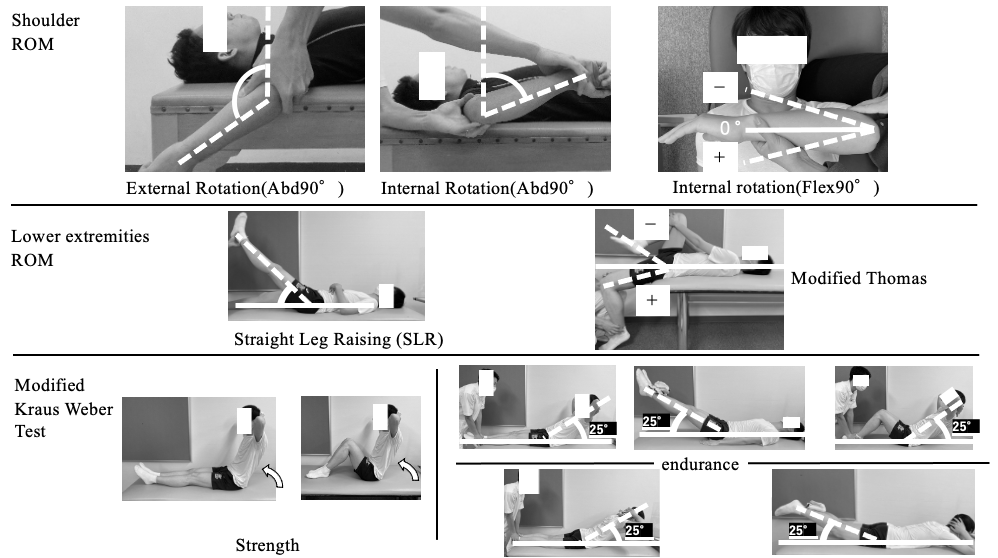
The physical examination involved passive measurements of the lower limb (straight leg raise [SLR] and modified Thomas test) range of motion (ROM) and trunk function (modified Kraus–Weber test [M-KWT]11) (Figure 1). The participants were placed in a supine position in the SLR ROM measurements. One of the measurers flexed the hip joint with the knee joint in extension while another examiner measured ROM. The participant was positioned supine with the lower limb out over the edge of the bed for the modified Thomas ROM measurement. The participant holds the lower limb not being measured at the abdomen with both hands. The hip joint was in maximum extension while a measurer held the knee of the lower limb at 90 degrees of flexion and another assessed hip joint extension ROM. A 10% of body weight was loaded on the head (two hands grasp the weights and set them on the back of the head) or the end of the lower extremity (wrapping weights around the feet) for measurement to further load the normal M-KWT.
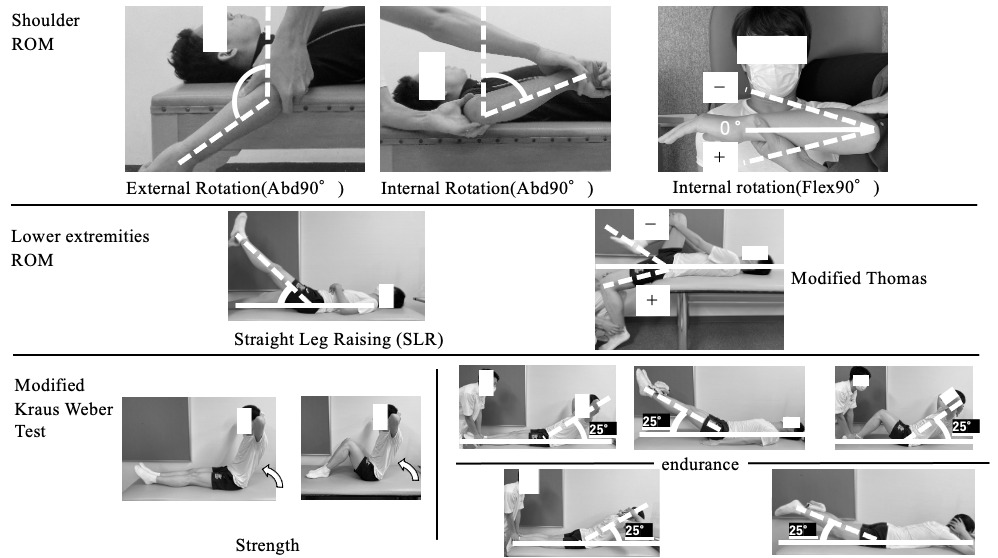
The M-KWT was performed with 10% of the body weight loading.
Passive shoulder ROM was measured: external rotation at 90° shoulder abduction (Abd90°ER), internal rotation at 90° shoulder abduction (Abd90°IR), and internal rotation at 90° shoulder flexion (Flex90°IR).
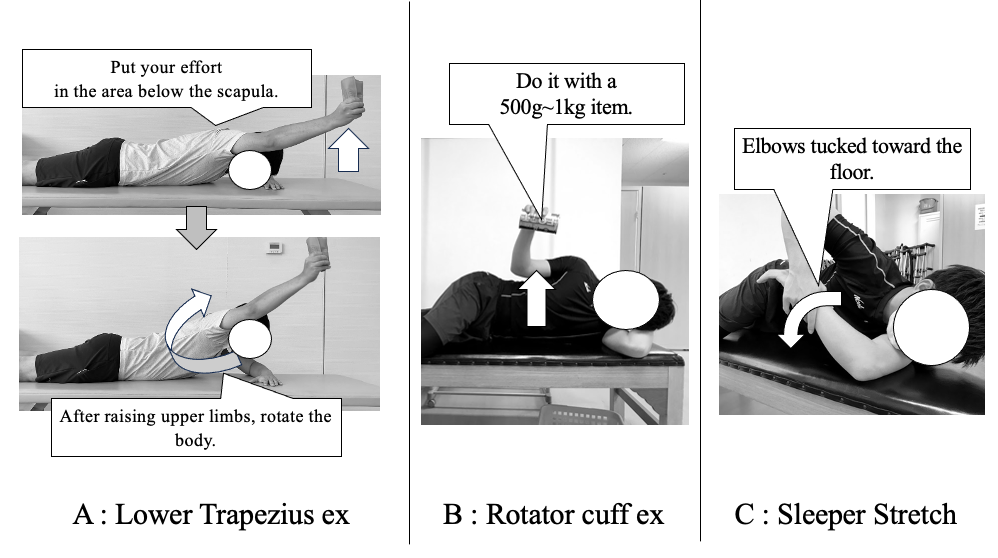
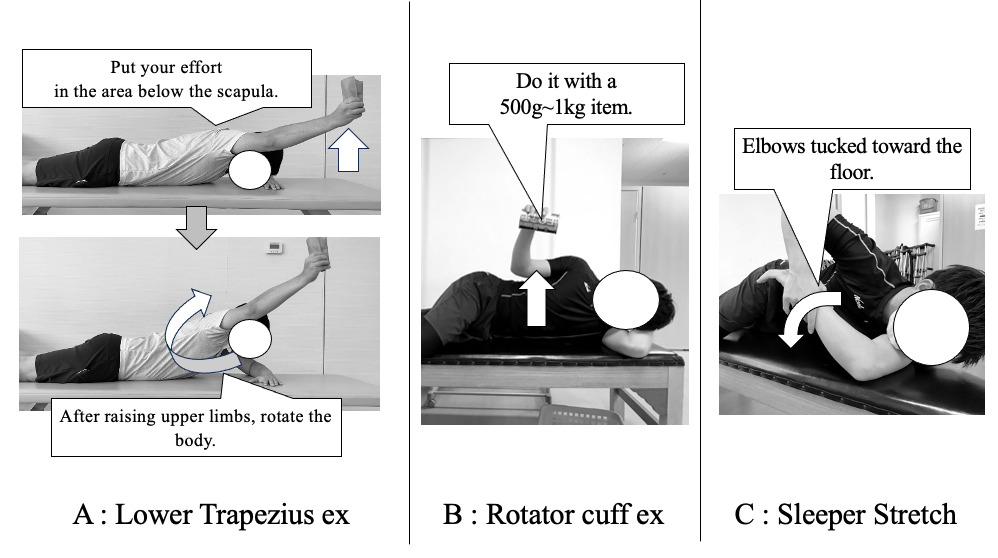
Written and verbally-instructed exercise programs were provided to improve the physical function of each swimmer based on the injury history and the measurement results of swimmers with an injury history. Details of the shoulder exercise (Figure 2) were as follows. (A) Lower trapezius strengthening exercises12 involved three sets of 10 with no load, twice a week, with a 1 kg weight for the second six months. (B) Rotator cuff exercises13 involved three sets of 20 repetitions at a low load (1 kg), twice a week. (C) Modified sleeper stretches,14 three sets 30-s after every practice.
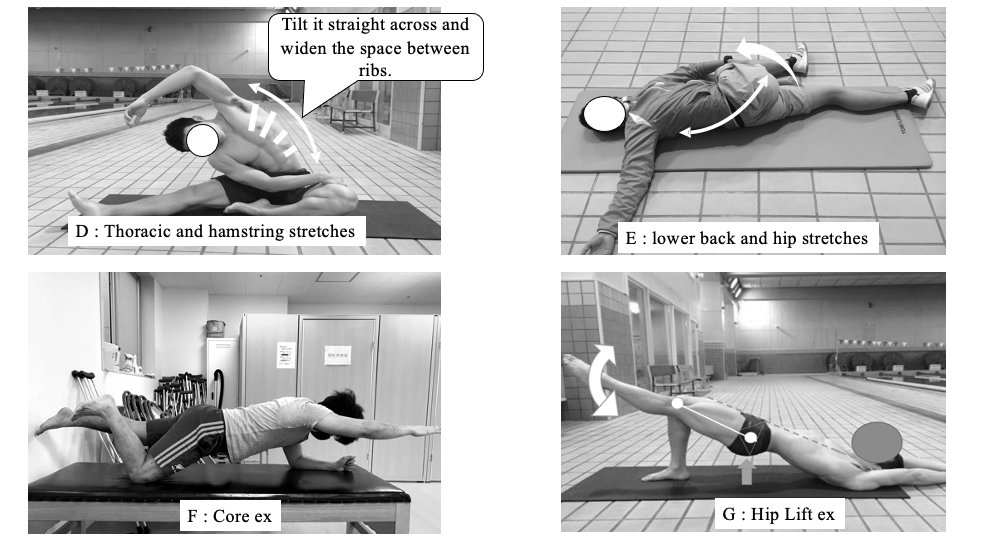
Details of the lumber exercise (Figure 3) are as follows: (D and E) Stretching of the spine and lower limb muscles, three 60-s held repetitions, with 30-s rest15 after every repetition. (F) Core exercise2 involved the front bridge while raising the upper and lower limbs on the diagonal 10 × 2 repetitions, twice a week. (G) Hip lift exercise2 involves moving the lifting leg up and down during a single limb bridge, 10 × 2 repetitions, twice a week. During the year, the participants were interviewed weekly for pain and fatigue, and the team’s physiotherapist monitored their exercise program. Physical examination was repeated after one year, and an injury history was obtained.

STATISTICAL METHODS
The injury rate was calculated using 1,000 player h (1,000 ph). Here, 1,000 ph was calculated by dividing the number of injuries by the total number of hours that the athlete participated in practice and multiplying by 1,000. The 95% confidence interval (CI) for 1,000 ph was simultaneously calculated. Swimmers with shoulder and lumbar disabilities at the first physical examination were compared to asymptomatic athletes on each item with the Mann–Whitney U-test, and one-year measurements were compared. EZR version 1.5416 was utilized for statistical processing. A post hoc power analysis was conducted when the p-value was <0.05. A difference was considered significant if the study had sufficient statistical power (1-b ≧ 0.8).
RESULTS
Injury rate
The mean age of the participants was 17.0 ± 1.1 years, with a mean height of 172.5 ± 5.2 cm and a mean weight of 66.0 ± 7.4 kg. Table 1 presents the number of injuries and 1,000 ph (95%CI) results. The shoulder exhibited 1,000 ph of 0.32 (0.13–0.50) and 0.05 (0.00–0.12) at the first examination and one year thereafter, respectively. Swimmers who reported shoulder injuries in the prior year at the first examination demonstrated no shoulder injuries in the following year. The lumbar area demonstrated 1,000 ph of 0.16 (0.03–0.28) and 0.03 (0.00–0.07) for the first examination and one year thereafter, respectively. The six swimmers with lumbar injuries reported no recurrences at the first examination, but one of the remaining 25 suffered a new injury.
Comparison of each measured parameter (the shoulder and lumbar area)
Swimmers who experienced shoulder pain at the first examination (n = 12) demonstrated a lower ROM of Flex90°IR (p = 0.003) and higher Abd90°ER (p = 0.034) compared to those without shoulder pain (n = 19). Post hoc power analysis revealed that Flex90°IR had high statistical power and was significantly different. All parameters exhibited no significant differences after one year (Table 2). The swimmers with lumbar injury at the first examination (n = 6) exhibited no significant difference in lower limb ROM and M-KWT compared with those without lumbar injury (n = 25), and the same was true after one year (Table 3).
DISCUSSION
This study consisted of the utilization of a physical examination and subsequent prescription of an exercise program based on the swimmers’ injury history and the measurement results of those with an injury history. The results revealed decreased shoulder and back injuries and improved Flex90°IR after one year.
Physical examination and exercise program
A previous study on longitudinal survey implementation and disability incidence in competitive swimmers revealed no changes in disability incidence in males but decreased incidence in females.4 However, Kerr’s study included injuries other than those in the shoulder and lumbar area, and the effects of physical examination on the lumbar and shoulder joints specifically remain unclear even after involving other sports. Longitudinal studies on swimmers undergoing medical check up (physical examination) and exercise programs have decreased lumbar injuries.2 However, 96% of swimmers have experienced shoulder pain at the end of the season, even when provided with a longitudinal examination and dryland exercise program provided by an athletic trainer.16 Some studies demonstrated that swimmers continue to practice even with lumbar or shoulder injuries if the injuries are minor,3 and swimmers do not consider minor injuries as important. However, preseason screening for shoulder ROM is useful in determining athletes at risk of disability,16 and the benefits of physical examination have been indicated. The current survey and interventions reduced the number of lumbar injuries from six to one and shoulder injuries from 12 to two within this cohort, with particularly favorable results for the shoulder. The provided intervention program was based on injury history findings and physical examination results, and carried out with oversight from the physiotherapist regarding exercise content. Furthermore, participants were interviewed weekly for pain and fatigue, and the physiotherapist monitored their exercise program. Introducing exercise only with physical examination or without physical evaluation of target athletes may be unlikely to decrease the occurrence of injury. The current results indicate that a physical examination performed to determine the problematic areas and continuous exercise guidance afterward decreased the incidence of injuries.
Decreased incidence of shoulder injury
The current study demonstrated that swimmers with shoulder pain at the first examination were characterized by decreased Flex90°IR ROM (Table 2). A previous study that investigated the ROM in swimmers with shoulder injuries revealed an external rotation ROM of <93° or >100° in the 90° shoulder abduction position as a predictor of shoulder disorders in swimmers with shoulder injuries.17 The median Abd90°ER ROM of the swimmers with shoulder disorders for the first time in this study was 101°, which is consistent with previous studies. However, the post hoc power analysis results revealed no significant difference between the two groups, and the incidence of disability decreased despite an increase in Abd90°ER ROM in both groups after one year. Factors, other than shoulder injury, may affect the magnitude of Abd90°ER ROM, as reports indicate that high-performance swimmers demonstrate greater Abd90°ER ROM18 and that competitive swimmers may also have acquired anterior shoulder tissue laxity.19 A previous study that investigated the shoulder internal rotation restriction in nonswimming athletes revealed that baseball players (pitchers) with glenohumeral internal rotation deficit are at approximately twice the risk of having a shoulder joint injury.20 Further, Takayama’s study reported reduced Flex90°IR ROM in swimmers with shoulder joint injuries.21 The Flex90°IR ROM may reflect posterior shoulder tightness. Posterior shoulder tightness may have caused the superior anterior displacement of the humeral head during shoulder flexion, thereby significantly increasing the contact pressure with soft tissues.22 Thus, improved internal rotation ROM may be associated with reduced incidence of shoulder joint disorders in swimmers.
The measured Flex90°IR position in this study is similar to that of the modified sleeper stretch position. Performance of the modified sleeper stretch has been associated with decreased tightness of the infraspinatus muscle which attaches to the posterior shoulder.14 Thus, swimmers with shoulder pain were instructed to perform modified sleeper stretch. Following a year-long modified sleeper stretch program, the shoulder pain group demonstrated significant improvements in Flex90°IR, and there were no significant differences between shoulder pain and the pain-free groups in one year later. A previous study revealed that four weeks of modified sleeper stretching reduced the stiffness of the infraspinatus muscle.14 Therefore, long-term application of modified sleeper stretches that improved posterior shoulder flexibility (similar to the previous study14) may have contributed to the reduced incidence of shoulder joint injuries.
Posterior shoulder musculature reduced endurance23 and lower muscle activity in the lower trapezius during the crawl and backstroke24 has also been described, which may contribute to shoulder injuries among swimmers. Therefore, participants were instructed to perform low load, high-frequency exercises for the lower trapezius and external rotator muscles of the shoulder. The provision of these exercises contributed to reduced shoulder joint injury after one year. Moreover, some studies reported that a three-week periscapular exercise prescription increased lower trapezius muscle thickness25 and decreased shoulder pain26 and that 16 weeks of training with the band elevated the external rotator muscle strength in competitive swimmers.27 These results indicate that exercises for the shoulder’s lower trapezius and external rotator muscles may help decrease the incidence of shoulder disorders.
Decreased incidence of lumbar injury
Cejudo et al. revealed that hamstring flexibility deficits in male soccer and basketball players are related to low back pain.28 Iliopsoas elasticity and lumbar kyphosis angle have been shown to be greater during in-water movements in competitive swimmers with low back pain.29 However, the physical examination findings indicated that no difference in straight leg raise or modified Thomas ROM was present in the lumbar injury group compared with the nonlumbar injury group. The oblique abdominal muscles and erector spinae are constantly contracted in the butterfly stroke,30 and the endurance of the trunk muscles would be related to low back pain. However, the current study revealed no difference in M-KWT in swimmers with or without lumbar injury. On the other hand, lumbar spondylolysis and facet joint pain are possible causes of back pain in swimmers.31 This is believed to be due to a position of spinal hyperextension, which requires dynamic movement of the trunk for repeated flexion and extension of the spine.31 Another factor may be the scapulothoracic region, as patients with recurrent low back pain in sports with lumbar spondylolysis exhibit decreased flexibility of the scapulothoracic region/thoracic cage.32 Further, elite diving athletes with low back pain demonstrated decreased scapulothoracic joint mobility.33 With these reports and guided by the exercise program2 used with the Japanese national team, the authors provided (1) thoracic stretching, (2) deep trunk muscle exercises (core stabilization), and (3) lower back and hip exercises. Hence, six swimmers who experienced back pain at the first examination reported no recurrence for one year, suggesting the effectiveness of exercise program based on the physical examination findings.
Limitation
One limitation of the current study is that a few of the measures were not consistent with the prescribed exercise program. The exercise program included strengthening muscle endurance exercises around the shoulder, but the physical examination did not include a strength or muscle endurance variable in the assessment. Because the measurements of the physical examination were biased toward mobility. In the future, investigating the association between force and injury in the upper and lower limbs and trunk using hand-held dynamometers will be necessary.
Authors have suggested that decreased posterior shoulder muscle endurance, including the periscapular muscles, is seen in swimmers with shoulder pain23 and increased numbers (~ 50%) of swimmers displaying scapular dyskinesis after exercise.34 Thus, a longitudinal study on shoulder muscle endurance is warranted. The posterior shoulder endurance test has been measured in competitive swimmers,23 and the authors aim to include this in future research. Further, the authors plan to conduct a longitudinal study on the mobility of the thoracic cage and deep trunk muscles to identify the effectiveness of the exercise program utilized in the current study for the lumbar region. Finally, the number of participants is small and no control group was established; thus, the authors would like to recruit more participants in the future. Additionally, conducting a survey that involves female athletes is imperative, as none were included among the participants in this study.
CONCLUSIONS
This study prescribed an exercise program to swimmers with shoulder injuries after undergoing physical examination and obtaining injury history. None of the 12 injured swimmers reported a history of shoulder injury recurrence, and none of the six injured swimmers exhibited a history of lumbar recurrence during the study period. These results indicate that using a prescribed exercise program subsequent to a physical examination reduces the incidence of injury over one year.