









Introduction
After ACLR, athletes often arrive a crossroads where they have “finished” their rehabilitation, but have not yet been cleared to return to sport. This commonly occurs due to insurance plan limitations, an inability to afford rehabilitation following the exhaustion of benefits, or self-discharge. Despite the abundance of evidence that suggests the importance of meeting specific return to play criteria, many athletes continue to exhibit strength deficits and poor results with functional testing including altered proprioception, impaired motor control and muscle recruitment, and heightened reliance on visual feedback.
Persistent efforts and countless time have been spent on research following ACLR, however the ability of an athlete to return to sport at their highest level of performance and reinjury rates continues to be a challenge to sports physical therapists.1–3 Ardern et al. reported that current return to sports rates in elite athletes following ACLR is 81% to any sport, 65% to their preinjury level, and only 55% to their previous competition level.1 Athletes following ACLR are at increased risk for reinjury with documented rates as high as 30%, 21% occurring in the contralateral limb and 9% in the ipsilateral limb.3 Although time is not the only factor in return to sport decision making, delaying return until nine months after surgery can significantly reduce the reinjury rate by 51%4 and athletes that return prior to nine months post-operatively are at approximately a seven-fold increased rate of sustaining a second ACL injury.5 Strength continues to be a long-term concern following ACLR, with reports indicating that deficits in the hip, knee, and ankle musculature can persist for two-plus years following surgery.6,7 Deficits in deceleration performance and landing/jumping, both vital to reducing risk of ACL injury, may persiste for years following ACLR. Paterno et al demonstrated that biomechanical asymmetries exist during both landing and takeoff from a drop vertical jump two-plus years following ACLR.8 Asymmetries are also present during a 90-degree change of direction task in individuals following ACLR four-plus years following injury, demonstrating the need to address these biomechanical asymmetries in the later stages of rehab.9 Continued rehabilitation into the advanced/return to performance phases of ACL reconstruction is essential, however this begs the question; “Is there something missing from the traditional approach of ACL rehabiliation?”
While current training and testing metrics often fail to replicate the dynamic and unpredictable nature of sports, neurocognitive training offers a promising solution. Part 1 of this commentary advocates for early and consistent integration of neurocognitive rehabilitation in patients following ACLR. Incorporating these principles throughout ACL rehabilitation can better simulate the athletic environment, thus reducing the risk of re-injury, improving athletes’ confidence, and ultimately bridging the gap between rehabilitation and performance.
The overall goal of rehabilitation following ACLR is to return athletes back to sport safely. Continued neurocognitive rehabilitation and training into the advanced phases may be one of the missing links which helps bridge that gap from return to sport and return to performance at greater than or equal to an athlete’s prior level of competition. The purpose of this clinical commentary is to offer strategies to implement neurocognitive training elements into the traditional ACLR rehabilitation (in weeks 9+) and review updated testing metrics that may better indicate an athletes readiness to return to competition.
Neurocognitive Techniques Applied to ACL Rehab
Neurocognitive deficits continue to persistent in the later stages of ACLR rehabilitation and have been shown to impact performance on traditional return to sport testing. Readiness to return to sport involves more than just the readiness of the musculoskeletal system and should also include psychological readiness, as well as adequate neuromuscular control. This is highlighted through the work by Swanik et al. found that amongst a cohort of NCAA athletes, those who sustained a non-contact ACL injury demonstrated slower reaction time, processing speed, and performed worse on verbal and visual memory tasks on IMPACT testing.10 Silvers-Granelli et al. demonstrated that in Division I and II men’s collegiate soccer players (1,500+ athletes), a warmup consisting of neuromuscular control and technique resulted in a reduction of injury rates by 46.1% and decreased time loss to injury by 28.6% in the competitive male collegiate soccer players.11 This data illustrates the importance of the continuation of neuromuscular/neurocognitive training into the advanced stages of ACLR rehabilitation and even as the athletes have been cleared for full competition to help minimize the risk of reinjury.
Simon et al. demonstrated that the addition of a neurocognitive and unanticipatory component to the traditional hop test series resulted in a significant difference in performance and may improve functional return to sport testing.12 This was further described by Smith et al. who demonstrated that reactive agility tasks that incorporate aspects of visual search, reactive decision making, working memory, and pathfinding, as well as the incorporation of visual perturbation resulted in a performance deficit.13
The authors propose that the traditional rehabilitation approach post ACLR, including the advanced stages progressing towards return to performance, should include increased emphasis on the neuroplastic, cognitive, and visual-motor capabilities that are impacted following injury to better prepare athletes for the chaotic nature of the sporting environment.
ACL Rehabilitation - Advanced Phase (Weeks 9-16)
Part 1 of this clinical commentary, Optimizing Recovery in the Acute Post-Operative Phase, set the stage for goals to be achieved prior to starting this phase of rehabilitation. The advanced phase of ACLR rehabilitation focuses on traditional goals by continuing to restore full knee flexion PROM (heel to glute) and progressing the intensity of a strength training program (focusing on both double and single leg exercises). Additonally, the authors suggest implementing neuromuscular control drills which specifically target deficits that are common following ACLR. During this phase individuals may transition towards low level plyos (i.e. variety of double and single leg pogo hops) prior to a return to running progression. This progression will better prepare the athlete for the demands of running and assess their ability to generate and accept load. Lastly it is essential to begin assessing an athlete’s ability to decelerate because they must be able to “apply the brakes” (deceleration) prior to working on “hitting the gas” (acceleration).
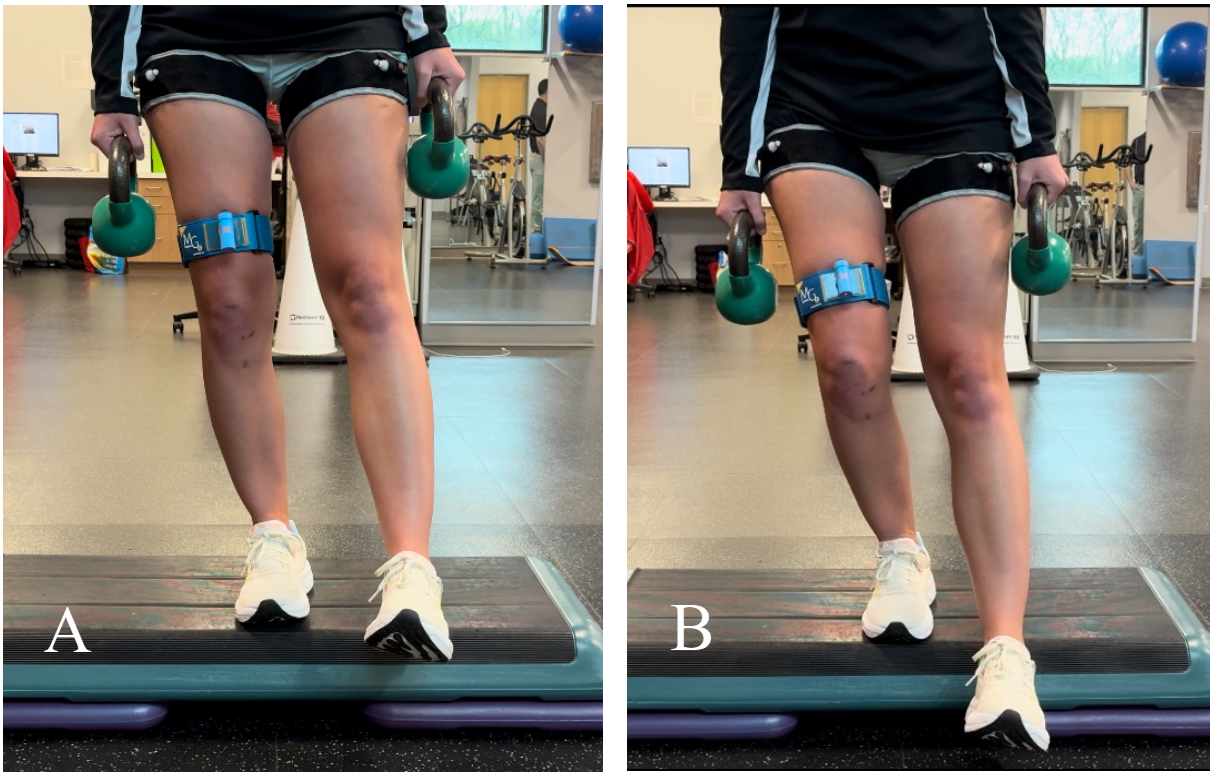
In an effort to restore strength, blood flow restriction training can be an excellent adjunct as it respects the healing process by minimizing load on the tissue during this phase. It can be used in combination with heavy resistance training, to promote increased muscular strength and hypertrophy.14 Blood flow restriction can be coupled with neuromuscular control drills (such as an anterior step down) which are crucial prior to progressing towards higher level activities. The authors suggest utilizing a laser light system during exercise which provides an externally focused visual feedback mechanism to ensure proper lower limb alignment (Figure 1).
_to_optimize_.png)
Once satisfactory mechanics, neuromuscular control, and strength (>65% of the contralateral limb via isokinetic or isometric hand held dynamometer) has been demonstrated, a gradual return to running progression may begin using the Alter-G or an underwater treadmill. This typically occurs at 10-12 weeks post-op, however the authors advise that objective criteria versus time alone should guide the decision as individuals who experience reactive symptoms during a return to running progression can experience significant setbacks.
Injury to the ACL often goes beyond injury to a soft tissue structure, resulting in joint damage and possibly contributing to early joint osteoarthritis. Bone bruising has been reported to occur in 98-100% of ACL tears.15,16 Byrd et al. assessed the prevalence of bone bruises in 208 patients (mean age: 23.8 years) who underwent ACL reconstruction with a median time from injury to MRI scan of 12 days.15 In this cohort, 59% of the athletes who suffered a non-contact injury with 98% (203/208) demonstrated evidence of a bone bruise, 79% at the medial tibial plateau, 83% in both the medial and lateral tibial plateau, and 46.6% demonstrating a bruise in all four locations (medial femoral condyle, lateral femoral condyle, medial tibial plateau, and lateral tibial plateau).15 This is important to consider in that it should guide the rehab professional towards a gradual return to impact progression in the advanced stages of rehab in order to preserve and maximize long term joint health.
Once the athlete demonstrates appropriate mechanics and tolerance through a gradual weight bearing progression, land-based running may begin typically around 14-16 weeks. The decision to return to running is based on a comprehensive evaluation by the rehabilitation specialist and is informed by the athlete’s ability to tolerate the functional progression without an increase in pain and swelling, while demonstrating good hip and knee control.
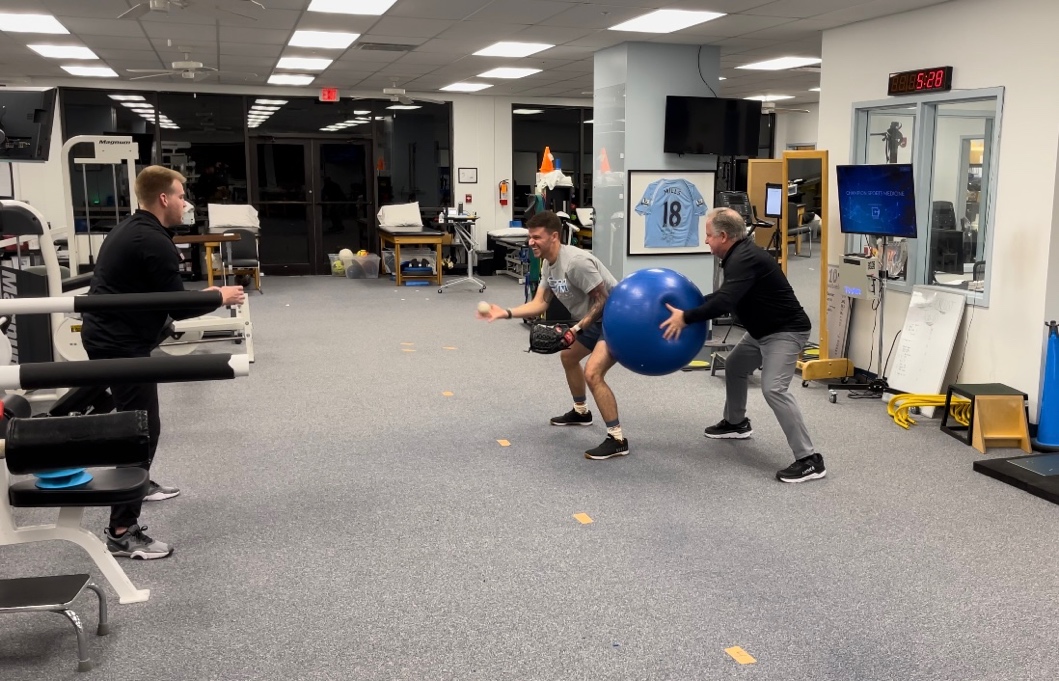
During this phase, athletes should be progressing more towards the associative phase of motor learning, with increased task complexity and focusing on generating neuromuscular solutions that minimize error without focusing attention on the movement alone. This may include increased emphasis on visual distraction and/or working memory as well as perturbation training during a dynamic exercise such as ball toss, colored lights, or counting (Figure 2). The goal should be training both cognitive and motor function in an interactive manner to meet the demands of each individual sport. Examples of exercises that can be utilized during the phase are further described in Table 1.
_single_leg_balance_on_rocker_board___external_focus_of_demand_s.jpeg)

.jpeg)
_neurocognitive_training_-_array_reactive_foot_fire_to_target_co.jpeg)
ACL Rehabilitation - Functional Sport Training Phase (Months 5-9)
During the functional sport training phase of ACLR rehabilitation the emphasis should be placed on continuing to progress athletes towards sport specific drills and later beginning to gradually progress towards return to practice participation. Athletes should be progressing towards the autonomous phase of motor learning performing multi-planar dynamic movements while simultaneously completing a high cognitively demanding challenge. Examples of exercises that can be utilized during the phase are further described in Table 2. By this point, athletes should have completed a return to straight line running progression and are continuing to progress plyometrics, agility drills, and sport specific training. Strength should not be forgotten at this stage, and athletes should be approaching 85-90% limb symmetry index (LSI) compared to their contralateral side. Overall, the goal of the functional sport training phase of ACLR rehabilitation should be to prepare athletes for the demands of sport by placing increased attention on reactive agility, multiplanar stability, power development, sprinting and jumping / landing capabilities.
_single_leg_rocker_board_balance_with_perturbations___dual_taski.jpeg)
_reactive_mirror_drill_with_lateral_slides.jpeg)


ACL Rehabilitation - Return to Performance (Months 9+)
Individuals entering this phase of rehabilitation will begin to participate in more advanced drills with the goal of progressing back into practice and later, competition. This phased approach to returning was proposed by the senior author in 2020.17 During the participation phase individuals are continuing to refine skills such as jumping, landing, single leg balance, and reaction time however it is imperative that they continue to be challenged. Figure 10 illustrates an individual performing a countermovement jump. They are given a variety of multi-step memory, counting, and verbal demands all while ensuring equal weight distribution is maintained. This can also be seen in Figure 11 where the individual has progressed from tradtional ladder drills. In this case they are given multiple commands, first to switch between two drills, occuring in two different planes of motion, second to change directions, and third to catch a ball with a specific hand. The goal is that the athlete can multitask without breaking stride and complete the cognitive challenge with minimal errors.
Once competent with these tasks in a clinic (closed) environment they can be returned to the practice (open) setting where sport specific progressions may take place. Communication among the entire team caring for the athlete are imperative as they may be spending more time with athletic trainers, strength and conditioning specialists, skills trainers, and coaches. The rehab provider must continue to ensure neurocognitive challenges are being imparted to the patient to combat potential long lasting deficits.
.png)
_reactive_agility_ladders___dual_tasking_and_external_focus_of_.jpeg)
ACL Rehabilitation – Recommendations for Testing
Deciding when to return to sport is a complex, multifactorial, and multidisciplinary decision not taken in isolation at the end of the recovery and rehabilitation process, but instead should be viewed as a continuum, paralleled with recovery and rehabilitation.18 Athletes’ struggles to return to play can be attributed to issues with the current return to sport testing procedures, or lack thereof. In a 2011 systematic review of 264 articles, Noyes et al indicated that 40% (105) of studies discussing return to athletics following primary ACL reconstruction failed to provide any return to play criteria before sending ACL athletes back to sport.19 Of those that did provide criteria 32% (82) used time alone, while 15% (40) used time and subjective criteria. Only 13% (55) used objective criteria, without any consensus or agreement on the “best” tests. The importance of specific objective criteria, described by Kyritsis et al. as not achieving six specific markers (quadriceps deficit < 10% on isokinetic at 60°/s, LSI Single Hop >90%, LSI Triple Hop >90%, LSI Triple Crossover Hop >90%, completion of on-field drills, and a Running T-Test <11s) led to a four-fold increase in risk of re-rupture.20
Performing objective testing prior to returning athletes to sport is pivotal in ensuring positive outcomes, however, the authors suggest that there should be updates to our current practices. The criteria mentioned above is a good starting point, however flaws exist. The current tests place emphasis on limb symmetry and fail to respect the bilateral deficits that commonly occur following injury, otherwise known as the “flat tire phenomenon”. This leads clinicians on a chase to achieve a moving target that is still below that of the athletes level of function prior to injury. More importantly these tests as traditionally completed are predictable in nature, which allows individuals the ability to practice the skill independently and may reflect a learning effect. Lastly it has been reported12 that there is a decrease in performance during functional tasks when a cognitive load is applied, and thus the authors suggest that modification be made to traditional hop testing when trying to replicate the demands of sport.
Based on the available knowledge pertaining to neurocognitive changes following ACLR a shift has begun related to return to sport testing. Schnittjer et al. aimed to understand how functional tasks were affected by cognitive challenge.21 They had individuals perform jump landing tasks under three conditions: no dual-task, “easy” dual-task, and “hard” dual-task. The authors concluded that with each increasing demand, movement quality was negatively affected.
Millikan et al. aimed to develop four clinical neurocognitive single-leg (SL) hop tests.22 Similarly Farraye et al. developed and tested the reliability of a Visual-Cognitive Reactive Triple Hop Test, and demonstrated excellent reliability for visual-cognitive reaction and moderate reliability for reaction time however, the maximum hop distance was significantly lower by 8.17%.23
Differences have also been described when comparing preplanned versus reactive agility or change of directions drills. Serpell et al. demonstrated a difference in mean reaction time between elite and subelite groups which they contributed to perceptual skills and/or reaction ability.24 When performing a reactive deceleration change of direction task in response to either a visual stimulus (i.e. light system)25 or an external object (i.e. soccer ball),26 changes were noted in a reduction of braking force at the penultimate step with an increase during the final step25 as well as a greater display of “high-risk” movement patterns.26 Both Grooms et al. and Wilk et al. have proposed frameworks for combining neurocognitive and functional tests to help improve return to sport decision making following ACLR.27,28 Grooms et al. also aimed to understand the reliance on neurocognitive demand as it pertains to functional performance in an effort to improve return to play decisions following ACL reconstruction.27 They proposed the performance of four highly reliable tests both with and without neurocognitive augmentation in order assess for neurocognitive reliance.

Figure 12. Reactive Single Limb Cross Over Hop for Distance Test. The participant stands on one foot and hops outward – as the participant jumps, they are instructed which foot to land on and they must cross over the center tape. They will then complete the sequence by completing two more cross over hops on the same limb.
ACL Rehabilitation – Preventative Programs
Even following return to sport, research has demonstrated the importance of continuing a risk reduction program both in the preseason and throughout the season to help minimize the risk of reinjury. These preventative programs (Sportsmetrics Program, FIFA 11, FIFA 11+, and the Prevent Injury and Enhance Performance [PEP]) have shown that a session consisting of neuromuscular training including stretching, strengthening, plyometrics, and agility may have a direct benefit in minimizing the number of ACL injuries in male and female athletes.29–32 The results of a recent systematic review indicate that a comprehensive program which includes plyometrics, strengthening, and neuromuscular training exercises led to a 50% reduction in the risk for all ACL injuries and 67% reduction for non-contact ACL injuries in female athletes.33 However these reviews also indicate an improvement in performance amongst organizations which were compliant to preventative programs due to the ability to keep more players healthy. The authors suggest that when educating individuals that they not only promote the risk of injury reduction, but additionally the improvement in performance to improve compliance with these programs.
Future Directions and Implications
Further research must continue to test and implement reactive return to sport testing. As new tests develop clinicians must continue to ensure reliability and validity standards remain sufficient. Long term data collection and randomized control trials (RCTs) on athletes who have completed a reactive and neurocognitively challenged return to sport testing battery compared to traditional testing is needed to determine the effectiveness of such testing strategies regarding return to performance decisions and reinjury rates. Continued work is also needed to determine the impact on the uninvolved limb and whether or not neuromuscular training can help minimize the risk of contralateral injury as well. The authors’ recommendation for all sports physical therapists, athletic trainers, and/or strength and conditioning specialists is to think of an ACL injury as more than just a musculoskeletal injury and to understand/appreciate the importance of “training the brain” in order to best prepare our athletes for the chaotic and unpredictable nature of the sporting environment they are returning to and testing accordingly.
Summary
Traditional ACLR rehabilitation has been well researched and progressed over the years, however the rates of return to prior level of performance and risk of reinjury continue to be less than optimal. It is important to understand that recovery following an ACL injury is not an isolated musculoskeletal issue, but also are accompanied by neuroplastic changes at the CNS. Recovery of the musculoskeletal impairments is only the minimum prerequisite for RTS, which does not fully ensure readiness to return. As rehab professionals, we gradually progress “chaos” from low to highly distractive environments to better prepare athletes for the demands of sport. Integrating neurocognitive challenges throughout the rehabilitation process, beginning during the acute post-operative phases and concluding with RTS testing, may allow clinicians to more confidently make decisions regarding returning individuals following ACLR to sports, not only at their same level of performance but at one that exceeds the level they were at prior to their injury.
Conflict of interest
The authors above are affliated with the organizations mentioned in this manuscript however there is no personal or financial gain from any of the organizations linked to this manuscript.
Kevin Wilk serves on the medical advisory board for BlazePods and receives educational grant from QuickBoard.