

Introduction
The iliopsoas muscle complex plays a critical role in hip flexion and is involved in various activities, from daily movement to athletic performance. The iliopsoas consists of the psoas major and iliacus muscles, converging to form the iliopsoas tendon, which inserts at the lesser trochanter of the femur. Dysfunction or pathology of the iliopsoas can lead to anterior hip pain, which is commonly seen in athletes, dancers, and individuals with hip overuse injuries.1 Disorders of the iliopsoas, such as tendinopathy, bursitis, and snapping hip syndrome, are common sources of anterior hip and groin pain, particularly among athletes and individuals engaged in repetitive hip flexion activities. Recently, it has been felt that the psoas major may be representative of whole-body skeletal muscle mass, and a decrease in its cross-sectional area may be associated with a loss of motor function.2–4
Traditional diagnostic modalities, such as magnetic resonance imaging (MRI), have limitations in accessibility and the ability to provide real-time, dynamic assessments. Diagnostic musculoskeletal ultrasound (MSK-US) is an excellent modality for evaluating the iliopsoas complex due to its accessibility, cost-effectiveness, and ability to offer dynamic evaluation. This imaging technique enables practitioners to assess the iliopsoas during movement, evaluate muscle and tendon morphology, and identify abnormalities that may be contributing to hip pain or dysfunction. The purpose of this article is to provide an in-depth review of the use of diagnostic MSK-US in evaluating the iliopsoas muscle on the anterior hip. It outlines the relevant anatomy, scanning protocols, interpretation of findings, and discusses common iliopsoas-related pathologies detectable via ultrasound.
Anatomy and Pathophysiology of the Iliopsoas
The iliopsoas is a complex muscle group that spans the lumbar spine to the anterior hip. The psoas major originates from the transverse processes and bodies of the T12 to L5 vertebrae, while the iliacus originates from the iliac fossa. Both muscles join to form the iliopsoas tendon, which passes deep to the inguinal ligament and inserts into the lesser trochanter of the femur. The iliopsoas bursa, the largest bursa in the body, is located between the iliopsoas muscle and the hip joint capsule, reducing friction during muscle movement. The iliopsoas functions primarily as a hip flexor and also plays a role in stabilizing the lumbar spine and pelvis during movement. Given its deep location and proximity to important neurovascular structures, accurate imaging is essential for identifying pathology.
Common pathologies of the iliopsoas include:
-
Iliopsoas Tendinopathy: Degenerative changes in the tendon due to repetitive overuse or acute injury.
-
Iliopsoas Bursitis: Inflammation of the iliopsoas bursa, often linked to overuse or mechanical irritation.
-
Snapping Hip Syndrome (Coxa Saltans): Audible and palpable snapping during hip movements, caused by iliopsoas tendon impingement. Causes can be either extra- or intra-articular. Extra- articular causes include iliopsoas tendon, iliofemoral ligament anteriorly and iliotibial band or gluteus maximus laterally. Intra-articular causes include labral tears, chondral defects and loose bodies.5–10
Advantages of MSK Ultrasound for Iliopsoas Evaluation
There are several advantages in using MSK-US to evaluate the iliopsoas in patients with anterior hip pain.
-
Dynamic Imaging: Allows visualization of the iliopsoas during active movement, aiding in the diagnosis of snapping hip syndrome.
-
Real-Time Guidance: Facilitates guided interventions such as injections or dry needling.
-
Soft-Tissue Differentiation: Provides high-resolution imaging of tendons, muscles, and bursae.
-
Cost-Effectiveness and Accessibility: Offers a less expensive and more readily available alternative to MRI.
Diagnostic MSK Ultrasound in Iliopsoas Evaluation
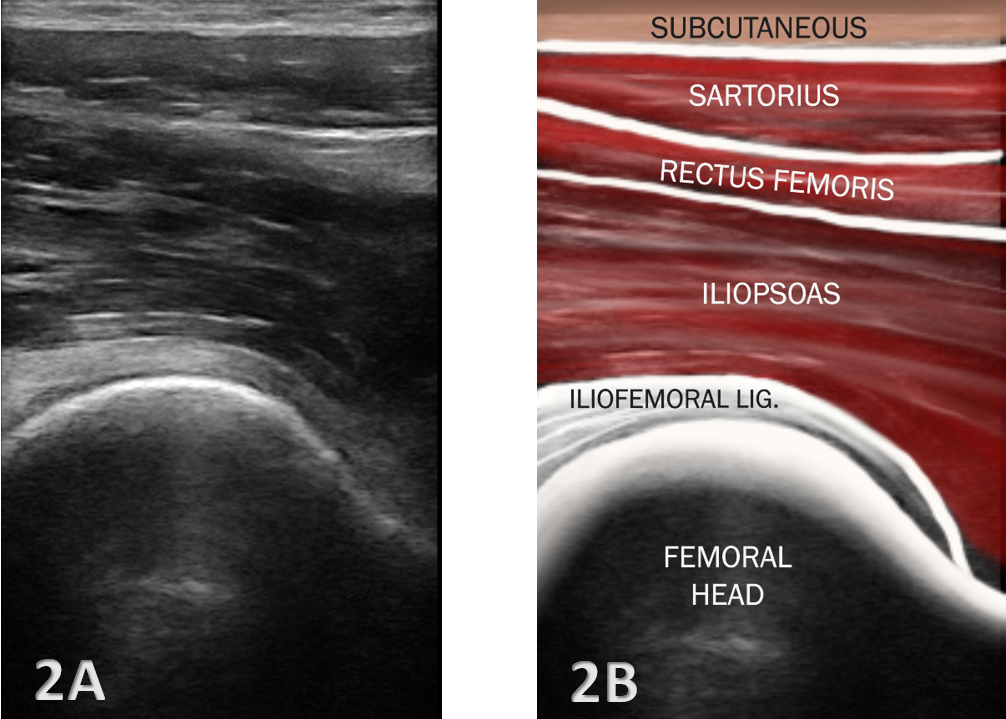
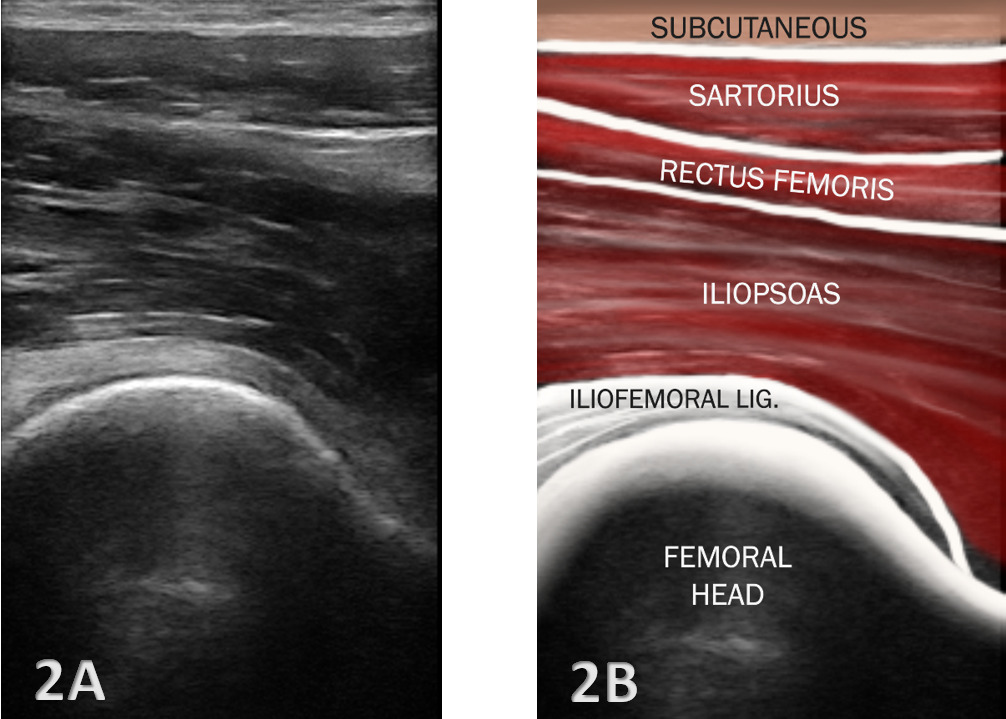
Proper patient positioning and transducer placement are crucial for visualizing the iliopsoas. The patient is typically positioned supine with the hip slightly externally rotated to improve access to the anterior hip region. A high-frequency linear transducer (7-12 MHz) is commonly used to visualize the iliopsoas complex. A curvilinear transducer may be necessary for deeper visualization.
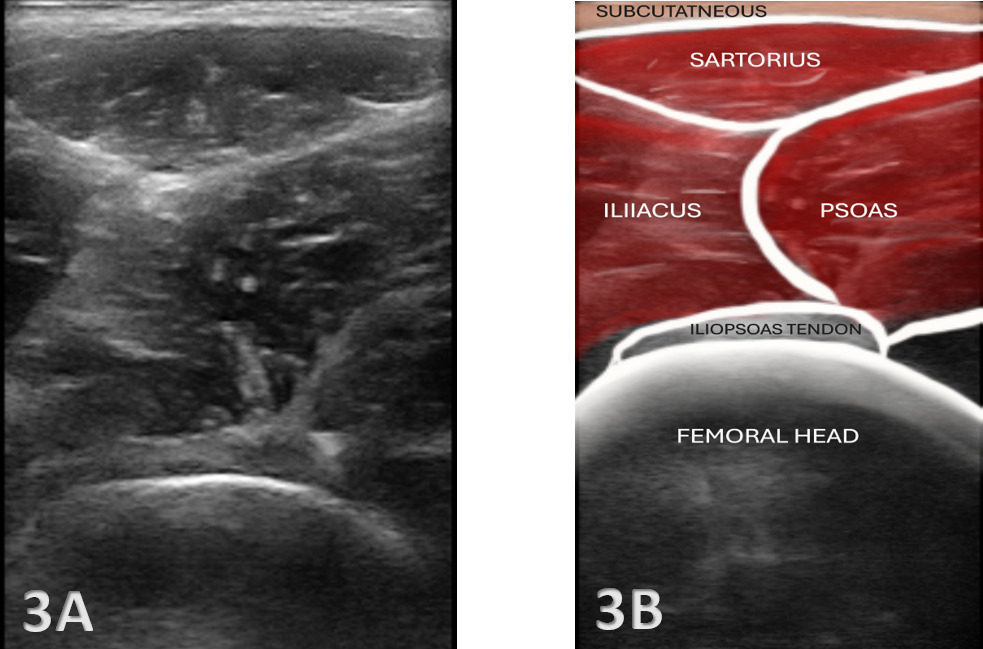
The transducer is placed parallel to the inguinal ligament, just below the anterior superior iliac spine (ASIS), to identify the iliacus muscle, psoas major, and iliopsoas tendon. The psoas muscle has historically been divided into three sections during ultrasound scanning: 1) upper section from origin of muscle to lower pole of the kidney, 2) mid- section from the lower pole of kidney to iliac crest, and 3) lower section from iliac crest to fusion with iliacus.11
The scanning protocol for the iliopsoas includes 2 planes of transducer placement.
-
Transverse Plane: The transducer is placed parallel to the inguinal ligament to identify the femoral vessels, then moved laterally to locate the iliopsoas muscle.
-
Longitudinal Plane: The transducer is aligned along the muscle fibers to assess the muscle and tendon continuity.
By gradually moving the transducer distally, the practitioner can follow the iliopsoas tendon as it passes beneath the inguinal ligament to its insertion at the lesser trochanter. Dynamic assessment, such as asking the patient to flex the hip against resistance, can help visualize tendon movement and identify snapping or other abnormalities. Doppler imaging may be utilized to assess hyperemia, which can indicate active inflammation.

Interpretation of Ultrasound Findings
-
Normal Anatomy: The iliopsoas muscle appears as a hypoechoic (darker) striated structure with internal echogenic (brighter) fibrous septa typical of a muscle.12 The tendon is more echogenic and is best visualized near its insertion on the lesser trochanter.
-
Dynamic Assessment: Active or passive movements can be performed to assess for snapping phenomena or to evaluate muscle function. MSK-US is ideally suited for dynamic assessment of muscles and tendons around the hip during motion and has been used to demonstrate correlation between abnormal iliopsoas tendon motion and painful snapping.13
Common Pathological Findings and Clinical Implications
MSK-US is highly effective in identifying a range of iliopsoas pathologies, including:
-
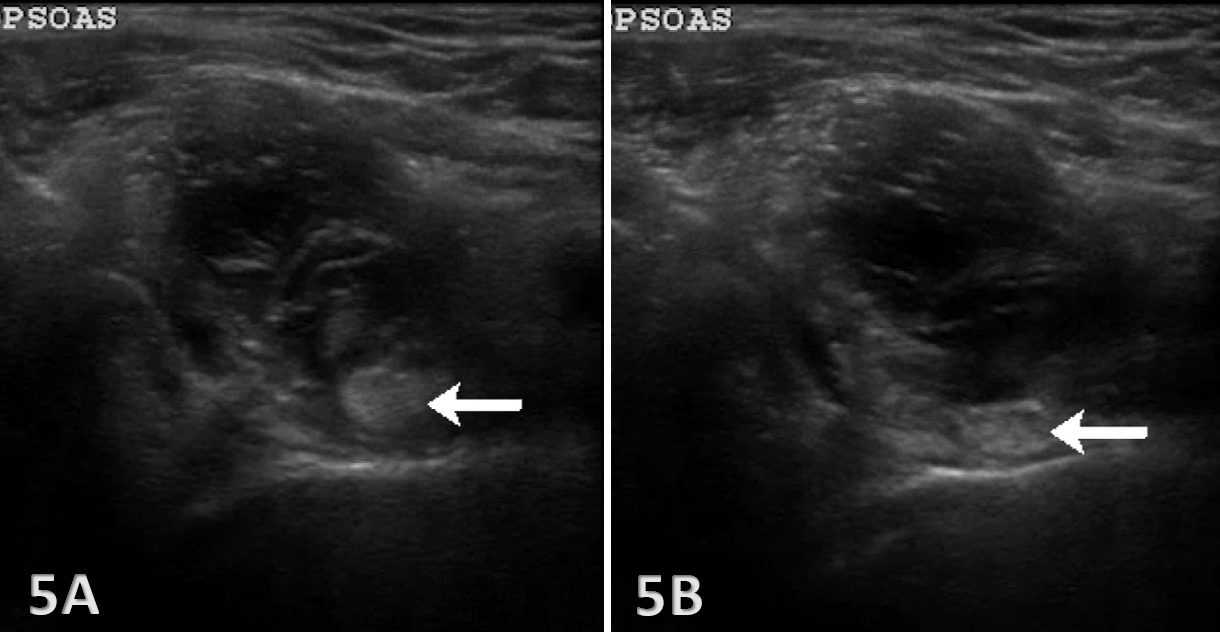
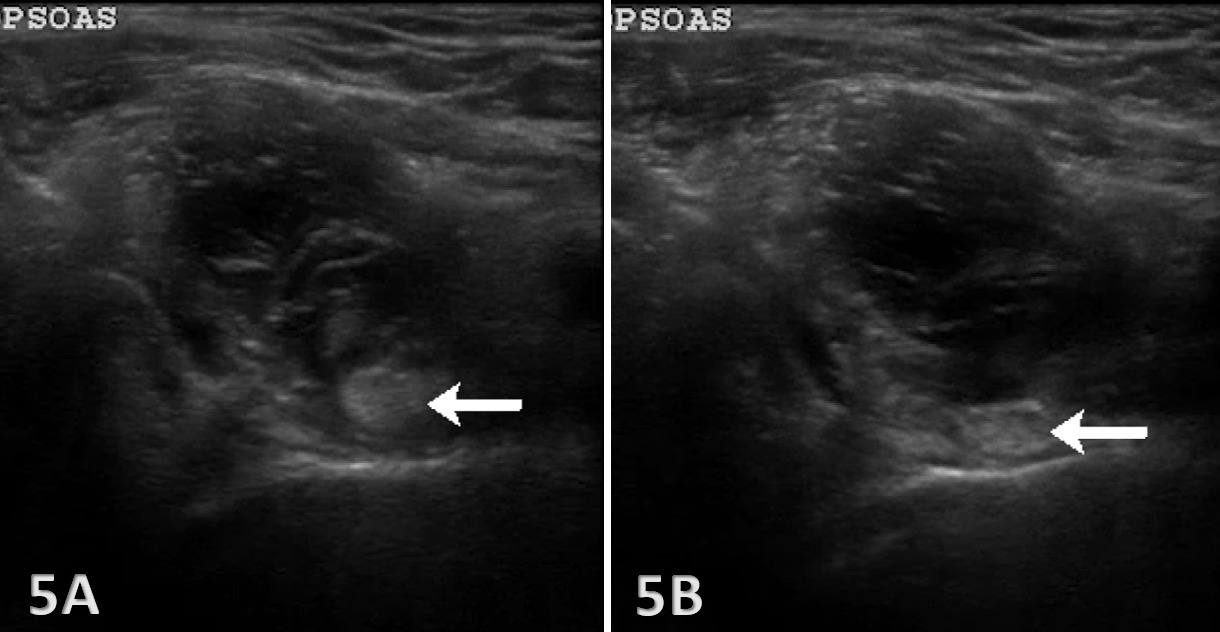
Tendinitis/Tendinopathy: Thickening of the iliopsoas tendon, hypoechoic changes, and increased Doppler signal may indicate tendinitis or tendinopathy. Clinical implications focus upon the dentification of tendinopathy which guides the rehabilitation focused on eccentric strengthening and load management.
-
Snapping Hip Syndrome: Dynamic ultrasound can capture the snapping of the iliopsoas tendon over the iliopectineal eminence, which is commonly seen in patients with internal snapping hip syndrome.5,6 The clinical implication for rehabilitation focuses on muscle flexibility, strength balance, and motor control exercises.
-
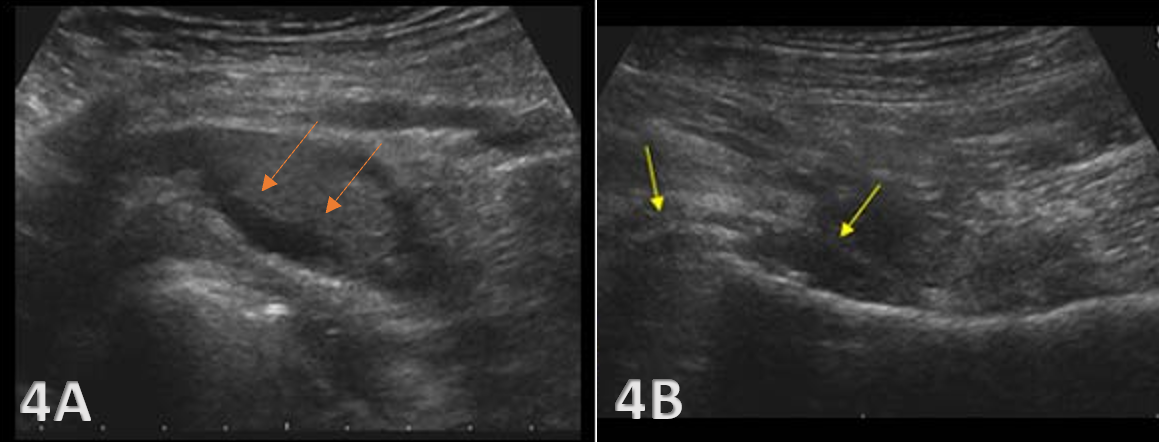
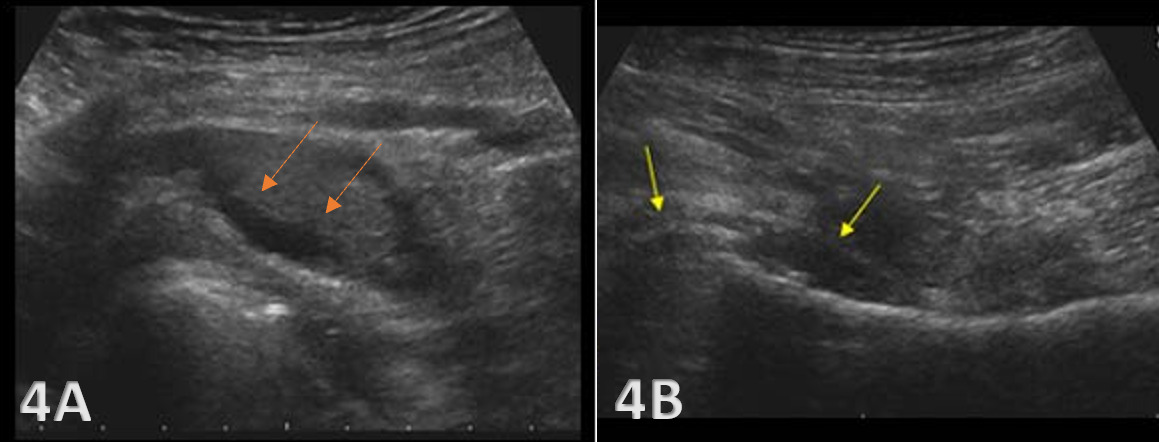
Bursitis: Iliopsoas bursitis may present as an anechoic or hypoechoic fluid collection between the iliopsoas tendon and the hip joint capsule. The bursa originates at the level of the femoral head and typically extends medially and possibly deep to the psoas major tendon and iliopsoas tendon.13 An iliopsoas bursitis will present as hip and groin pain. Bursal distensions rarely produce compression neuropathy of the femoral nerve; however, large distensions may extend into the pelvis along the iliacus muscle and may displace the pelvis structures.14 Management includes anti-inflammatory strategies and ultrasound-guided bursal injections.
-
Muscle Strain: Hypoechoic or mixed echogenic areas within the iliacus or psoas major may indicate muscle strain or partial tears, often associated with athletic overuse. Ultrasound findings can help tailor rehabilitation programs addressing muscle imbalances and joint mechanics. For example, changes in tendon thickness or echotexture can be tracked over time to assess the effectiveness of therapeutic interventions.
Clinical Implications for Rehabilitation
MSK-US findings should be integrated into a comprehensive rehabilitation plan including exercise, injections, and monitoring.
-
Targeted Interventions: Use guided injections for bursitis or tendinopathy and implement specific therapeutic exercises to address biomechanical deficits.
-
Progress Monitoring: Serial MSK-US assessments to evaluate the effectiveness of interventions.
-
Collaborative Care: Enhance interdisciplinary collaboration by providing detailed imaging reports to referring providers.
Conclusion
Diagnostic MSK-US is a powerful, dynamic imaging modality for evaluating the iliopsoas complex in patients with anterior hip pain. Its ability to provide real-time visualization of soft tissue structures, evaluate tendon movement, and identify pathological changes makes it an ideal tool for rehabilitation providers. By integrating MSK-US into clinical practice, practitioners can enhance the accuracy of diagnosis, tailor rehabilitation interventions, and improve patient outcomes in individuals with iliopsoas-related hip pain. Ultrasound-guided interventions, such as dry needling or corticosteroid injections, can be performed with increased accuracy under direct visualization. MSK-US also facilitates the monitoring of treatment progress. Rehabilitation providers can use ultrasound findings to make informed decisions about progression through stages of rehabilitation, return to sport, or modifications in exercise prescription. As technology advances, further research is warranted to expand MSK-US applications and refine diagnostic criteria, potentially transforming rehabilitation practices focused on hip pathologies.