INTRODUCTION
The menisci are critical structures that contribute to the function and health of the knee joint. Each meniscus is anchored to the tibia through an anterior and posterior root attachment within each compartment. Radial tears span across and sever the circumferential fibers of the meniscus and disrupt the meniscus’s native hoop stress. Hoop stress is the mechanism through which the meniscus manages axial joint load by creating an elastic containment at the joint that allows the meniscus to “give but not give way,” thus dispersing load. A radial tear located within one centimeter of the meniscus’s tibial attachment is referred to as a root tear1 and compromises the overall stability of the meniscus. Disruption of the circumferential fibers (and hoop stress) allows the meniscus adjacent to the tear to extrude outside of the joint space.2,3 Meniscal extrusion outside of the compartment reduces the contact area between the tibia and femur, normally buffered and broadened by the meniscus, leading to increased pressure on the articular cartilage. Notable extrusion creates an environment comparable to a total meniscectomy. A reduction of contact area by 40 to 75% may increase joint contact stresses by as much as 200 to 300%, transferring significant burden to the articular cartilage.4–6 To this end, accelerated osteoarthritis (OA) progression has been observed in association with meniscus root tears and meniscal extrusion among patients with no prior evidence of radiographic OA four years prior.7 More dramatic joint changes have also been observed over shorter time periods.8 For this reason, there is a justified sense of urgency in the orthopedic community to improve the management of this pathology.
The purpose of this clinical commentary is to explore clinical questions related to 1) posterior medial meniscus root epidemiology, 2) diagnosis and surgical management of posterior medial meniscus root tears, and 3) critical considerations for safe and effective post-operative rehabilitation.
EPIDEMIOLOGY
Meniscus root tears account for up to 10 to 21% of all meniscus tears.1,9 Posterior medial meniscus root (PMMR) tears comprise approximately 52% of all root tears and occur more commonly in females, typically in the 4th or 5th decade of life.9,10 These tears often occur with deep knee flexion or deep squatting with knee rotation.11 In general, tears of the PMMR are considered degenerative in nature with associated chondral defects observed 5.8 times more often with medial compared to lateral meniscus root tears.9 The posterior root of the medial meniscus is adjacent to the tibial attachment of the PCL and has been reported to be acutely injured with PCL tunnel drilling.12
DIAGNOSIS
Meniscus root tears are classified by tear location and tear pattern details. Type II tears, radial tears within 9 millimeters of the root attachment, are the most common.1 Tears at the posterior root attachments are more common at both the medial and lateral meniscus, perhaps related to lower loads to failure compared to the anterior root attachments.13,14
NON-OPERATIVE MANAGEMENT
The term “non-operative management” is not consistently synonymous with “physical therapy” in orthopedic literature. Rather, non-operative management typically refers to oral pain medication, corticosteroid injections, use of an assistive device, use of an unloader knee brace, bed rest, or other palliative and passive interventions and these treatments have not shown favorable outcomes for PMMR tears.15 Well-designed physical therapy protocols, however, have demonstrated equivocal or superior outcomes to meniscectomy among older and younger patients with other meniscal tear types, but it is not known if the same can be true for meniscus root tears.16 Surgical repair is typically advised per concerns about rapid OA progression associated with PMMR tears in relatively young patients with previously healthy knees,7 but there is more to be learned from prospective longitudinal studies comparing surgery to physical therapy.
SURGICAL MANAGEMENT
Anatomic Two-tunnel Transtibial PMMR Repair
Up until the past decade, PMMR tears were often debrided rather than repaired. Emerging literature, however, has sounded the alarm for the critical need for repair rather than resection, because patients undergoing meniscectomy exhibit more rapid progression of radiographic arthritic joint changes and significantly earlier pursuit of a total knee arthroplasty (TKA) when compared to a root repair.15,17–20 The anatomic two-tunnel transtibial repair technique has emerged as the gold standard for PMMR tears due to biomechanical evidence showing restoration of joint compartment stress to near normal levels.21,22
Most patients who present with meniscal root tear pathology have medial knee pain which is exacerbated by deep squatting. Many can recall a specific episode, such as kneeling in the garden or climbing stairs and hearing a pop in their knee, while others may have no specific history and report a gradual onset of symptoms. In general, the longer patients have symptoms, the more often they experience joint effusions with activities, which usually indicates that the medial compartment has developed varying degrees of chondromalacia due to the meniscal root tear.
On physical examination, some will have medial joint line pain, where others may only have deep knee pain with full knee flexion or when squatting. In thin patients, when performing a valgus stress test at 30 degrees of knee flexion, meniscal extrusion may be felt along the margins of the medial collateral ligament. In addition, the meniscus may be extruded somewhat anteriorly, and this can be painful with deep palpation in patients.
Plain radiographs are essential to determine the status of the articular cartilage of the effected medial compartment when there is suspicion for a PMMR tear. Specifically, anterior posterior (AP), lateral, and Rosenberg views should be obtained in all patients to assess their degree of cartilage wear. In addition, a long leg alignment radiograph should be obtained to determine if the knee is in varus alignment. Patients in varus alignment have been noted to have poorer surgical outcomes, and this may be because they have extra stress on the healing root tear.23,24 MRI scans are essential to diagnose a PMMR tear. Most commonly, there is loss of signal within 1 cm of the posterior root attachment. This discontinuity can be seen on the axial and coronal views. On the sagittal views, there may be a loss of signal at the normal root attachment posteriorly, which has been called a “ghost sign.” This occurs because the meniscus root has been detached and it extrudes medially so there is a loss of signal where there would normally be a dark triangle shape of the meniscus at its posterior root attachment.
Surgical Technique
First, it is important to ensure that the patient is an appropriate candidate for a meniscus root repair. This can include ensuring that they have no more than grade 1 or 2 Kellgren-Lawrence changes on plain radiographs and do not have any limitations or pathologies which could limit their ability to be compliant in their postoperative rehabilitation program. Root repair may be contraindicated for patients who are unable to use crutches or a walker to follow the initial weight bearing (WB) restrictions.
The most common surgical technique is a transtibial tunnel root repair. In this type of technique, the bone where the meniscus root would normally attach is decorticated to provide a bony surface to maximize healing potential of the root reattachment. In addition, it is important to release the meniscus peripherally from the capsule when it is extruded, or the meniscus function will not be restored.25 This may require a release of the meniscofemoral and meniscotibial capsule all the way up to the level of the deep medial collateral ligament. Once the extruded meniscus has been sufficiently released, then tibial tunnel drilling is performed. The authors’ preferred technique is a two-tunnel technique which provides a broad-based healing surface of the meniscus. Self-capture meniscal suturing devices are used to place sutures or suture tapes into the meniscus substance and then shuttle them down these tunnels. When they are pulled out the anteromedial tibia, one can judge the ability of the meniscus to be pulled back to its attachment site and to reduce the meniscal extrusion. Once satisfactory reduction is achieved, the surgical sutures or suture tapes used to repair the meniscus substance are fixed to the tibia. The most common technique is to utilize a cortical button and tie the sutures over the button to the tibia. Postoperatively, radiographs are obtained to assess the position of the cortical button because an early fall after surgery could tear the sutures through the meniscus repair and result in button loosening. In cases where concomitant ligament reconstructions are performed, such as cruciate ligament reconstructions, it is important to assess tunnel trajectories for both the ligament reconstruction and the meniscus root repair to ensure that there is no convergence of the tunnels during the procedure.26
POST-SURGICAL REHABILITATION
Post-operative physical therapy can commence immediately after PMMR repair and is divided into four distinct phases (Table 1): Phase I – Recovery, Phase II – Transition to WB, Phase III – Rebuild, and Phase IV – Restore. Each phase has unique rehabilitation priorities, precautions (Table 2), and goals that align with timelines related to tissue healing and adaptation to physiological demands of the limb and joint. This review will focus on precautions following PMMR repair and the rationale behind them.
Unique Post-operative Rehabilitation Considerations
Post-operative precautions aim to minimize joint loading or movements that contribute to excessive distraction or displacement of the repair. Gradual activity progressions, with incrementally increasing meniscal demand, should align with biological healing timeframes and maturation of the repair. Rehabilitation progressions are not only guided by time and task mastery, but also by observations of joint irritability, utilizing algorithms such as the Pain Monitoring Model27 or Soreness Rules.28 Rehabilitation following PMMR repair differs from the more commonly seen repairs of traumatic vertical longitudinal tears in younger active or athletic patients. A more conservative progression is followed due to the fact that a PMMR tear is typically a radial tear type that severely disrupts meniscal hoop stress in an older patient with potentially more fragile or degenerative meniscus tissue. With these concerns in mind, there are multiple rehabilitation considerations that may be unique or amplified in the context of a PMMR repair.
Weight Bearing
Patients remain non-weight bearing (NWB) during the Recovery phase to minimize hoop stress through the meniscus and tension on the repair. This precaution is based on the known function of the meniscal root as an anchor against axial loading and findings from a laboratory study showing transtibial repair site loosening and displacement following cyclical joint loading to simulate WB.29 Weight bearing can be initiated after six weeks, but a gradual progression (two to four weeks) toward full weight bearing (FWB) is recommended to minimize joint reactivity and maximize normal gait mechanics. Once FWB is achieved, graded increases in daily step counts can be monitored through use of wearable technologies (smart phone/watch, pedometer) to avoid sudden spikes in joint loading which may contribute to increased irritability.
Range of Motion
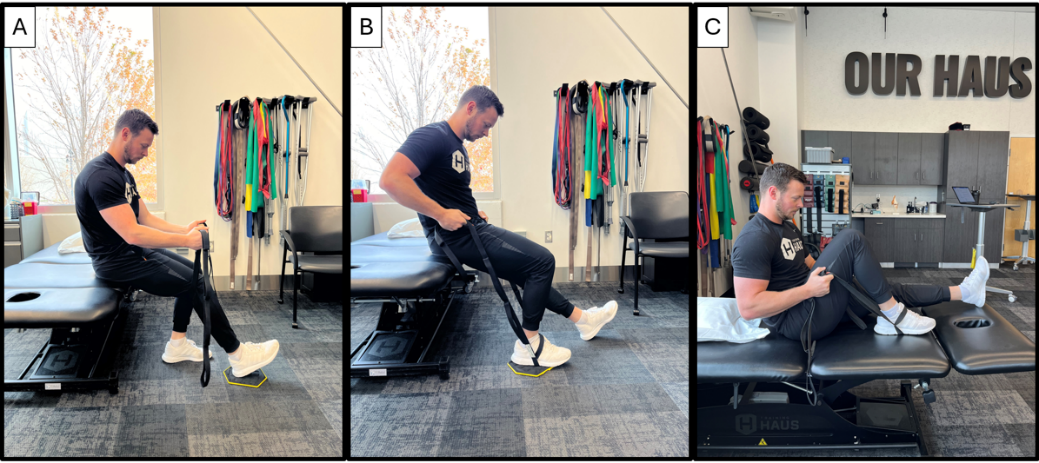
Joint ROM exercises can begin immediately after surgery; however, flexion angles are initially limited and the motion is performed passively to avoid potentially harmful tension through the repair. (Figure 1) The medial meniscus natively exhibits slight posterior translation with knee flexion.30 In the setting of a root tear, the posterior meniscus has been observed to exhibit increased posterior extrusion with progression into deeper knee flexion angles (90 degrees).31 Flexion ROM is limited to 90 degrees for the first two weeks after surgery and then patients can gradually progress, but should not push aggressively into end range flexion (Table 1). Passive flexion ROM can be advanced with different patient positioning and belt placement during the first four to six weeks after surgery. (Figure 1) Low rates of repair failure have been observed, upon second look arthroscopy, among patients following this ROM protocol.32 Full joint extension should be achieved immediately after surgery and preserved throughout recovery.
_progressions__a._seated_prom___90_degrees_with.png)
Muscle Strengthening
Early muscle strengthening activities should focus on restoring a strong volitional quadriceps contraction. Quadriceps strength has been identified as a critical factor for maximizing long term meniscal and articular cartilage health at the knee joint.33,34 Addressing joint pain and swelling is critical to minimize arthrogenic muscular inhibition (AMI).35 Traditional symptom management strategies such as limb/joint cryo-compressive therapy, elevation and compression garments can be supplemented with specific techniques to minimize AMI (Examples: focal joint cooling, and transcutaneous electrical nerve stimulation [TENS]).35,36 These strategies can be coupled with modalities to enhance quadriceps muscle contraction specificity, intensity and/or awareness such as neuromuscular electrical stimulation (NMES), surface electromyography (EMG) and vibration.35,36 The goal is to minimize muscular atrophy and maximize recovery of strength with exercises that are low-load and safe during the early recovery period. Blood flow restriction (BFR) therapy (with patients who do not exhibit any contraindications) can be added to minimize muscle strength loss and atrophy during this most restrictive phase. It may be advisable to perform open chain strengthening activities in a manner that minimizes tibial shear immediately following root repair. This would include isometric contractions at fixed angles or isotonic strengthening through a small arc of motion. As healing progresses into the remodeling and maturation phases after the initial three to four weeks, unloaded shear at the joint, with a broader arc of motion, may be tolerated.37,38
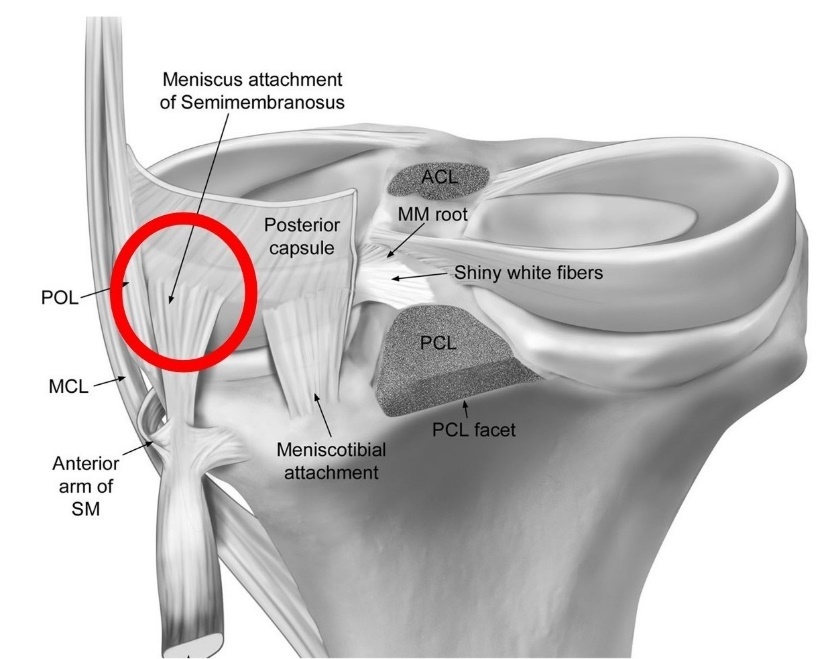
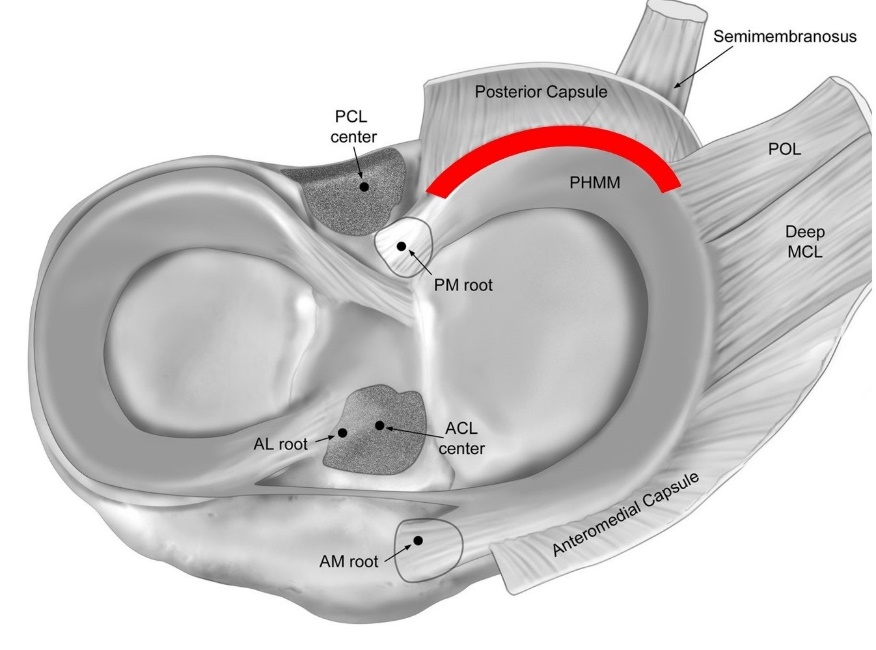
Hamstring strengthening, or even repetitive hamstring pulling with flexion ROM exercises, may warrant caution initially after PMMR repair. There are no biomechanical studies expressly examining the impact of open chain hamstring strengthening on meniscal repair, but caution stems from the known anatomy of the semimembranosus with its relatively broad attachment at the posteromedial joint capsule (Figure 2) and its function to mobilize the meniscus posteriorly with knee flexion.39 Theoretically, this could be disruptive, or at the very least irritating, to a healing posteromedial meniscus repair, because of this shared capsular attachment zone (Figure 3). When the meniscus is surgically released from the posteromedial capsule to address chronic extrusion, healing must occur at the meniscocapsular interval (Figure 3) and could be compromised by repetitive traction forces at the posteromedial capsule caused by hamstring pulling with knee flexion or strengthening activities. Further research is warranted to understand the effect of hamstring forces on PMMR repair.


Squatting
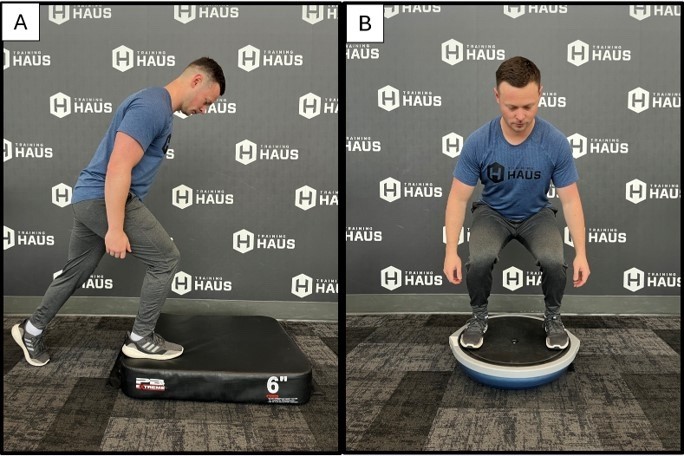
The role of the meniscus in managing joint compressive forces increases with greater knee flexion angles in WB as the articular cartilage contact surface area reduces between the femur and tibia.40–42 Increases in posterior horn meniscal pressure, joint compressive forces and joint shear have been observed with increasing squat depth.43,44 These biomechanical factors justify early squat depth restrictions following meniscus repair, particularly for radial and/or root tears at the posterior meniscus. Shallow squatting (<70 degrees) can commence once WB through an extended knee with gait is well tolerated, typically no sooner than 9 to 10 weeks post-surgery. Leg press or 2-legged squatting is initially well tolerated but does not control for off-loading of the surgical limb. To prevent off-loading, patients can initially employ strategies such as isometric holds in a triple flexion lunge position at the surgical limb (Figure 4A) or staggered stance squatting with the non-surgical limb up on a box or step. As recovery progresses and coordination permits, bilateral squatting on a BOSU provides excellent immediate input to help correct surgical limb off-loading. (Figure 4B) Progressions with squat depth or load should occur independently to allow for clear observations of joint reactivity before progressing both variables (depth plus load). Deep squatting is generally not advised following PMMR repair, especially in patients with no prior exposure to deep squatting or those with more degenerative tissue quality observed at the time of surgery. This precaution is based on prior research reporting increased risk of degenerative meniscus pathology in individuals with higher (occupational) demand for deep knee flexion (squatting, kneeling, stairs).45,46 Younger, more active patients, with healthier tissue quality and a non-degenerative tear mechanism, can progress squat depth and external loads gradually with ongoing observation for symptom response; however, this is not the primary demographic seeking care for PMMR tears.

Return to Run and/or Sport
Guidelines for returning to running or higher impact/sport activity are not well defined for PMMR repairs in part because the patient demographic is older, and the condition is often considered degenerative. In contrast, patients who undergo posterior lateral meniscus root repair are often expected to return to sporting activities, because lateral root tears are typically an acute injury that often occurs in the context of anterior cruciate ligament rupture in a younger, sporting population.9 Counseling on post-operative activities should account for the patient’s pre-operative activity exposure (activity type, intensity, frequency), underlying joint health, time-based healing guidelines, objective recovery criteria, and knee joint reactivity in response to activity progressions. Objective criteria that should be achieved prior to considering return to run are described in Table 1. Such criteria stem from the ACL reconstruction literature, including patients with concomitant meniscus repair. The goal is to maximize the likelihood of normal, symmetrical running kinematics and kinetics to reduce the potential for elevated or abnormal knee joint loading with running.47–49 Given the paucity of literature on this topic specific to this population, return to run and sport counseling should be approached on a case-by-case basis with shared decision-making between the patient, physical therapist, and surgeon.
OUTCOMES
Research on long term outcomes following root repair is increasing, but existing studies are often underpowered, retrospective in nature, and generally lower quality and should be interpreted with caution. Most studies compare root repair to arthroscopic debridement of the meniscus/root. Post-operative patient reported outcome measures show improvement from the pre-operative state following PMMR repair,50 with results superior to those reported for meniscectomy.51 A higher rate of conversion to TKA is reported following meniscectomy compared to root repair.52 Progression of OA is observed and meniscal extrusion persists following root repair, but the degree of OA progression is reduced compared to that observed following meniscectomy.50,52,53 Varus limb alignment and a higher degree of baseline articular cartilage disease are associated with worse post-operative outcomes, whereas age and body mass index are not consistently identified as poor prognostic indicators.51,54
CONCLUSION
Meniscus root tears are an increasingly recognized diagnosis that has been reported to be associated with a deterioration of knee joint health.7,52,53,55 Surgical techniques to repair PMMR tears yield superior outcomes compared to debridement51–53,56 and may slow OA progression and delay the need for future TKA.7,52,53,55 Post-operative rehabilitation protocols are not well defined in the literature and the degree of physical recovery to be expected or advised following PMMR repair is not yet well understood. Post-operative rehabilitation should focus on resolving fundamental deficits in joint motion, restoring muscle strength to symmetry and a relative level appropriate to the patient’s lifestyle, and coaching patients through a gradual return to activity, perhaps lower impact, per joint tolerance. Future research will help define best practices for post-operative rehabilitation and expectations for long term patient outcomes.
Statement of financial disclosure and conflict of interest
Jill Monson, PT, OCS has no conflicts of interest. Dr. Robert F. LaPrade, MD, PhD discloses the following relationships: Consultant: Ossur, Smith & Nephew, Responsive Arthroscopy, Royalties: Ossur, Smith & Nephew, Elsevier, Arthrex, Research Grants: Ossur, Smith & Nephew, AANA, AOSSM, Committees: ISAKOS, AOSSM, AANA, Editorial Board: AJSM, JEO, KSSTA, JKS, JISPT, OTSM, Education: Foundation Medical