INTRODUCTION
The steady decline in national physical activity levels and increases in overweight and obese adolescents1,2 has decreased the number of individuals eligible for military service3 and widens the physical readiness gap between the general population and military physical demands.4 This disparity complicates training physically capable recruits without injuring those who are less fit and highlights the need of minimizing preventable attrition such as those from musculoskeletal injury (MSK-I). Despite efforts to improve soldier readiness, more than half of all soldiers experience an injury annually.5 As many as 58,400 soldiers were not able to deploy in April 2020, which is the equivalent of 13 brigade combat teams.6 MSK-Is are the leading cause of non-deployability, lost duty days (LDD), medical encounters, military discharge, and disability.7,8 In 2018 the U.S. Army spent $434 million in direct medical costs to treat MSK-Is.7
The leading causes of MSK-Is are the same activities that leaders deliberately conduct to develop physical resilience9 including running, load carriage, other physical fitness training activities (besides running) and work-related tasks.8 Physical training results in the highest number of total injuries, while load carriage causes greater injuries per exposure.10 Other common causes of MSK-Is include overexertion, falls/slips, and occupational accidents.11
Researchers have identified multiple physical and behavioral MSK-I risk factors including prior injury, low aerobic endurance,12–16 high or low body mass index (BMI),17 and low muscular strength and endurance.18,19 Multiple previous studies have demonstrated that prior injury strongly predicts future injury14,16; however, it is unclear whether these previous injures had fully resolved or not. Female biological sex is a long-accepted risk factor for MSK-I,20–22 but recent research suggests this may be due to differences in average physical fitness rather than biological sex-exclusive differences.12,23–26 Military leaders have used these and similar study outcomes to develop injury prevention programs including physical fitness training regimens, MSK-I risk screening, and leader education with mixed results.10,27–29
These epidemiological studies summarize the dilemma: service members with prior injury and lower fitness levels tend to get injured while training to improve their physical fitness. It is possible that other modifiable risk factors exist that, if trained, may reduce injuries without such high injury risk.
Albert Bandura (1977) introduced self-efficacy as one’s confidence to perform a specific task. In behavioral psychology, this concept helps patients and clinicians establish a therapeutic path by accomplishing individualized, increasingly difficult tasks.30 Multiple subsequent publications have proposed positive relationships between self-efficacy and self-regulation,31 performance,31–33 goal-setting,34 and motor learning.35
Researchers have also found that psychological factors predict military performance outcomes.32,36,37 Gruber et al. found that for every one point increase on the new general self-efficacy scale, participants were 77.7% less likely to voluntarily withdraw assuming the other factors remained constant. Self-efficacy did not predict medical withdrawal; however, this study did not report injury statistics.36 In an initial entry Army training environment, Moran et al. found that psychological burnout was predictive of MSK-I, but did not measure self-efficacy.38 To date, no studies have reported the prospective relationship between self-efficacy, other known risk factors, and MSK-I in an initial entry military training environment.
Cadet basic training at the United States Military Academy (USMA) is a seven-week initial entry training course with physical demands similar to basic combat training. Many traditional risk factors for MSK-I have been investigated previously in service academy cadets, but the relationship between self-efficacy and injury has not. This study’s purpose was to investigate whether self-efficacy is a risk factor for MSK-I in an initial military training environment and compare it to other known risk factors. The researchers hypothesized that self-efficacy (overall and task-specific) would be lower among new cadets who sustain an MSK-I and negatively associated with MSK-I over time throughout cadet basic training.
METHODS
Study Design
This was a prospective cohort study investigating the relationships between self-efficacy, other known intrinsic and extrinsic risk factors and MSK-I in an initial entry military setting.
Study Size and Approval
All 1,200 incoming USMA new cadets were eligible to participate in this study. The Portsmouth Naval Medical Center Institutional Review Board (IRB) and USMA administrators reviewed and approved the study procedures prior to initiation. Participation was voluntary.
Participants and Setting
All participants were USMA new cadets completing cadet basic training from June to August 2022. Cadet basic training introduces new cadets to military skills while physically and psychologically preparing them to be service academy cadets and future officers. Some of the most strenuous and injury-causing events include running and strength training during morning physical fitness training (every week), the Army Combat Fitness Test (ACFT) (Weeks 5-6), land navigation (Weeks 3-4), and the final 12-mile ruck march (Week 7). Cadets also practice tactical skills including individual movement techniques, basic marksmanship, water survival, communication skills, and emergency medical treatment. The researchers recruited participants and collected all demographic, injury history, and self-efficacy data on Day 8 of 44 following a verbal study explanation and written description.
Inclusion/Exclusion Criteria
All English-speaking new cadets qualified to begin cadet basic training were eligible for inclusion. Cadets were excluded only if they declined to participate, had not fully recovered from a previous injury, were already injured at the time of the consent/survey, or attritted from cadet basic training for reasons other than MSK-I. All participants under 18 years old were considered emancipated minors and did not require parental consent. All participants who consented for this study also consented participation to a randomized controlled trial by Scott et al. related to back pain beliefs and maximum deadlift. All randomization and interventions for this study were conducted separately and included same-day back pain resilience education for all participants to prevent subsequent pain avoidance behaviors during Week 5 or 6 of cadet basic training.39
Reporting prior injuries is a sensitive topic due to fear of administrative disqualification, so the researchers assured the new cadets’ confidentiality whenever asked to self-report prior or current injury. All participants who reported a history of injury within the past year classified themselves as either completely recovered (1), mostly recovered (2), or not recovered (3) and completed the Single Assessment Numeric Evaluation (SANE). The SANE required the participants to rate the previously injured body part on a scale of 0% to 100% and has demonstrated reliability and concurrent validity with other injury-specific outcome measures.40–43 Patient Acceptable Symptom State (PASS) thresholds for SANE scores range from 65.5% to 82.5%, but there is no evidence-based threshold when an injured individual has fully recovered.44–46 In the present study, participants were excluded if they described themselves as “not recovered” regardless of SANE score or if they described themselves as “mostly recovered” or “completely recovered” with a SANE score of less than 80%. This was to ensure the unresolved prior injuries (or a currently injured state) did not affect participants’ self-efficacy to complete CBT and specific events without injury.
Outcome Measures
The primary outcome of interest was either new injury or recurrence of a previously resolved musculoskeletal or neurological injury. Systemic conditions, skin reactions, and infections were excluded as well as blisters and ingrown toenails which are commonly treated by on-site U.S. Army medics without duty limitations. The researchers operationally defined injuries as a neuromusculoskeletal condition which required care at a medical treatment facility, with or without duty limitations.20,21,47 This definition eliminated recall bias and the difficulty of obtaining self-reported injury status, which might not have been serious enough to seek medical treatment. Time was recorded as the number of days from study consent to the initial medical encounter.
Procedures and Variables
The primary independent variable of interest was the participants’ self-efficacy to complete cadet basic training without injury and self-efficacy to complete the three most injury-causing and physically demanding events without injury (land navigation physical demands, the 12-mile ruck march, and the ACFT). Although scales for general and pain self-efficacy exist, these scales lack task-specific concordance with the cadet basic training events.48 The researchers developed task-specific self-efficacy questions (Appendix A) following guidance from Bandura and other previous studies.32,49 The consent form and survey were piloted among a group of first-year cadets to ensure clarity, accuracy and cultural appropriateness. The participants rated their self-efficacy prospectively on Day 8 via the questionnaire with an 11-point numerical rating scale from 0 (no confidence) to 10 (fully confident). The combined event-specific self-efficacy item combined the three scores from land navigation athletic demands, the 12-mile ruck march, and the ACFT for a maximum score of 30 (items 2-4, Appendix A). Prior to collecting data, the researchers selected approximately 70% as the cut-off for low self-efficacy based on previous research.50,51 We also planned on visually inspecting the data in quartiles and tertiles in comparison with our cut-off score.32,52 Participants completed this questionnaire immediately after consenting to participate. The baseline questions survey demonstrated good internal consistency according to Cronbach’s alpha (0.817).
Other independent variables included age, biological sex, height, weight, previous military experience, performance motivation, athletic intentions, history of injury within the past year, current level of relative function (only for those with a history of previous injury), baseline aerobic fitness (2-mile run time), baseline upper body muscular endurance (hand release push-ups in 2 minutes), and anterior core muscular endurance (maximum plank duration). Age and sex were both self-reported and verified with the participants’ medical record. Injury history, previous military experience, academy overall performance motivation, athletic intentions (intending to participate in division 1, club or intramural athletics), height, and weight were also collected by self-report. Self-reported height and weight has previously demonstrated validity in the military population.53 The service academy cadet basic training cadre and instructors conducted the 2-mile run, hand release push-up and plank performance assessments according to military testing standards54 on days 3 to 5.
Data Sources/Measurements
The researchers received demographic and performance information from USMA administrators. Participants self-reported additional demographic information, previous experiences, previous injury, and self-efficacy using a paper-based survey. The researchers collected new injury data individually using the Armed Forces Health Longitudinal Technology Application (AHLTA) and the Cadet Injury and Illness Tracking System (CIITS). CIITS is a program unique to this service academy for all participation-limiting injuries. To protect from bias, all other variable data (including self-efficacy data) were hidden during injury surveillance. Additionally, 10% of all questionnaire responses and injury designation data were checked by another researcher for accuracy.
The injury study period lasted 36 days during cadet basic training and the injury surveillance additionally lasted for the entire following semester (174 total days from start to finish). This additional surveillance time was to capture injuries that began during cadet basic training but either received delayed medical care, did not resolve with time alone or worsened during the fall semester. The additional surveillance time did not include any injuries that occurred after cadet basic training ended. The researchers also captured days until the approximate onset of symptoms and days between the onset of symptoms until the medical encounter.
Data Analysis
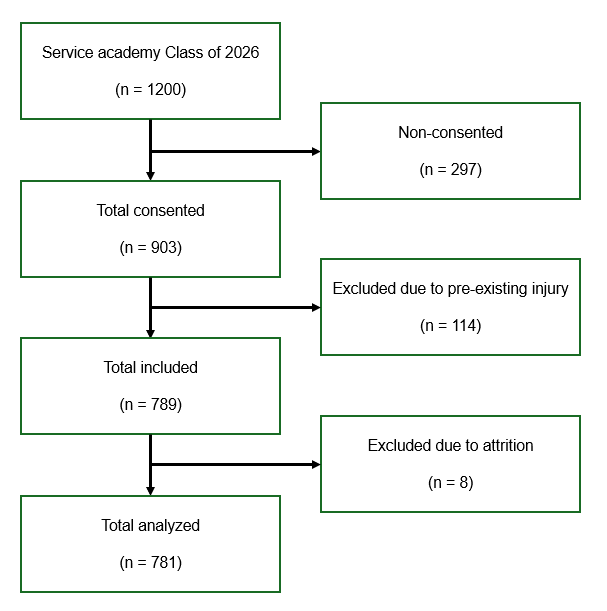
After excluding ineligible participants (Figure 1), the researchers conducted descriptive analyses to compare the independent variables between injured and non-injured participants. Missing values were excluded with pairwise deletion. The researchers recorded and analyzed all data using Statistical Package for the Social Sciences (SPSS), version 28 (IBM Corps, Armonk, NY, 2021).
The independent samples t-test was used to compare continuous data, chi-square test was used to compare categorical data, and effect sizes were calculated with Cohen’s d and phi.
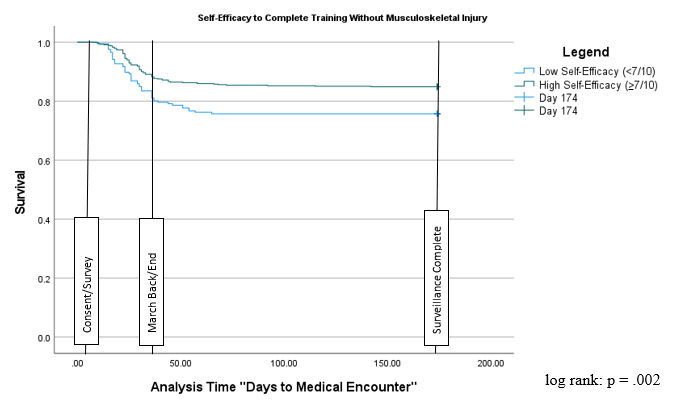
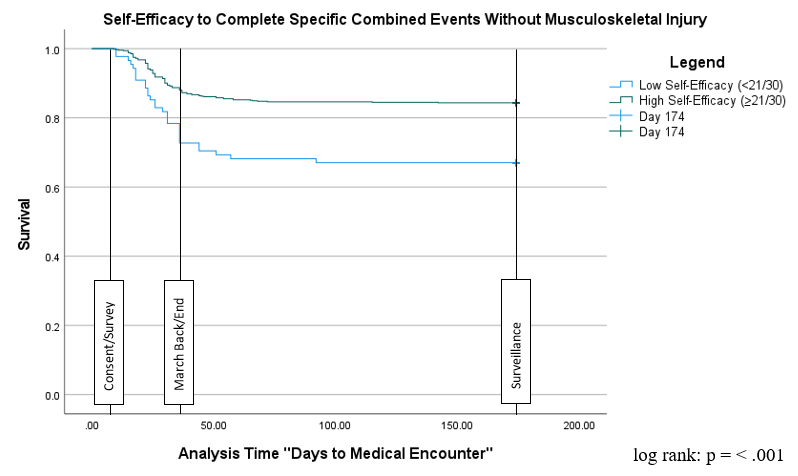
The researchers used a Kaplan-Meier survival analysis to determine whether the risk of injury throughout cadet basic training was different between those with low or high self-efficacy. New cadets who reported self-efficacy of 7/10 or less to complete all of cadet basic training or 24/30 or less to complete the three combined specific events without injury were identified as having low self-efficacy and compared to new cadets with 8/10 or 25/30 or higher self-efficacy, respectively. The new cadet population was a fixed-sized, closed cohort that began and ended training on the same days. There were some differences in daily training schedules, but the cohort completed training events within the same week. Kaplan-Meier analysis assumptions were met by excluding all new cadets with current or unresolved injuries, beginning the surveillance period simultaneously, defining the censoring event as the first medical encounter date, and by terminating survival at the day of the first medical encounter or right-censoring at 174 days. Subsequent injuries sustained by the same participant were not included in the analysis. The researchers used the log-rank test (α < 0.05) to determine whether the time to event was statistically significant between new cadets with high versus low self-efficacy.
Individual variables predictive of future injury were identified using univariable Cox proportional hazard ratios. The researchers purposefully selected variables similar to methods in previous literature based on previously established risk factors.32,55 Variables that were statistically significant (α < 0.05) were compared using correlation coefficients (Pearson’s and Spearman rho for continuous and categorical data, respectively) to identify potential collinearity. Variables that did not statistically predict MSK-I or demonstrated moderate to high (> 0.5) correlation were considered for omission from the multivariable analysis. Finally, a multivariable Cox proportional hazard ratio was used to construct a model that predicted MSK-I between all variables of interest and the dependent variable of time to injury.
RESULTS
Of 1200 new cadets, 903 (75.3%) consented to participate in the study. The baseline demographic information revealed that 22 participants had “not recovered” from pre-existing injuries and 43 reported an injury within the last year with SANE of less than 80%. Injury surveillance revealed that 49 new cadets received medical treatment for injuries prior to consent and self-efficacy data collection. Eight included participants left cadet basic training for either non-musculoskeletal medical reasons or by voluntary withdrawal. In total, 122 participants were excluded, leaving 781 new cadets for analysis (Figure 1).

During the 36 days following the survey, 136 (17.4%) new cadets sustained at least one MSK-I that required medical attention with or without work limitations. The most injured regions were the knee (38, 27.9%), ankle (27, 19.9%), lower leg (22, 16.1%), foot (13, 9.6%), and hip/pelvis (9, 6.6%). The most common injury natures were ligament sprains (33, 24.3%), bone stress injuries (23, 16.9%), joint synovitis (20, 14.7%), and tendinopathy (20, 14.7%). The most common injury causes were aerobic physical training/running (41, 30.1%), ruck marching (24, 17.6%), land navigation (19, 14.0%), gradual onset (14, 10.3%), and organized athletics (8, 5.9%). Appendix B contains the complete injury and associated activity analysis.
The average class self-efficacy score was 8.2/10 to complete cadet basic training without injury and 26.0/30 to complete the combined task-specific events without injury. The lowest tertile responded at or below 7/10 to complete all of cadet basic training without injury and at or below 24/30 to complete the three combined specific events without injury. The researchers used these cutoff scores to differentiate between low and high self-efficacy.
Statistical results comparing injured and uninjured participants are summarized in Table 1. Two-mile run performance was the only statistically significant variable with a large (Cohen’s d>0.8) effect size (t(764)=-9.40, p=<0.001). Independent variables with a positive and statistically significant but small effect size (Cohen’s d<0.5) included self-efficacy to complete cadet basic training without injury (t(773)=2.94, p=0.002), combined event-specific self-efficacy (t(770)=4.08, p=<0.001), sex (X2(1, N=781)=41.28, p=<0.001), hand release push-up performance (t(773)=4.00, p<0.001), plank performance (t(772)=3.88, p=<0.001), height (t(765)=5.00, p=<0.001), and weight (t(762)=2.01, p=0.036). Age, BMI, injury history (only including those above an 80% SANE), athletic intentions, personal performance goals, and prior military experience were not statistically different between those who experienced an injury and those who did not. Although attending the service academy preparatory school was found to be significantly different between injured and uninjured new cadets, it was not carried forward in the analysis due to internal differences (higher athletics participation) between cadets with and without this extra year of training.21
The Kaplan-Meier survival curves in Figures 2 and 3 display MSK-I occurrences over time by participants with low (blue line) and high self-efficacy (green line) to complete cadet basic training uninjured (Figure 2) and the combined specific events uninjured (Figure 3). Under both conditions, new cadets with self-efficacy scores of 7/10 or less (Figure 2) or task-specific combined self-efficacy of 24/30 or less (Figure 3) demonstrated a significantly reduced probability (p=0.004 and p=<.001, respectively) to continue training without injury over time according to the log-rank test.


All variables that demonstrated statistically significant difference between new cadets with and without MSK-I resulted in statistically significant univariable hazard ratios (HR). History of a resolved prior injury again was not a hazard for injury during cadet basic training. Correlation analysis (Table 2) demonstrated a moderate (>0.5) correlation between height and weight (r=0.68), sex and height (r=0.60), and sex and hand release push-up (r=0.58). Using a selective stepwise method, height and weight were excluded from the subsequent multivariable analysis due to correlation with each other, sex, and hand release push-up. There was also a moderate to strong correlation between self-efficacy to complete cadet basic training and combined specific events (r=0.63). The multivariable Cox proportional hazard ratio analysis was conducted using two different models to account for collinearity between the self-efficacy variable, each with a self-efficacy variable included.
Tables 3 and 4 depict results from the univariable and multivariable Cox proportional hazard analyses. The univariable analysis demonstrated that height, weight, hand release push-up performance, plank performance, and both self-efficacy measures were all individually protective against MSK-I risk over time. Compared to males, females had a greater injury risk over time. Lastly, new cadets with slower 2-mile run times were also at a greater MSK-I risk over time (Table 3). Of the other variables statistically significant in the univariable models, only slower 2-mile run time predicted injury risk over time (HR=1.004 [1.003-1.006], p=<0.001) in the multivariable model (Table 4).
Although injury history did not demonstrate a statistical significance, the researchers decided to include it in the multivariable analysis due to strong historical prediction for future injury. When included in the multivariable analysis, it was again not predictive of future MSK-I (HR=1.19 [0.83-1.70], p=0.335).
DISCUSSION
The primary purpose of this study was to test the strength of association and predictive value between self-efficacy and future MSK-I. The results support the hypothesis that new cadets who sustained an MSK-I had significantly less self-efficacy than those who remained uninjured and had a shorter survival time during cadet basic training. However, when controlling for other known risk factors, only aerobic fitness (2-mile run time) predicted MSK-I.
These results are the first to prospectively demonstrate that self-efficacy to complete strenuous military training without injury was lower among new cadets who sustained an MSK-I. Those with lower self-efficacy also had reduced time to injury compared to new cadets with high self-efficacy. However, self-efficacy is not predictive of future MSK-Is when controlling for other important covariates. This is not surprising considering that the six sources of self-efficacy56 might interact with the other risk factors. For instance, individuals with lower aerobic fitness might report lower self-efficacy due to the perceived level of necessary exertion to perform specific tasks. Future research is needed to determine how previous injury affects self-efficacy, the interactions between self-efficacy sources and performance, and how self-efficacy affects injury, performance, and other important risk factors.
These findings support prior research that low aerobic physical fitness, as identified in a one to two mile running assessment, is the strongest predictive risk factor for MSK-I during initial entry training.13,14,24,57,58 In this cohort, a one second increase in 2-mile run time increased the MSK-I hazard ratio by 0.5%. This can be interpreted as for every one minute increase in 2-mile run time, there was a 30% increased risk of sustaining an MSK-I. This study’s injury surveillance echoes the classic training conundrum: aerobic physical training (running) and ruck marching accounted for 47.1% of all training injuries. This implies that military leadership and instructors should continue to use low aerobic fitness performance to identify at-risk populations, conduct appropriately programed training such as ability group-based running,59,60 and consider improving the other independent factors that were associated, although not predictive of MSK-I.
Previous injury is one of the most widely accepted risk factors for future injury, but was not significantly different between the injured and non-injured population in this cohort. This may have been due to either the previous injury timeframe (one year) or distinguishing between resolved and unresolved previous injuries. The researchers surveyed previous injuries within the past year in order to capture relatively common athletic injuries such as anterior cruciate ligament tears, which can take a year to fully resolve. Previous studies surveyed previous injuries within the prior three to six months.18,47 The longer timeframe might have resulted in including more positive responses for mild to moderate previous injuries with more time to fully resolve.
This study uniquely distinguished between resolved and unresolved previous injuries by requiring participants to rate their current level of function according to the SANE. The researchers chose this method to control for unresolved previous injuries at the time of the survey but expected previous injury again to strongly predict future injury. This finding presents a potential need to differentiate between resolved and unresolved previous injuries at the beginning of an injury surveillance study and might emphasize the importance of “finishing” rehabilitation to prevent future injury. The plethora of previous research on prior injury as an MSK-I risk factor necessitates future research with the same and related populations before elucidating the relationship between prior injury, injury resolution, and future injury.
Other independent variables that were significantly different between the injured and non-injured groups (associated with MSK-I) but did not collectively predict MSK-I included height, weight, biological sex, plank, and hand release push-up performance. Biological sex and height are both intrinsic factors which have previously demonstrated association with MSK-I during military training. This study adds to a substantial body of evidence that when controlling for other injury risk factors, biological sex alone does not predict future injury.12,14,24,26,57 However, females may exhibit higher injury risk due to physiological traits that predispose all soldiers to injury, such as slower 2-mile run times, shorter height, lower weight, and lower hand-release push-up performance.18,22
Hand release push-up and plank performance were significantly different between the injured and non-injured groups and were predictive of MSK-I individually, but not when controlling for the other risk factors. De la Mott et al. previously found strong and moderate evidence of relationships between upper body and core muscular endurance respectively and both have demonstrated value as part of a prospective injury screen.18,60 However, when controlling for other risk factors, Moran et al. also did not find push-up endurance to be predictive of injury.38 Because of this association, but not predictive value, military instructors should continue to train upper body muscular endurance, but it is unclear whether the hand release push-up nor the plank should be included in injury prevention screening. This is the first known study to identify hand release push-up performance as a potential MSK-I risk factor based on univariable analysis.
It is important to emphasize how self-efficacy concepts should and should not be incorporated into training. First, this study did not find that low self-efficacy was able to predict future injury when controlling for other known risk factors and therefore, should not be used in isolation to identify at-risk populations. However, based on mean differences and univariable relationships, self-efficacy may be a modifiable extrinsic risk factor. Self-efficacy is a psychological concept, but training could include strategies beyond talking and thinking about confidence. Training strategies could include leveraging the six sources of self-efficacy: enhancing mastery experiences (prior success), vicarious experiences (seeing others succeed), physiological state (including nutrient timing and adequate sleep), affective state, verbal persuasion, and mental imagery.56 More specific intervention strategies are beyond the scope of this analysis and future studies should explore intervention effectiveness.
One strength of this study was the researchers’ thorough injury surveillance through multiple electronic medical record reviews, including all musculoskeletal patient encounters, radiology reports, and physical screenings. Working in the same facility as the other medical providers allowed the authors to clarify injury diagnoses when medical documentation was unclear. This resulted in very few classifications as “other” or “unknown” injury causes. Injury trends were otherwise similar to prior initial entry training environment research.20,21
The researchers chose to develop a task-specific self-efficacy assessment to ensure concordance48 with cadet basic training events and it demonstrated strong internal consistency. The low self-efficacy cutoff scores based on the lowest tertiles were consistent with findings on the Pain Self-Efficacy Questionnaire (40/60 [67%])48 and the Return to Work Self-Efficacy (RTW-SE) Questionnaire (4.6/6 [77%]).49 Although the items were developed following guidance by Bandura, a limitation of our study is that it was not validated with another accepted self-efficacy scale. Future studies should consider validating custom self-efficacy questionnaires with either the Pain50 or General36 Self-Efficacy Scales.
Another limitation to this study included consent and survey timing. Due to the demanding cadet basic training schedule, study consent and survey took place 1 week after cadet basic training commencement, which was the soonest available opportunity. Although this occurred prior to high-demand physical training events except for a portion of the ACFT (only push ups, plank and 2-mile run), 26% of all known injuries during cadet basic training occurred prior to the beginning of data collection and therefore were not a part of the analyzed data set. It is reasonable to assume that these cadets, who were the first to sustain injuries, may have been a valuable addition. Future studies should prioritize surveying participants as early as possible for overall self-efficacy.
Self-selection bias both when consenting to the study and in seeking medical care was another considerable limitation. The reasons for only 903 (75.3%) of the 1200 new cadets agreeing to participate in this study despite no additional time requirements could have been related to reporting prior injuries, consenting to medical records review, or having to consent to two separate studies simultaneously. Also, new cadets had the ability to choose whether or to seek medical care except in emergency situations.
Lastly, this study was limited to the relationship between self-efficacy and MSK-I, but as a psychological trait, may have a broader reach. Individuals with lower self-efficacy might exhibit decreased resilience to illness or psychological stress, leading to more medical or mental health encounters. Future studies might consider examining the relationship between self-efficacy and all medical encounters.
CONCLUSION
There was a significant, although small relationship between new cadets who reported low self-efficacy and future MSK-I during initial entry training. Self-efficacy could potentially be a modifiable risk factor, but further research is necessary to validate these findings and identify beneficial interventions. At this time, self-efficacy assessments should not be used alone to identify those with higher MSK-I risk. Additionally, this study strongly supports the body of literature that aerobic performance can be used to identify at-risk populations and proposes using the SANE to differentiate between resolved and unresolved injuries for injury surveillance research.