INTRODUCTION
Anterior cruciate ligament (ACL) injuries are common, with approximately 100,000 incidences occur annually.1–3 Rehabilitation is lengthy,4 prognosis for developing osteoarthritis is high after ACL reconstruction5 which poses a significant annual healthcare burden.6 Over half of all sports-related ACL tears occur with a non-contact mechanism, with female incidence being two to eight times greater than males.7,8 Insufficient motor control and poor landing mechanics, such as increased dynamic knee valgus and shallow knee flexion angles, are hypothesized to increase ACL injury risk.9 Additionally, stiff landings,10 often characterized by increased vertical ground reaction force (vGRF)11 and axial compressive forces,12 have been associated with a greater risk of ACL injury. Many of these factors in non-contact injuries are movement-related which are more likely modifiable with training. Identifying and integrating strategies to address these factors may reduce ACL injury risk.13 Although the cause of injury is multifactorial and complex, in a recent prospective study vGRF was found to have the strongest association with sustaining an ACL injury.11 Furthermore, vGRF is easily measurable via force plates and may be a salient measure that is readily modifiable by athletes as previous work has demonstrated improved vGRF and knee alignment following augmented feedback.14
Since jumping and landing pose ACL injury risks to athletes in sport, motor learning approaches and strategies can be used to modify technique where four processes need to occur in rapid succession. Each athlete must strategically decide on the environment-specific goals of the task, integrate their motor perception, sequence any observed spatial targets, and effectively interpret the sequence of special targets into the desired muscle activation.15,16 The use of both knowledge of performance and knowledge of results provided via augmented feedback may better serve to facilitate the scaffolding of a cognitive bridge to more efficiently modify a given motor pattern.17
Insufficient neuromuscular coordination and execution during drop landing tasks place athletes at an increased risk of ACL injury.9,11,12,18,19 Incorporating two-dimensional (2-D) video footage and the use of augmented feedback has been an effective modality in manipulating the aberrant movement patterns reflected by neuromuscular deficits, displayed during landing.18,20–22 Furthermore, it’s postulated that the inclusion of randomized, reactive movement patterns throughout training may further improve motor planning and skill acquisition integration into game-like scenarios.23 These understandings drive the foundational salience of a drop landing movement pattern as well as the importance of simultaneously completing a task that demands the athlete’s attention. The use of augmented feedback to train landing mechanics in adolescent female athletes suggests that individuals who experience initial vGRF > 3.77 body weight (BW) demonstrated the most change after training.24 Therefore, there seems to be a floor effect to the responsiveness of this type of training. Such a phenomenon may partially explain the difficulty of implementing large-scale and generalized preventative programs.
It has been estimated that approximately 122 female athletes would need to be trained in a preventative program for one ACL injury to be avoided.13 Although such preventative training programs appear to be effective in reducing injury, if individual athletes with specific risk factors can be readily identified, this may increase the efficacy of such efforts. Since vGRFs have been identified as a risk factor for ACL injury risk, and it has been shown that some athletes respond more favorably to augmented feedback to reduce vGRFs, establishing a means to identify those individuals that may respond best to augmented feedback may improve the efficient delivery of preventative training. Therefore, the purpose of this study was to identify which female athletes most readily respond to a single session of augmented feedback to attenuate vGRF, by considering baseline peak vGFR and change in vGRF during training.
METHODS
SUBJECTS
This study was approved by the University Institutional Review Board. Before participation, all participants or a parent/guardian provided their written informed consent following university guidelines. One hundred forty-seven females at regional high schools between the ages of 13-18 years participated in a single session. Age, height, body mass index, and Tegner level25 were recorded. All were actively participating female athletes in competitive organized sports. Exclusion criteria for the study included (1) any current lower extremity injury, (2) knee pain at rest or during running or jumping, (3) pregnancy, (4) any cardiovascular abnormalities or medical condition that limited training as indicated by a physical activity readiness questionnaire (PAR-Q).26 All participants utilized their own athletic footwear and wore comfortable athletic clothing.
PROCEDURES
Participants were asked to complete a drop landing from a 50-centimeter (cm) box onto two portable force plates after a self-selected warm-up and three trials for familiarization. Before testing, athletes were given verbal instructions for the landing task including: 1) jump forward with both feet and land with both feet on one of the force platforms, (2) jump bilaterally rather than stepping off the box, (3) land as to not to step from the force platforms, (4) return to standing after the landing. During data collection, trials were repeated if those requirements were not met. Data were collected generally in a gymnasium or common space on site with a ceiling height that could accommodate the experimental setup.
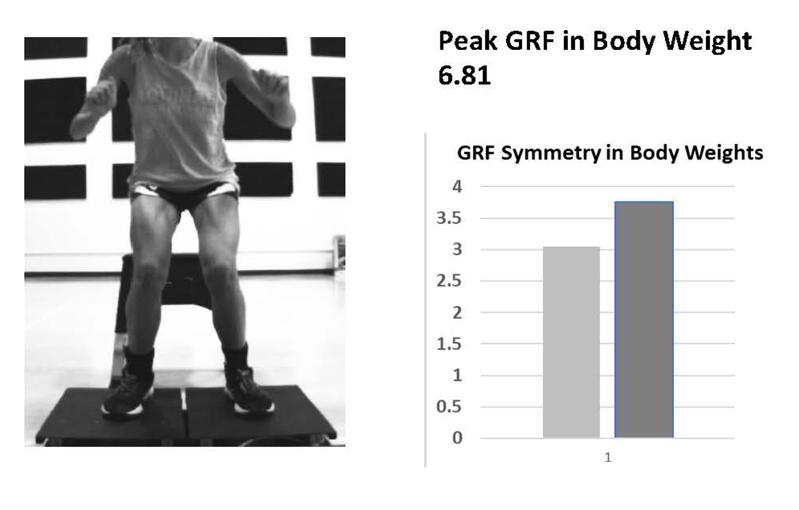
Athletes completed 30 landing trials divided into five blocks of six trials with a one-minute rest period between each trial block. During the initial block (Pre-test), participants were blinded to feedback to determine their baseline landing performance. Before beginning the training blocks, the athletes were provided with a brief orientation of the type of visual feedback they would receive on the visual feedback display following each trial. This information included peak vGRF displayed in body weight (BW), symmetry of lower extremity vGRF demonstrated through a bar graph, and frontal plane video that was replayed by the investigator in a slower motion to depict a qualitative impression of the performer’s body position during landing. No quantitative data was gathered from the video and presented during training.
Specific feedback was provided using the visual display by instructing participants to lower the overall height of the graph, try to make the graphs representing each leg even, and how knee position may have changed between trials (Figure 1). The baseline test was followed by the first training block where participants received post-trial feedback based on these data coupled with cues for improving their landing performance. Athletes were provided with both externally focused feedback first (e.g., “try to reduce the vGRF value”, “try to land quieter or more softly”) and internally focused feedback (e.g., “try to keep your knees over your toes,” “try to land with your knees out”). This feedback was individualized based on what was observed from the peak vGRF, vGRF symmetry, and impression from the frontal plane video of the landing. The feedback was based on the order of processing and displaying these data (peak vGRF, vGRF symmetry first, and then video performance). Data appeared within 20 seconds of the landing. The video was viewed at the same time in a separate window.
Athletes were given time to review the data with an investigator and relevant cues addressing their performance were provided. The next trial was then immediately performed such that the entire testing and feedback provided took approximately 20 minutes for all trial blocks. The general training and feedback provided were systematic where once vGRF showed substantial improvement, the next variable (symmetry or body positioning) was addressed. During the second training block, the feedback from the investigator was gradually withdrawn so that the athletes were asked to self-evaluate their peak vGRF, loading symmetry, and body position projected to the display.

Following the completion of both training blocks, a post-test (six trial block) was completed without any verbal or visual feedback. Finally, a transfer task was examined where a dual task landing was performed without feedback. During the transfer task, participants were required to complete the landing task with a distracting element. This distraction was accomplished by having to respond to a ball being passed in their direction to catch it, or the pass would be faked. A completed or faked pass was completed in a randomized order. Six trials were performed. Outcome data from the transfer condition performance trials were averaged.
INSTRUMENTATION
Kinetic data were collected in situ from two custom, high-impact force plates. Each force platform was positioned adjacent to one another and 25 cm in front of the 50 cm box. Each force platform had 4 calibrated load cells (ntep-1klb shear beam load cell) capable of measuring vertical force. Vertical ground reaction force data were sampled at 2000 Hz from each plate and data were normalized to each participant’s body weight. The system was validated in a pilot investigation of 20 participants where the custom force platforms were placed directly on top of two commercially available force platforms (Model 4080, Bertec Corporation, Columbus, OH) and sampled at 2000 Hz on both systems. The peak vGRF was well within 5% peak vGRF obtained with commercially available force platforms.14 This level of accuracy is similar to other portable force plate systems that have been validated against traditional force platforms.27 During each performance trial, a frontal plane video displaying each participant’s lower extremity was recorded from a high-speed camera at 100 Hz (DFK 23UV024, The Imaging Source, LLC, Charlotte, NC, USA). The camera was positioned 65 cm atop a tripod and located 130 cm from the force plates. Custom scripts were implemented within Visual Basic (Microsoft, Redmon, WA, USA) to calculate vGRF parameters and portray the video.
STATISTICAL METHODS
Participants were classified by initial baseline vGRF and response to augmented feedback training following training block 2. Previous work has suggested that impact force of greater than 3.77 BWs may indicate individuals most likely to benefit from augmented feedback training.24 Additionally, when investigating response to training over four weeks, a change of 0.25 BWs was the smallest change observed during this training.28 Thus, participants were grouped into four types of data: (1) those showing >3.77 BWs initially and demonstrating an improvement >0.25 BW in training (High Baseline-Responders (HB-R)), (2) those showing >3.77 BWs initially and demonstrating an improvement <0.25 BWs in training (High Baseline-Non-responders (HB-NR)), (3) those showing <3.77 BWs initially and demonstrating an improvement >0.25 BWs in training (Low Baseline-Responders (LB-R)), and (4) those showing <3.77 BWs initially and demonstrating an improvement of <0.25 BWs in training (Low Baseline-Non-responders (LB-NR)).
Linear regression was then used to quantify how well initial baseline vGRF measures and change in vGRF measures could be used to predict response to augmented feedback training. Pre-test vGRF, change following training block 1, and change following training block 2 were included in a hierarchical regression model to predict mean post-test vGRF and transfer vGRF using SPSS (Version 28, IBM, Aramonk, NY).
RESULTS
A total of 147 athletes participated and were classified into these four groups (Table 1). The first group consisted of 107 participants with high baseline vGRFs and responded to augmented feedback training (HB-R). The second group consisted of 11 participants with high baseline vGRFs but did not respond to augmented feedback training (HB-NR). The third group was comprised of 17 participants with low baseline vGRFs and responded to augmented feedback training (LB-R). The final group contained 12 participants with low baseline vGRFs but did not respond to augmented feedback training (LB-NR).
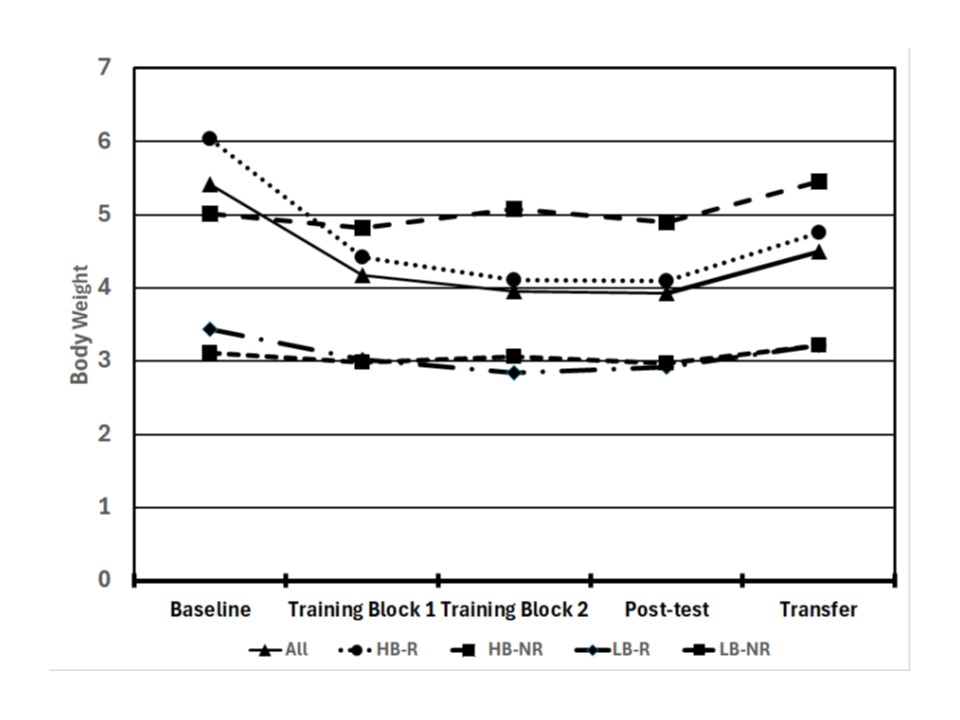
Baseline vGRFs, changes in vGRFs with augmented feedback training, post-test vGRFs, and transfer vGRFs are reported in Table 2 and displayed in Figure 2. Twenty-three athletes did not appear to respond to augmented feedback training and initial measures of vGRF were not sufficient to identify these athletes. There was a nearly equal number of low baseline non-responders (LB-NR) and high baseline non-responders (HB-NR) (12 vs. 11, respectively).

In the HB-R group, individuals showed a reduction of 26.7% in vGRF after training block 1 of augmented feedback. This was followed by a further improvement of 7.01% after training block 2. These participants were able to reduce their vGRF during the post-test and transfer tasks compared to baseline scores by 27.17% and 16.82%, respectively. Those with high baseline vGRFs but did not respond to augmented feedback training (HB-NR) showed less than 4% improvement in vGRF at any point during training and even increased 8.78% compared to baseline vGRFs during the transfer task.
In those with low baseline vGRFs, 17 participants athletes demonstrated further reductions in vGRF with augmented feedback training (LB-R). They exhibited a 11.95% reduction in vGRF after training block 1 of augmented feedback, with vGRF exhibiting another 5.96% reduction after training block 2. This subset of participants reduced their vGRFs by 17.96% and 7.19% during the posttest and transfer tasks, respectively. Those not responding to augmented feedback training but demonstrating an initial low baseline vGRF, demonstrated less than 5% change across all blocks (LB-R).
Linear regression revealed that baseline vGRF explained over 50% of the variance in post-test vGRF (R = 0.713; R2 = 0.508). Adding the change score from augmented feedback training block 1 improved the model (R = 0.883; R2 = 0.780) and including the change score from training block 2 improved the model further (R = 0.955; R2 = 0.911). When assessing the transfer task, linear regression revealed that baseline vGRF explained 40% of the variance in vGRF (R = 0.633, R2 = 0.400). Utilizing the change score from augmented feedback training block 1 improved the model (R = 0.797, R2 = 0.635) with the change score from training block 2 resulted in further improvements in the model (R = 0.872, R2 = 0.761).
DISCUSSION
The purpose of this study was to assess how baseline impact force and single session response to augmented feedback training can be used to identify those most likely to benefit from this training. Baseline ground reaction force appears to be a relatively strong predictor of those that will respond to augmented feedback training explaining 50% of the variance in reductions in vGRF as a stand-alone measure. However, there appears to be a subset of athletes who, despite showing high baseline vGRFs, do not respond to augmented feedback training. Assessing their response to at least one round of augmented feedback training appears necessary to identify these individuals. Thus, attempts to identify those most likely to benefit from augmented feedback training will likely need to incorporate both screenings of baseline vGRFs and at least one trial of augmented feedback training.
An athlete’s responsiveness to augmented feedback training appears to be different based on an athlete’s baseline vGRF in landing. Heinert et al.24 observed when dividing participants into quartiles according to their baseline peak vGRF, those in the highest quartile, with an initial vGRF ≥ 4.30 times BW displayed a 32% reduction in their peak vGRF while those in the lowest quartile (vGRF<3.77 BW) demonstrated only a 15% decrease in vGRF. Those who showed such small improvements after training were largely unchanged during the transfer task suggesting that there may be limited efficacy for some individuals as they had minimal room for improvement. This quartile data was used to inform our threshold for those athletes who appeared to have greater room for improvement in reducing vGRF. Similarly, athletes were classified in this manner who exhibited a reduction in vGRF > 0.25 BW from augmented feedback training. This was based on Heinert et al.28 who reported the retention in the reduction of vGRF > 0.25 BW after the completion of 4 weeks of augmented feedback training. Considering these distinct differences in responses of athletes, terminology that refers to these differences can be introduced. A “responder” referred to an athlete who responded favorably to augmented feedback and a “non-responder” referred to an athlete who displayed minimal to no change following the training intervention.29 When utilizing both metrics (vGRF and change in vGRF from a single session of augmented feedback training), an athlete’s likelihood of vGRF improvement during the post-feedback block and transfer task block was greater.
Most athletes were classified as high baseline-responders (HB-R) (n=107) and appeared to respond favorably to a single session of augmented feedback training to reduce vGRF. Kiminski et al.30 similarly used augmented feedback with Division III female collegiate athletes that explored deceleration with landing during a sport-specific movement (blocking for volleyball or rebounding for basketball) both before and following training. These individuals reported a 0.63 g or 11.5% reduction in the mean peak deceleration following training, reflecting the additional transfer to a more game-like activity related to vGRF.
Myer et al.18 (2013) reported female athletes under the age of 18 demonstrated a larger reduction in risk (72%) compared to those over 18 years old who had a risk reduction of 16%. Their risk was determined by evaluating biomechanical abnormalities in landing mechanics such as increased knee valgus, diminished trunk stability, and increased lateral trunk motion. Their data supports the notion that there may be a particular age range where skill acquisition and aptitude for skill refinement may be optimal and that this may occur before the integration of neuromuscular deficits and maturation. The augmented feedback training provided for these individuals may be effective based on their baseline landing performance as well as their concurrent affinity for improvement during training. The athletes classified in our study demonstrated a near 50% reduction in vGRF on the post-test and readily responded to augmented feedback within training block 1. There seems to be a large portion of athletes who may benefit and respond to augmented feedback training.
Additionally, 17 athletes were classified as “low baseline vGRF” and were deemed less likely to benefit from augmented feedback training, but still showed changes greater than 0.25 BW (low baseline-responders (LB-R)). This group showed a lower magnitude of change overall with augmented feedback training and showed posttest and transfer task vGRF values nearly identical to the low baseline-non-responder (LB-NR) group. Although on average this group showed a reduction in vGRF of nearly 18% it is uncertain how this may translate to reducing injury risk given their low baseline vGRF. Thus, the utility of this type of augmented feedback training in this group remains an area to further investigate.
Low baseline-non-responders (LB-NR) athletes (n=12) had a low vGRF during baseline testing, so there was likely a floor effect regarding their ability to improve beyond these relatively low-impact values. These athletes appear to be non-responders to augmented feedback training; however, they also may be at relatively low risk due to the reported inverse relationship between vGRF and ACL injury risk.11,19,31 These athletes may not require much, if any, drop landing augmented feedback training to reduce their vGRF.
The high baseline-non-responders (HB-NR) athletes (n=11) did not demonstrate marked improvement with augmented feedback trials despite having high baseline vGRFs. These athletes may require additional attention. It is possible they may need more augmented feedback training, another type of training or feedback mechanism, or may have other impairments (i.e., lack of strength or proprioception) that preclude their ability to respond to a single session of training. A meta-analysis by Sugimoto et. al.32 reported a larger volume, characterized by both session duration and frequency, of preventative training (>30 min/week) increased the effectiveness of ACL injury risk reduction. As such, these individuals may benefit from additional practice or assessment. However, it may be worth noting, that the studies analyzed in this meta-analysis provided intervention throughout an entire pre-season and/or season. As such, while we’re addressing peak vGRF, the further assessment of neuromuscular control may require supplementary evaluation of other constructs, such as gross multi-directional hip strength,33 quadriceps limb symmetry index,34 and rate of force development.34 More robustly evaluating female athletes may require multi-modal interventions to ameliorate injury risk.
While the ideal integration for more autonomous motor learning would require a robust multi-session program, the time and financial cost of this approach makes this less feasible for universal integration in high school sports. The proposed single-session evaluation and augmented feedback training may provide a targeted means to stratify those who better respond to such training based on their specific presentation. Equipping adolescent athletes, their coaches, strengthening and conditioning staff, and athletic trainers with data that identifies “responders” and “non-responders”, may allow better understanding of each athlete’s landing performance. Assessing baseline vGRF and response to initial augmented feedback training appears to be a feasible avenue to identify those most responsive to training and those who may benefit from additional evaluation or intervention within a single session.
LIMITATIONS
This study was performed over a single session with the inclusion of a transfer task block to assess for carryover of learning into a more game-like scenario; however, without a follow-up retention measure at a secondary point in time, the long-term efficacy of the augmented feedback training is speculative. Heinert et al.28 performed a study with a similar training protocol that examined the efficacy of a four-week training program on retention in NCAA Division III volleyball players, who were able to demonstrate week-to-week carryover, with an overall 28.8% reduction in vGRF.
In this sample of female athletes, it is unknown how many, if any, of the athletes incurred an ACL injury throughout the year. However, this was not the point of this study developed to assess ACL injury risk mitigation, and injury data were not collected. Finally, the methodology did not include a control group, so the performance improvements may be due to the augmented feedback training, further investigation may be needed using a randomized controlled trial design.
CONCLUSION
Assessing baseline vGRF alone does not entirely capture who may or may not respond to augmented feedback training. The combination of baseline vGRF and change in vGRF during augmented feedback training may be used to identify those most apt to respond to a single session of training, and those who may require further evaluation and/or focused training beyond augmented feedback. These findings may be important to sports health professionals regarding the implementation and use of augmented feedback training for female athletes related to ACL injury risk mitigation during landing.