





INTRODUCTION
Throughout every level of overhead athletics, upper extremity injuries are a common occurrence. Given its high injury rates, few overhead sports have been researched as much as baseball. At the collegiate and professional levels, shoulder pathology accounts for up to 35% of all baseball-related injuries,1–3 with pitchers making up as much as 60% of injured players.4 Elbow pathology in this population accounts for 7-16% of all injuries,3 with pitchers making up 40% of injured players.5 At the high school level, injury surveillance studies estimate that shoulder pathology accounts for 13-21% of all baseball-related injuries, with pitchers making up 40% of injured players.6,7 Elbow pathology in this population is estimated to account for 11-12% of all injuries, with pitchers making up 60% of injured players.6,7
With the significant prevalence of shoulder and elbow injuries, much attention has been given to the upper extremity in rehabilitation and prevention strategies.8–11 However, despite the fact that the overhead throwing motion has been well-established as a full-body kinetic chain motion, less attention seems to be paid to the trunk and lower quarter in the clinical setting. The intention of this current concept review is to highlight the importance of the trunk and lower extremity in mitigating load through the upper extremity in the overhead athlete. With this knowledge, clinicians can better evaluate and treat the entire throwing athlete, not just the injured segment.
THE KINETIC CHAIN: HOW IT IMPACTS THE UPPER EXTREMITY
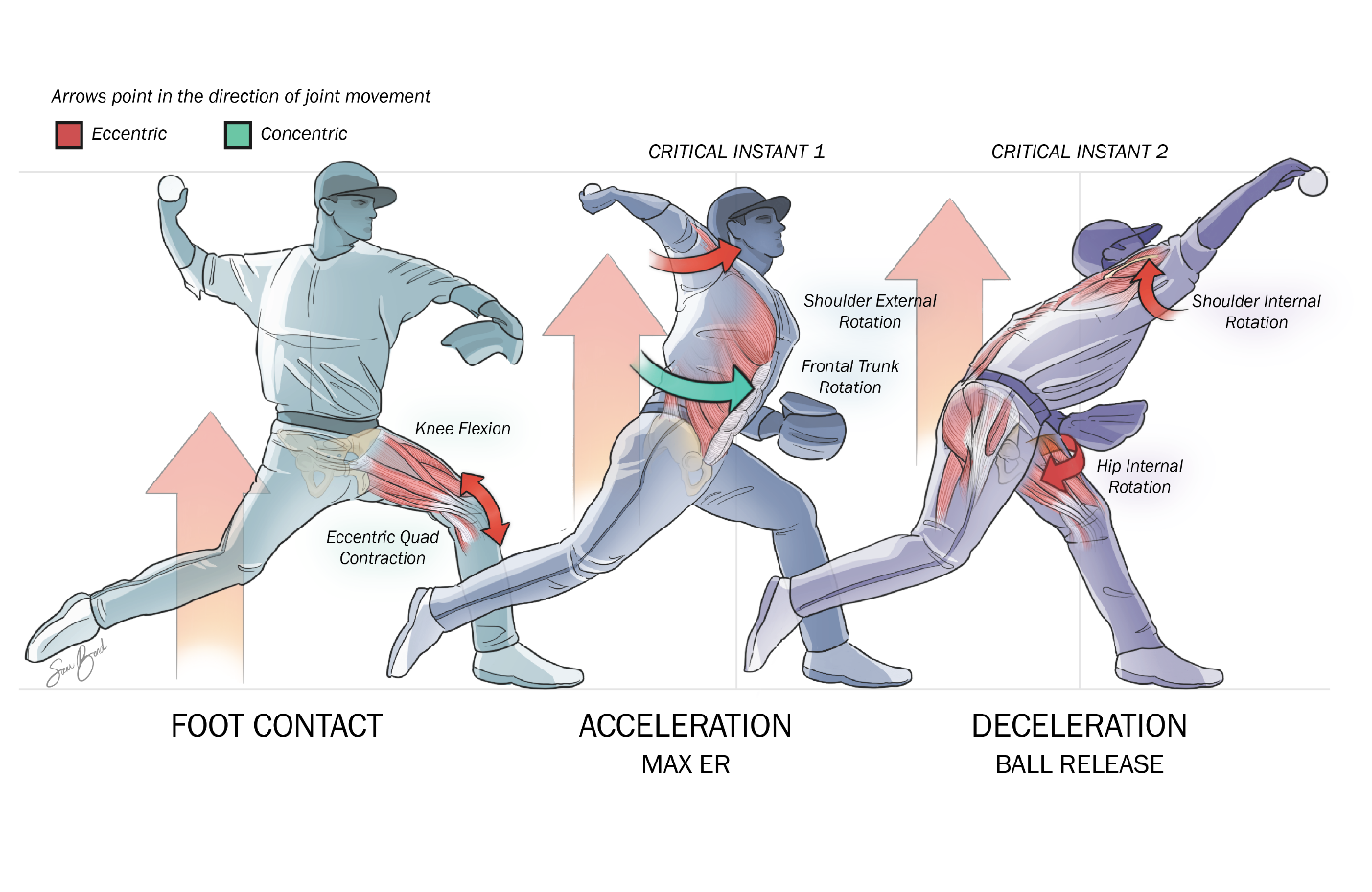
The impact of the kinetic chain in the overhead throwing motion was detailed by Atwater et al. in 1979, discussing how the larger, slower moving proximal segments of the lower extremity and trunk progressively developed kinetic energy that was later released by the smaller, rapidly-moving distal segments of the arm.12 Subsequent research would later organize the throwing motion into six phases: wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow-through.13 In 1995, Glenn Fleisig highlighted two “critical instants” of the throwing motion in which the upper extremity undergoes the greatest stress: just before maximum external rotation and just after ball release (Figure 1).14 Years later, Aguinaldo and Escamilla further elaborated on the impact these proximal segments had on the upper extremity in their study on segmental energy flow through the kinetic chain.15 In this study, they found that trunk rotation power played a significant role in the development of elbow valgus torque and ball speed. By synthesizing these descriptions of the kinetics and kinematics of the overhead throwing motion, we can better understand the impact that the trunk and lower extremity has on the performance and injury risk of the upper extremity. In the past decade, several studies have offered insight into how impairments of the trunk and lower quarter in each phase of throwing can impact the upper extremity.

Wind-Up
The wind-up phase of the throwing motion, occurring from a position of rest to the position of maximum lead leg lift, is the phase in which the athlete prepares the body to generate force. Since the athlete is in a position of single leg stance, lumbopelvic control is paramount in this phase. As described by Chaudari et al., throwing athletes demonstrating decreased lumbopelvic control in single leg stance were significantly more likely to miss over 30 days of a baseball season due to injury.16 Similarly, Laudner et al. found that decreased lumbopelvic control on an athlete’s drive leg was correlated with increased torque at the anterior shoulder and medial elbow.17 These data underscore the importance of lumbopelvic stability on the drive limb during the windup phase of throwing.
Stride
The stride phase of the throwing motion, occurring from the position of maximum lead leg lift to the position of front foot contact, is the phase in which the athlete uses their drive leg to propel their body toward home plate. During this phase, as the drive limb is pushing laterally against the pitching rubber to initiate the propulsion toward home plate, strength of the drive leg hip abductors is of considerable importance. Laudner et al. compared hip performance in position players versus pitchers in professional baseball and found that pitchers exhibited significantly decreased drive leg hip abductor strength compared to position players, requiring increased demand on the trunk and upper extremity to generate force.18 This strength deficit takes on greater importance when considering a study by Hamano et al. that found that high school pitchers experiencing an upper extremity injury were significantly more likely to present with decreased hip abduction strength of the drive limb compared to their uninjured peers.19 Drive leg hip abduction strength has been shown to impact performance as well, as peak ground reaction force (GRF) of the drive leg is strongly associated with ball speed.20 This suggests that a stronger push off the pitching rubber via hip abduction increases pitch velocity. These studies highlight the importance of hip abduction strength to optimize lower extremity contribution to the throwing motion.
Arm Cocking
The arm cocking phase of the throwing motion, occurring from the position of front foot contact to the position of maximum external rotation of the shoulder, is the phase in which the kinetic energy developed through lower extremity and trunk motion is transferred to potential energy of the shoulder. In other words, the energy developed from the legs, which has been augmented and transferred by the trunk, is now ready to be released from the arm through elastic energy. During this phase, the lead leg experiences considerable eccentric loading as it accepts the force of the body as it accelerates toward home plate. As a result, knee flexion at front foot contact has been identified as an important link in the kinetic chain. Chalmers et al. indicate that knee flexion angle at front foot contact was significantly correlated with shoulder and elbow strain.4 A strong eccentric quadriceps contraction of the lead leg is required to provide a braking impulse and allow propagation of energy up the kinetic chain from the legs to the trunk.21,22 Inadequate braking impulse alters the timing of trunk rotation, potentially leading to increase strain at the anterior shoulder and medial elbow.15 These studies underscore the importance of lead leg strength and eccentric control to promote the transfer of energy up the kinetic chain and to maintain optimal timing of trunk rotation.
Arm Acceleration
The arm acceleration phase of the throwing motion, occurring from the position of maximum external rotation of the shoulder to the position of ball release, is the phase in which kinetic energy generated by the body is transferred to the ball. When beginning in the position of maximum shoulder external rotation, the first of Fleisig’s two aforementioned “critical instants” occurs, as there is significant internal rotation torque at the shoulder, valgus torque at the elbow, and anterior force at the humeral head on the glenoid.14 Trunk motion is the key for generating power in the throwing motion, highlighting the importance of trunk rotation mobility, strength, control, and timing. Aguinaldo and Escamilla found that roughly 86% of the total energy transferred through the elbow during the throwing motion was due to trunk motion.23 Other researchers have also found that high school pitchers do not generate as much trunk rotation as professional pitchers, resulting in increased strain to the shoulder and elbow during acceleration.15,24 Trunk motion in the frontal plane during the throwing motion has been found to significantly impact strain to the upper extremity as well, and Oyama et al. found that increased contralateral trunk tilt during the acceleration phase was associated with increased velocity as well as increased joint loading to the upper extremity.25 Subsequently Solomito et al. found that increased contralateral trunk tilt resulted in only a 1.5% increase in ball velocity, but a 3.2 and 4.8% increase in anterior shoulder and medial elbow torque, respectively.26 These validate the importance of trunk motion related to developing elbow torque and ball velocity.
Arm Deceleration and Follow-Through
The arm deceleration phase of the throwing motion, occurring from the position of ball release to the position of maximum shoulder internal rotation, is the phase in which the arm must decelerate after a full-body acceleration. The follow-through phase is a continuation of this deceleration, but at lower speeds. When beginning in the position of ball release, the deceleration phase is where the second of Fleisig’s two “critical instants” occurs, as the posterior shoulder is placed under large stresses to decelerate the arm and resist distractive force.14 Just as accelerating the upper extremity in preparation for ball release was a result of the kinetic chain, deceleration of the upper extremity after ball release will require the kinetic chain as well. During this phase, the athlete is decelerating their body over the lead leg in single leg stance. As such, adequate hip internal rotation range of motion is needed to decelerate the trunk and pelvis over a stationary femur. Several studies have investigated hip range of motion norms among pitchers, with 30-35° of hip internal rotation being commonly described amongst healthy individuals.27,28 Decreased hip internal rotation has been correlated with hip, groin, back, and abdominal injuries in professional pitchers27,28 which suggests that an inability to decelerate over the lead leg may put more stress on the trunk to decelerate the upper extremity following ball release.
With this detailed understanding of how deficits along the kinetic chain can impact the upper extremity, clinicians can better evaluate the throwing athlete and create a plan of care that will mitigate injury risk and optimize performance.
EXAMINATION OF THE KINETIC CHAIN
Considering the importance of the aforementioned trunk and lower extremity contributions to the throwing motion in an overhead athlete, it is imperative that a systematic and comprehensive physical examination be conducted. This manuscript will highlight tests that can be performed in a “traditional” clinical setting without access to advanced testing equipment (motion capture, force plates, etc.). Various tests of range of motion, muscle performance testing, proprioceptive/kinesthetic testing, upper extremity functional performance tests and qualitative functional movement performance assessment will be listed.
When examining the entire kinetic chain, the concept of “Test, Don’t Guess” applies. The primary reason being that the kinetic chain is a complicated link system and if there is a deficit at one link in the kinetic chain it can impair performance of the movement pattern. The only way to determine if there are potential deficits is to test using appropriate methods and techniques.
Although the shoulder complex and elbow receive a lot of attention due to the significant injuries that occur with pitching, as indicated throughout this manuscript, various components of the kinetic chain can be a major cause or a contributing factor to the high-profile injuries.
A classic example of the impact of the kinetic chain is the case of Dizzy Dean, a Hall of Fame pitcher from the 1930s.29 In 1937, Dean was struck in the foot by a line drive, fracturing his great toe. This injury and the subsequent impairments resulted in altered throwing mechanics leading to an eventual career-altering arm injury. This example highlights the need to evaluate the pitcher and the kinetic chain “from the toes to the nose” as the Dizzy Dean injury illustrates what can stem from an impairment very distant from the shoulder. Specifically, Dean’s injury demonstrates the significance of evaluating the lower extremity range of motion of specific joints. Because of the function of the hip extensors contributing to the power of the acceleration and the quadriceps eccentrically contracting during the deceleration phase, a thorough exam includes evaluation of the muscle performance of the entire kinetic chain.
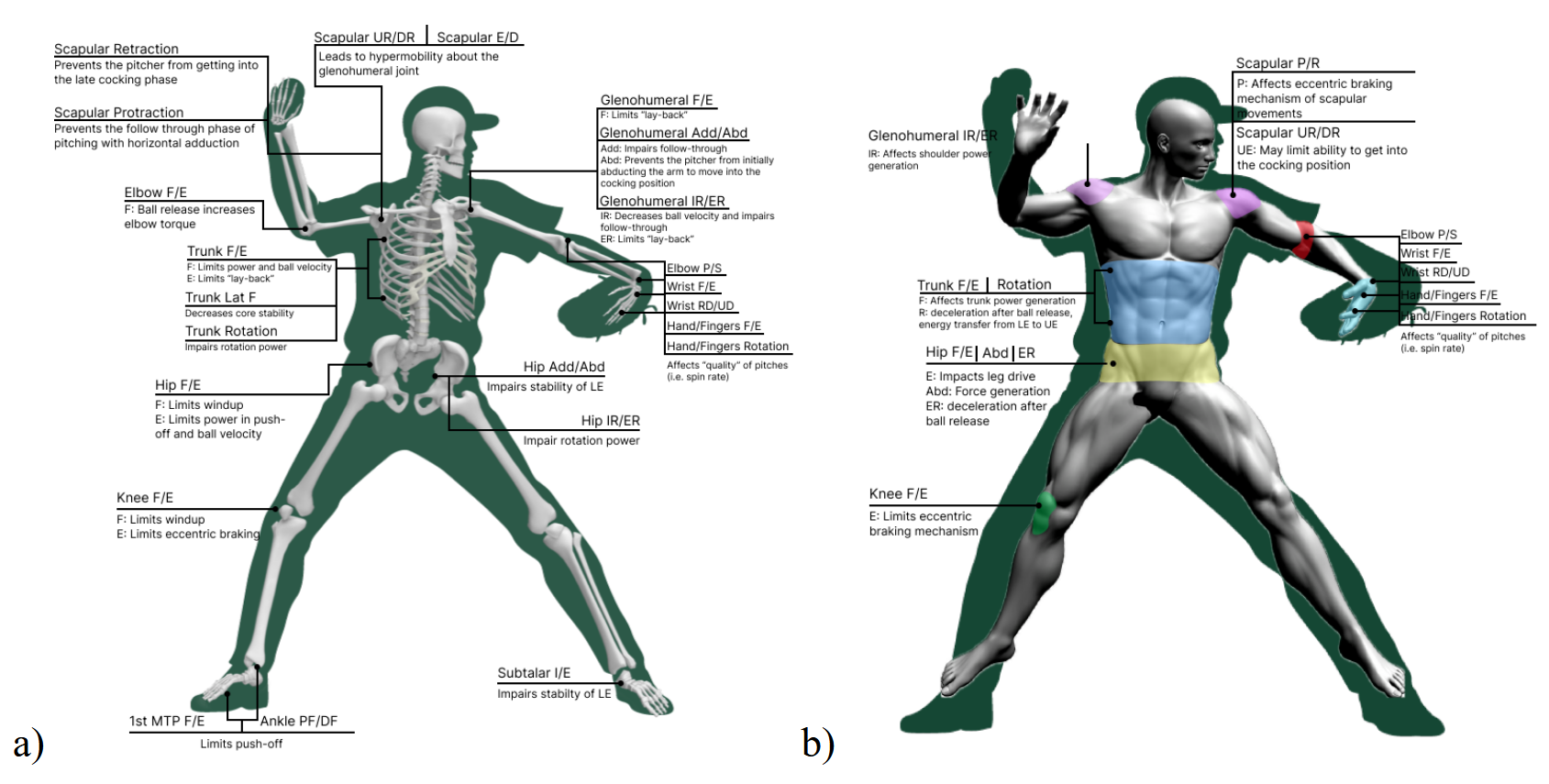
The frequency of oblique strains occurring in pitchers is another example of the need to evaluate the entire kinetic chain.30–32 In this case, the trunk/core needs to be evaluated for range of motion, flexibility, and muscle strength. Tables 1-4 provide specific details of various assessments that can be used throughout the kinetic chain and the potential effects on performance. Figure 2 features the mobility and strength considerations at various points along the kinetic chain.
_mobility_considerations_at_each_joint_along_the_kinetic_chain._(b)_muscle_strength_con.png)
INTERVENTIONS ADDRESSING TRUNK AND LOWER EXTREMITY IMPAIRMENTS
While distinct impairments are commonly seen in pitchers, it is vital that clinicians pursue treatment only after a thorough history and physical examination. Interventions must be targeted to each athlete; otherwise, cognitive biases such as availability bias, anchoring bias, confirmation bias, authority bias, and illusory correlations will lead to a shotgun approach to interventions. For example, if lumbopelvic or lower extremity impairments are discovered, they must receive as much attention, if not more, than anything in the upper quarter. A regional approach to treatment is important for these athletes.
Trunk and Hip
Trunk motion (thoracic, lumbar, and pelvic) is key to generating power. Without adequate motion in the various components of the kinetic chain, joints above and below the hypomobility are likely to become hypermobile as a means of compensation. If impairments are found with thoracic extension and rotation, clinicians are encouraged to consider the use of thoracic mobilization/manipulation, self-mobilization, assisted ROM in quadruped, and dynamic ROM (Figure 3). Particular attention should be paid to the soft tissue as well, including, but not limited to, the length of the hip flexors and hip rotators. Soft tissue deficits can often be addressed by dry needling, soft tissue mobilization, instrument-assisted soft tissue mobilization, and/or with active or passive stretching.
_supine_grade_v_thorac.png)
If the athlete has adequate trunk mobility but appears to be lacking stability, the authors recommend assessing and treating the trunk in all planes, with an emphasis on the transverse plane. While the trunk may have sufficient ROM and control in the frontal and sagittal planes it is not uncommon to lack rotational control. In these cases, clinicians are encouraged to focus on foundational movement patterns such as segmental rolling (Figure 4) pelvic diagonals, and/or proper pelvic floor recruitment before moving to more advanced interventions. Segmental rolling can also be progressed by shortening the lever arm used by the patient (Figure 5). Long-moment isometrics, such as resisted bird dogs, Pallof press, sustained battle ropes, or corrective side planks are examples. Cardinal plane movements, such as a prone extension progression, landmine press, and/or overhead squats can then be considered. In the final phase of interventions aimed at improving trunk-related impairments, power production should be emphasized using explosive medicine ball training, Turkish getups, and explosive diagonal squats and lifts. Regardless of the naming convention used to describe the exercise, trunk interventions should follow a logical progression, starting with mobility followed by motor control, isometrics, cardinal plane activities, transverse plane activities, and finally, interventions aimed at improving power.


Hip rotation is imperative for both acceleration (external rotation) and deceleration (internal rotation) during the throwing motion. If the deficit articular in nature, long axis hip distraction, lateral distractions, and lateral distractions with ER and IR can be effective. Prone pelvic mobilizations with the femur positioned in internal rotation (mobilizing pelvis on femur) as shown in Figure 6 (to restore hip internal rotation). Self-mobilizations, such as an inferior-posterior glide with step back, lateral femoral glides, and kneeling rotation with active internal rotation58 serve as a home exercise program to reinforce the ROM gained via manual therapy in the clinic. Finally, active exercises using the new ROM are imperative and can include shin box hip thrust (sitting exercise emphasizing internal rotation of one leg and external rotation of the other), hip controlled articular rotation (CARS), plie squats, etc.

If the athlete is found to demonstrate decreased lumbopelvic control in single leg stance, it is recommended that the athlete be progressed through a drop squat progression similar to that reported by Andreyo et al.59 If a pitcher demonstrates reduced strength of their drive limb hip abductors, a targeted strengthening and neuromuscular program should be implemented. While classic exercises such as clamshells, side-lying hip abduction, “monster walks” and unilateral standing hip abduction effectively target the weakened musculature, it is unlikely there will be sufficient carryover from these interventions into the throwing motion. The authors recommend initiating a strength and neuromuscular progression using a side-lying technique in which the athlete learns the movements associated with anterior elevation of the pelvis (Figure 7) followed by posterior depression of the pelvis (Figure 8). Once the athlete has adequate proprioception and motor control of the hip, the athlete should be progressed to more weightbearing and pitching-specific interventions, such as resisted abduction using a SportCord® (JDP Products, Peoria, AZ), resisted abduction with rotation using a SportCord®, and breakaway abduction with resistance using a SportCord®. Explosive side hops, side-lying hops on a Shuttle, and explosive resisted single leg squats all serve appropriate advanced interventions.


Knee
Arguably the most common knee-related impairment seen in pitchers is that of a loss of lead leg eccentric quadriceps control. It is this eccentric braking mechanism of the lead leg that contributes to the transition of linear power created by the drive leg to angular power. This transition occurs as the lead leg serves as an “anchor” over which the body rotates, creating a “catapult” effect of the trunk and arm.60–62 Furthermore, if the pitcher lacks eccentric control of the lead leg, this will limit the braking mechanism needed to quickly and efficiently position himself in a ready position after he throws the ball. Additionally, the lack of force attenuation will place additional stress on the articular cartilage and meniscus, possibly increasing a pitcher’s risk of injury. Interventions to address this should start with loaded bilateral squats, focused on the deceleration phase, progressing to single leg squats. The athlete should be quickly progressed to more demanding and sport-specific interventions including plyometric training emphasizing the deceleration/eccentric phase as well as lateral movements that mimic the throwing motion.
Ankle and Foot
A lack of dorsiflexion ROM, as well as a loss of great toe extension, are deficits commonly seen in pitchers. While these deficits may appear insignificant at first, a prospective cohort study of 228 baseball players found that a loss of trail leg dorsiflexion strongly correlated with shoulder and elbow injuries in youth baseball players.63 Additionally, a loss of dorsiflexion ROM has been shown to have a strong influence on dynamic balance.64 Manual therapy aimed at improving closed chain dorsiflexion should include ankle long axis distraction, posterior talar glides, lateral tibial glides, and mobilizations with movement using a strap/belt (Figure 9). Self-mobilizations can serve as a great means to reinforce manual therapy delivered in the clinic. Kneeling knee-to-wall mobilizations, mobilization with movement with talar fixation, and rearfoot eversion self-mobilizations are all paramount to restoring and maintaining closed chain dorsiflexion. Soft tissue deficits can often be addressed via dry needling of the gastrocnemius and/or soleus, soft tissue mobilization, instrument-assisted soft tissue mobilization, and with active or passive stretching. Finally, active exercise should be utilized in order to develop new motor patterns. Active exercises emphasizing closed chain dorsiflexion include lunges, deep squats, heel raises off a step, and single leg Romanian deadlifts with a wedge under the forefoot. A loss of great toe extension can be addressed in a similar fashion via manual therapy followed up by a home self-mobilization program, soft tissue treatment, stretching, and finally, active engagement of the gained ROM.
_long_axis_d.png)
Looking Beyond ROM & Strength
While evaluation and treatment of mobility and strength deficits are critical to both the prevention and treatment of injuries in pitchers, clinicians should appreciate the neuroplastic changes that occur in overhead athletes both before and after an injury. Clinicians should consider incorporating reactive neurocognitive (RNC) testing and treatment into an athlete’s testing and treatment. These tests should be dynamic, sport specific, non-invasive, and require reactive agility.65 They can assess reaction time, attention, memory, perception, as well as a player’s ability to multitask.65 Recently, a testing battery was proposed by Wilk et al. which includes: 1) reactive closed kinetic chain upper extremity test (CKCUEST+); 2) reactive triangle CKCUEST+; 3) reactive right vs. left CKCUEST+; and 4) reactive OKC 90/90 wall throws. Neurocognitive tests utilizing reactive agility pods such as Blaze Pods (Blaze Pods, Tel Aviv, Israel) can quantify athlete speed, reaction time, left to right asymmetries, etc. Should deficits be discovered through the testing, interventions must be tailored accordingly. Often, the plan of care can simply be modified, as opposed to overhauled, to meet the athlete’s specific needs. Emphasis can be placed on dual-tasking, dyad training, reacting to an unpredictable stimulus, or completing the activity with different visual stimulus.
KEEPING EVERYTHING IN PERSPECTIVE
While the authors strongly believe that the trunk and lower extremity are grossly under-evaluated and treated in baseball players, it would not be wise to not bring to light the fact that the biggest predictor of injuries in pitchers is not necessarily biomechanical but is likely overuse. As such, readers are encouraged to digest this information with the healthy understanding that preventing and treating injuries goes far beyond range of motion, strength, and pitching technique. Every component of the kinetic chain as well as biopsychosocial considerations, and training loads must be addressed: neglecting any one of these factors, may lead to decreased performance at best and injury at worst.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to express their sincere thanks to Sam Bond (Figure 1) and Emily Schaedle (Figure 2) for their contributions of original artwork within this commentary.