


Introduction
Lateral elbow pain is a frequent complaint in clinical practice, with diverse etiologies that range from overuse injuries to degenerative and inflammatory conditions.1–3 Accurate diagnosis is pivotal to tailoring effective rehabilitation interventions. Musculoskeletal ultrasound (MSKUS) has gained prominence as a diagnostic modality due to its ability to provide real-time, high-resolution imaging of soft tissues, including tendons, ligaments, and nerves, without the radiation exposure inherent in other imaging techniques. This article explores the application of MSKUS in evaluating lateral elbow disorders, focusing on its diagnostic capabilities, procedural benefits, and integration into rehabilitation settings.
Anatomy of the Lateral Elbow
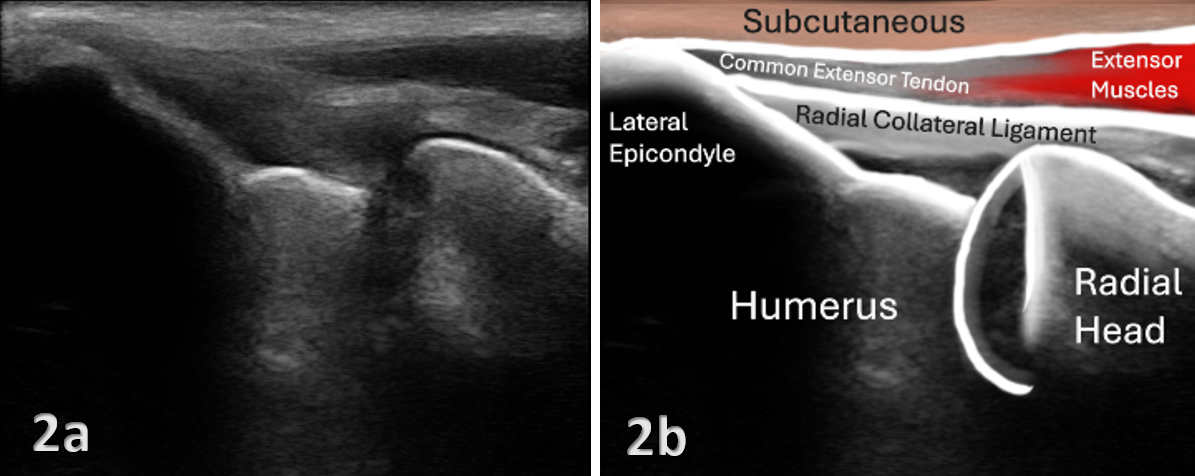
Understanding anatomy is essential for accurate ultrasound evaluation. The lateral elbow comprises several key structures, including:
-
The lateral epicondyle of the humerus, serving as the origin for the common extensor tendon (CET).
-
The radial collateral ligament complex providing lateral stability.
-
The radial head and its articulation with the humerus and ulna.
-
Adjacent neurovascular structures, including the radial nerve.
Benefits of MSK Ultrasound
MSKUS offers several benefits in the assessment, diagnosis, and management of lateral elbow pain.
-
Real-Time Imaging: Compared to other imaging modalities, MSKUS enables dynamic assessment and immediate correlation with clinical findings. Standardized protocols for static4 and dynamic5 elbow assessment are available.
-
High Resolution: MSKUS is excellent for superficial structures like tendons and ligaments, making it an ideal imaging modality for lateral epicondylitis.6
-
Cost-Effective and Accessible: Compared to magnetic resonance imaging (MRI), MSKUS is more widely available and affordable. Researchers reported moderate agreement of MSKUS with MRI in detecting tears of the CET.7
-
Guidance for Interventions: MSKUS facilitates precision in procedures such as corticosteroid injections or platelet-rich plasma (PRP) therapy.8
Common Pathologies of the Lateral Elbow
MSKUS provides clear visualization of the anatomical details required for precise diagnosis, which is critical for forming appropriate rehabilitation strategies. Several pathologies can cause lateral elbow pain.
-
Lateral Epicondylitis: Characterized by degeneration of the extensor carpi radialis brevis (ECRB) tendon, lateral epicondylitis is the most prevalent cause of lateral elbow pain.9–11 MSKUS can reveal tendon thickening, hypoechoic regions, and neovascularization, providing critical insights into the extent of tendon pathology. Dynamic scanning5 can aid in identifying pain generators.
-
Tendon Tears: MSKUS is adept at identifying partial tendon disruptions and other degenerative changes. Sensitivity, specificity, and accuracy of MSKUS in detecting CET tears were reported as 64.5%, 85.2%, and 72.2%, respectively.7
-
Radial Collateral Ligament, or Lateral Ulnar Collateral Ligament Injury (Posterolateral Rotatory Instability)12–14: MSKSUS can identify ligamentous sprains or tears through visualization of discontinuity, thickening, or hypoechoic changes in the ligament. Varus stress testing during ultrasound can confirm functional instability.
-
Radial Tunnel Syndrome15–17: MSKUS aids in the evaluation of compression or irritation of the posterior interosseous nerve, often caused by fibrosis or muscular hypertrophy.
-
Olecranon Bursitis and Synovitis18–20: Fluid accumulation and synovial thickening in bursae can be detected with MSKUS, allowing differentiation between inflammatory and infective processes.
-
Elbow Fractures: Fluid accumulation demonstrating a lipohemarthrosis is children with acute elbow fractures may be seen.21,22 However, poor ultrasound penetration through bone makes it difficult to fully characterize the type of fracture.
Ultrasound Techniques for the Lateral Elbow
MSKUS imaging of the lateral elbow involves proper positioning, probe selection, and protocol selection (see Figures 1–3).
-
Patient Positioning: The patient is seated with the elbow flexed to 90 degrees, the forearm pronated or supinated depending on the target structure, and the hand resting on a flat surface. This position optimizes exposure of the lateral elbow structures.
-
Probe Selection: A high-frequency linear transducer (10-15 MHz) is recommended for optimal resolution.
-
Scanning Protocol:
-
Extensor Tendon Evaluation: Place the transducer longitudinally over the lateral epicondyle to assess the common extensor tendon for hypoechoic areas, calcifications, or tears. Longitudinal and transverse views of the ECRB and extensor digitorum tendons are essential.
-
Radial Collateral Ligament: Scan the lateral joint line in a longitudinal plane, looking for ligament thickening, disruptions, or instability during varus stress testing.
-
Nerves: Trace the posterior interosseous nerve for evidence of entrapment.
-
Dynamic Assessment: Real-time imaging during active or resisted movements aids in diagnosing subtle abnormalities, such as snapping syndromes or dynamic nerve impingement.
-
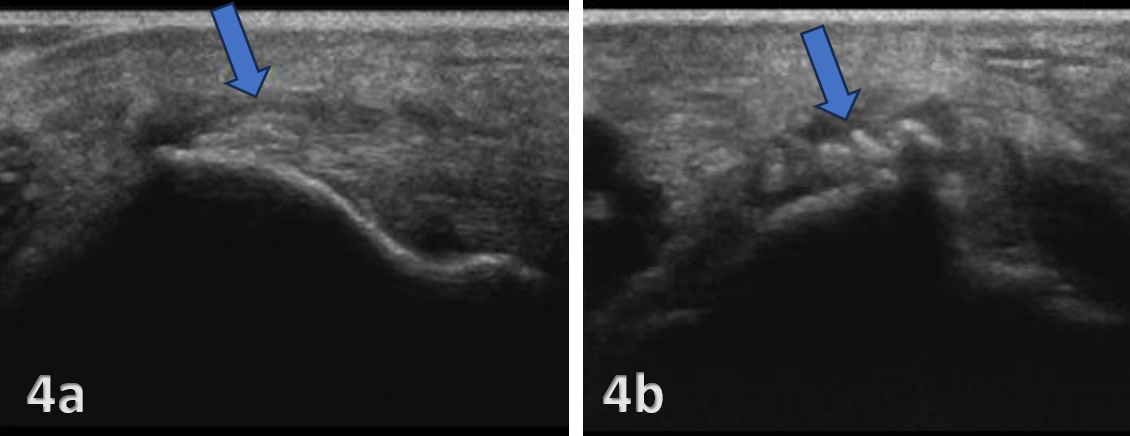
Figures 4 and 5 demonstrate lateral elbow pathologies.
Clinical Applications in Rehabilitation
MSKUS supports rehabilitation of lateral elbow pain through several methods:
-
Guiding Interventions: MSKUS enhances the precision of dry needling and injection therapies, including corticosteroids or platelet-rich plasma by confirming target localization.
-
Monitoring Progress: Periodic imaging allows for assessment of tendon healing, ligament repair, or resolution of inflammation, supporting adjustments to rehabilitation protocols.
-
Real-Time Feedback: Dynamic ultrasound enables visualization of biomechanical alterations during therapeutic exercises, facilitating biomechanical retraining.
Challenges and Limitations
-
Operator dependence: MSKUS is operator-dependent, necessitating adequate training and experience to achieve optimal diagnostic accuracy.
-
Limited visualization of deep structures: MSKUS is less effective for evaluating deep osseous or joint structures.
-
Artifacts: Improper technique can lead to imaging artifacts, potentially misguiding diagnosis.
Conclusion
MSKUS is an invaluable tool for rehabilitation providers managing lateral elbow conditions. Its ability to deliver high-resolution, real-time imaging facilitates accurate diagnosis, guides therapeutic interventions, and monitors patient progress. As expertise in MSKUS continues to grow, its integration into routine clinical practice promises to enhance the quality and outcomes of care for patients with lateral elbow pathologies. Future research should focus on standardizing ultrasound protocols and further exploring its efficacy in diverse rehabilitation settings.

.png)
.png)

