

INTRODUCTION
The shoulder is one of the most intricate joints in the human body owing to the interdependency of multiple bony segments and muscle groups. Functional tasks such as overhead reaching require adequate mobility and coordinated muscular control of the scapulothoracic, glenohumeral, acromioclavicular, and sternoclavicular joints to achieve full, functional range of motion.1,2 Disruptions in any aspect of the shoulder complex may interrupt the normal inter-joint coordination that is characteristic of normal upper limb function.
Observational evaluation of arm elevation is a routine part of the examination of patients with shoulder pain and dysfunction.3 Assessing arm elevation affords clinicians insight into an individual’s functional range of motion and movement quality. Importantly, observational assessment of arm elevation is necessary to identify movement impairments that should be considered when developing a treatment plan.
The interdependency of the glenohumeral and scapulothoracic joints during arm elevation presents a challenge for clinicians when attempting to characterize movement impairments and underlying causes. The assessment of arm elevation is further complicated by the fact that identification of movement impairments related to the scapulothoracic joint are easily observed (i.e. scapular winging or excessive scapular elevation) while movement faults at the glenohumeral joint (i.e. superior or anterior translation of the humeral head relative to the glenoid fossa) are more difficult to detect. As such, an inherent bias may exist in which clinicians prioritize movement impairments and associated physical impairments at the scapulothoracic joint in developing a treatment plan.
Because of the inherent interdependency of the glenohumeral and scapulothoracic joints, it is plausible that impairments at one joint could contribute to abnormal motion at the other. For example, abnormal scapular motion during arm elevation may be compensatory in nature owing to mobility or muscle performance impairments at the glenohumeral joint.4 This viewpoint differs from perspectives in which altered scapular kinematics are thought to be the primary cause of shoulder pain and disability.5,6 It is the authors’ contention that interpreting the cause(s) of abnormal scapulothoracic motion without considering the potential influence of the glenohumeral joint (and vice-versa) may lead to faulty clinical reasoning when developing a plan of care.
Given the complexity of the shoulder and the inherent challenges in the interpretation of the functional assessment of arm elevation, the purpose of this clinical commentary is to highlight the potential impact of faulty glenohumeral joint mechanics as being contributory to scapulothoracic joint kinematics. First the normal kinematics and muscular actions associated with typical arm elevation are reviewed, and then how impairments at the glenohumeral joint may be contributory to faulty scapulothoracic motion is discussed. Specifically, the authors address movement faults characterized by excessive motion of the scapula. It is hoped that this perspective will provide clinicians and researchers with a framework that can better inform the examination and treatment of various shoulder conditions.
FUNDAMENTALS OF ARM ELEVATION
For the purposes of this commentary, arm elevation will be discussed as shoulder motion in the scapular plane. Arm elevation occurs primarily through motions at the glenohumeral and scapulothoracic joints with accessory motions occurring at the acromioclavicular and sternoclavicular joints.5,7,8 While motions at the acromioclavicular and sternoclavicular joints during arm elevation are passive in nature, the glenohumeral and scapulothoracic joints are controlled by separate but interdependent muscular force couples. The muscular force couples at the glenohumeral and scapulothoracic joints produce coordinated motion between the scapula and humerus commonly referred to as scapulohumeral rhythm. A brief overview of the kinematics and muscular actions of the glenohumeral and scapulothoracic joint follows.
Glenohumeral Joint Kinematics & Muscular Actions
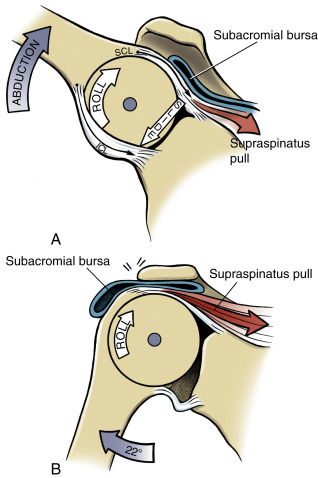
The glenohumeral joint is the largest contributor to arm motion during elevation. Shoulder elevation in the scapular plane requires the head of the humerus to glide inferiorly and roll superiorly (Figure 1). These motions prevent the humeral head from impinging on the coracoacromial arch and assist in maintaining an instant center of rotation throughout movement.9–11 Additionally, the humerus externally rotates within the glenoid fossa during arm elevation to avoid abutment of the greater tubercle and the acromion.12

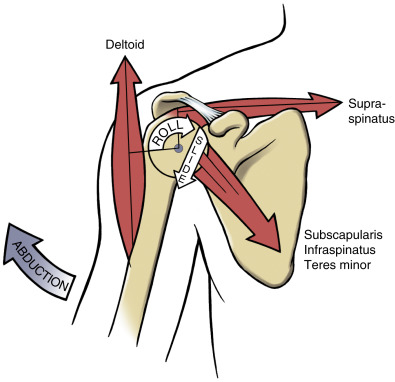
The muscles responsible for typical glenohumeral joint motion include the four rotator cuff muscles and the deltoid complex. While the deltoid is the prime mover of the humerus, the muscular actions of the rotator cuff provide the foundation by which the arm can elevate. The supraspinatus is particularly important for initiating the spinning action of the humeral head owing to its horizontal line of pull, while the infraspinatus and teres minor provide the external rotation motion of the humerus during arm elevation.13 The combined actions of the subscapularis, infraspinatus and teres minor counteract the superior translation of humeral head resulting from contraction of the deltoid owing to their downward lines of pull (Figure 2). Importantly, the lines of action of all the rotator cuff muscles stabilize the glenohumeral joint through medially directed compressive forces. Apart from the muscular forces, passive structures such as the joint capsule, ligaments, and labrum assist in guiding the intricate arthrokinematics of the glenohumeral joint.14,15

Scapulothoracic Joint Kinematics & Muscular Actions
In general, the scapula upwardly rotates and tilts posteriorly along the convex surface of the thorax as the arm elevates.16 These motions maintain broad surface contact with the rib cage to allow for force transfer from the upper extremity to the trunk.6,17 Scapular motions provide proper orientation of the glenoid fossa to ensure normal glenohumeral joint arthrokinematics as the arm moves overhead.18
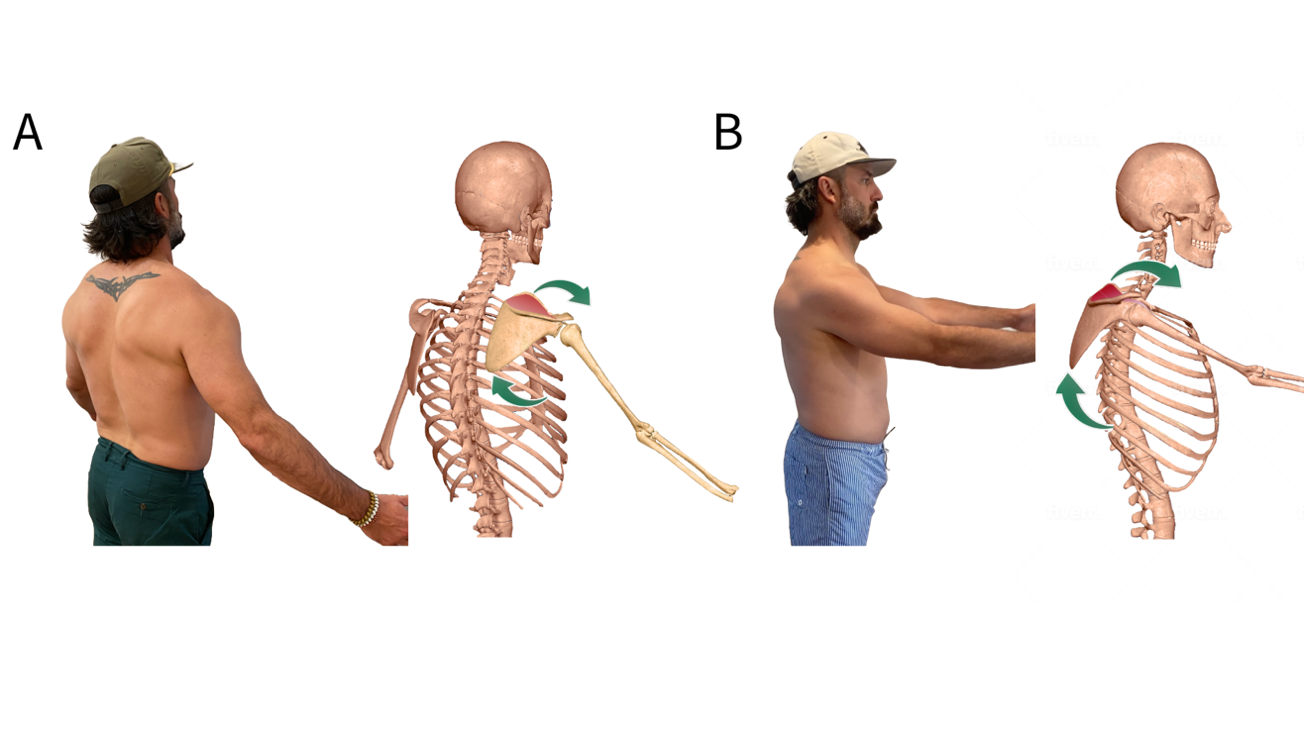
Motion of the scapula along the thorax during arm elevation is the result of a muscular force couple consisting of the upper and lower portions of the trapezius and the serratus anterior (Figure 3).8 Given its origin on the superolateral surfaces of the upper ribs, action of the serratus anterior maintains contact of the scapula against the thorax, thereby facilitating the motions of posterior tilt and rotation as the arm elevates.19 This force couple allows the scapula to upwardly rotate with overhead movement and functions to eccentrically control the scapula during arm lowering.

Scapulohumeral Rhythm
During the initiation of arm elevation (0-30°) motion primarily occurs at the glenohumeral joint.20 Little to no scapular motion is observed during this phase. Beyond 30° of arm elevation, the scapula upwardly rotates approximately 1° for every 2° of humeral elevation.21 The coordinated movement of the scapula and the humerus ensures that the length-tension relationship of the rotator cuff muscles is maintained throughout arm elevation.6 Importantly, scapulohumeral rhythm allows for the scapula to function as a moving base for the humerus thereby providing maximum stability as the arm moves overhead.
GLENOHUMERAL JOINT INFLUENCE ON ALTERED SCAPULOTHORACIC JOINT MOTION
There is evidence that altered scapular kinematics are present in individuals with a wide range of shoulder pathologies; however, underlying causes remain speculative and a source of debate.4,22 Specifically, authors have reported that individuals with various shoulder diagnoses exhibit excessive elevation, upward rotation, internal rotation, and anterior tilt.3,23 In the sections below, excessive scapular motions will be discussed in terms of possible glenohumeral impairments in which there is no apparent nerve involvement (ie. neuritis, neuropathy, or peripheral nerve injury).
Excessive scapular elevation & upward rotation
Inadequacy of the rotator cuff force couple has been hypothesized as being contributory to compensatory elevation and/or upward rotation of the scapula.4 Failure of the supraspinatus to provide the downward spinning action of the humeral head during the initiation of arm elevation owing to pain, injury and/or pathology could result in premature scapular elevation and upward rotation. These compensatory motions would serve to initiate arm elevation while preserving the subacromial space. (Figure 4)

The notion that excessive scapular motions during arm elevation could be the result of rotator cuff pathology was highlighted by a recent systematic review that examined the relationship between rotator cuff pathology and scapular dyskinesis.24 The summary of research in this area indicated that persons with rotator cuff tears (specifically supraspinatus) exhibited excessive scapular upward rotation, with greater motion impairments being present in persons with larger tears and those who were symptomatic. The presence of excessive scapular motions in persons with rotator cuff tears is consistent with the fact that superior humeral head migration is common in these individuals.3 Of note, several studies within this systematic review reported that abnormal scapular kinematics normalized following rotator cuff repair surgery, highlighting the fact that the excessive scapular motions observed pre-surgery may have been compensatory in nature to maximize arm function.27,28,29
As mentioned previously, the rolling and spinning action of the humeral head within the glenoid fossa is important to minimize abutment of the humeral head against the coracoacromial arch during arm elevation. In the presence of soft tissue restrictions or capsular tightness, the normal arthrokinematics of the glenohumeral joint can be impacted. In particular, the inability of the humeral head to translate inferiorly could result in the humeral head being positioned superiorly relative to the glenoid fossa. To maintain joint congruency and avoid abutment of the humerus against the coracoacromial arch, the scapula may be obligated to translate superiorly. Evidence in support of this premise is provided by studies that have reported persons with adhesive capsulitis exhibit significantly greater scapular elevation and upward rotation on the affected side when compared to the unaffected side.25,26 Additionally, Vermeulen et al. demonstrated that following the utilization of mobilization techniques to treat adhesive capsulitis, patients demonstrated a pattern of scapular motion that was closer to that of their unaffected side.26
Excessive scapular internal rotation and anterior tilt
As noted above, external rotation of the humerus is required during arm elevation to prevent abutment of the greater tubercle against the acromion.12 Glenohumeral joint impairments that may limit external rotation of the humerus include anterior capsular tightness/stiffness, shortness of the internal rotators of the humerus (ie. subscapularis, latissiumus dorsi, pectoralis muscles) and/or weakness of the posterior rotator cuff musculature (infraspinatus, teres minor). In the presence of limited humeral external rotation, the scapula may compensate through the combined motions of internal rotation and anterior tilt.27,28 These motions would result in relative external rotation of the humerus with respect to the scapula and allow for greater surface area contact between the glenoid fossa and head of the humerus. Excessive amounts of scapular internal rotation and anterior tilt could cause the medial border of the scapula to come away from the thorax, giving the appearance of scapular winging. (Figure 5)

Glenohumeral stability is necessary during arm elevation to keep the humeral head centered within the glenoid fossa. Asymmetric tension resulting from either hypermobility or hypomobility of the active and passive structures surrounding the joint can lead to excessive translations of the humeral head during arm elevation.29 Glenohumeral joint impairments that may impair stability include hypermobility of the joint capsule, impaired ligamentous or labral integrity, asymmetric anterior or posterior rotator cuff stiffness/tightness and/or disruption of the transverse plane force couple (ie. dynamic imbalance between the subscapularis and infraspinatus/teres minor). In the presence of anterior instability, the humeral head could be positioned anteriorly within the glenoid fossa. To maintain joint stability and congruency, the scapula may compensate through the combined motions of internal rotation and anterior tilt. This premise is supported by several studies that have reported an association between anterior glenohumeral joint instability and excessive scapular internal rotation.15,30–32 Regardless of the direction of instability, an argument could be made that compensatory motions of the scapula would be necessary to keep the humeral head centered within the glenoid fossa as the arm moves overhead.
SCAPULAR STABILIZATION EXERCISES: ADDRESSING THE SYMPTOMS OR THE ROOT CAUSE OF SHOULDER PAIN?
As presented above, it is plausible that abnormal scapular motions could be the result of glenohumeral joint impairments. This is not to discount the possibility however that scapulothoracic joint impairments (i.e. impaired muscular control of the scapula) could be contributory. As in the case with any form of movement analysis, the question as to whether the observed movement impairment is primary or compensatory needs to be considered.
Since the introduction of the concept of scapular dyskinesis in 1995, scapular stabilization exercises have been a mainstay of shoulder rehabilitation protocols.33–35 There have been several systematic reviews that have summarized the existing literature related to the efficacy of scapular stabilization exercises in reducing pain and disability in persons with various shoulder diagnoses.36–38 A consistent theme across these systematic reviews is that scapular stabilization exercises are effective in reducing shoulder pain and disability. Paradoxically, scapular stabilization exercises do not appear to result in a change in scapular kinematics, despite this being the intent.36,39–41
The disconnect between improvements in shoulder symptoms and the lack of corresponding changes in scapular kinematics is difficult to rectify. Exercises commonly prescribed to improve scapular stability (i.e. Y’s and T’s) require significant transfer of forces through the glenohumeral joint, owing to the long lever arm of the upper extremity.11 It is possible that the biomechanical demands of scapular exercises have an unintended positive effect on the glenohumeral joint in that they may provide a strengthening stimulus for the rotator cuff muscles, owing to the need for glenohumeral joint stability. In support of this premise, a systemic review by Edwards and colleagues reported that the supraspinatus and infraspinatus muscles exhibit a high-level of activation (75% and 64% of maximal voluntary isometric contraction respectively) during prone horizontal abduction.42
The high recurrence of shoulder pain in the general population highlights the fact that current treatment approaches for shoulder pain do not provide long-term benefits for many patients.43 Given as such, the underlying principles of shoulder rehabilitation may have to be re-examined. For example, the phrase “distal mobility requires proximal stability” is often used when devising an exercise program for patients with shoulder pain.44 While this statement may be suitable to describe functional movements of the arm, it may not be appropriate when designing an exercise program for shoulder pain.
Regardless of the cause-and-effect relationships between motions of the glenohumeral and scapulothoracic joints, a thorough assessment of the glenohumeral joint should be performed when faulty scapular kinematics are observed during arm elevation. Based on the arguments presented above, such an assessment should include an evaluation of rotator cuff strength and the presence of glenohumeral joint instability or hypomobility. Information obtained by the assessment of the glenohumeral joint should be considered when interpreting potential causes of abnormal scapular kinematics (if present).
CONCLUSION
Observational evaluation of arm elevation is an important element of the examination of the patient with shoulder pain. Due to the complexity of the shoulder owing to the intricate interaction of multiple joints and muscle systems required to achieve normal motion, teasing out cause and effect of the abnormal arm elevation is difficult. The purpose of this clinical perspective was to highlight the possibility that faulty scapular kinematics may be result of glenohumeral impairments. Clinicians should consider this possibility when prioritizing exercises for the patient who presents with shoulder pain and abnormal scapula kinematics. Although evidence exists to support the concepts presented in this clinical perspective, further research in this area is needed.
Conflicts of interest
The authors report no conflicts of interest.