INTRODUCTION
Anterior cruciate ligament (ACL) tears are common among athletes and other individuals who regularly engage in activities that involve landing, cutting, and pivoting.1–3 ACL reconstruction is generally recommended for those who plan to resume participation in these types of highly demanding activities.4 Following ACL reconstruction, patients typically complete extensive post-operative rehabilitation.5 During the earlier stages of rehabilitation, the primary focus is on controlling swelling/effusion, restoring knee motion, facilitating quadriceps activation, and promoting weight-bearing. As individuals progress, the focus shifts towards restoring lower body strength and control, and gradually transitioning to more demanding activities, such as jogging, jumping, and landing. The final phases of rehabilitation typically focus on preparing individuals to return to full activity (e.g. resumption of sport-specific activities for athletes).
Clearance to return to full activity following ACL reconstruction is typically based on multiple factors, including time since surgery, the demands associated with an individual’s sport/activities, an individual’s psychological readiness, and return-to-sport testing performance.6 Return-to-sport testing is typically conducted to gauge an individual’s physical readiness to resume their pre-injury activities by assessing lower body strength, power, and control.7 Hop tests are routinely conducted during return-to-sport testing to assess lower body power.8 For these tests, the individual is asked to perform single-leg hops for maximal distance with both their involved and uninvolved limbs, allowing clinicians to compare performance for the involved limb relative to the uninvolved limb. Although hop tests are just one component of a comprehensive return-to-sport testing battery, they can provide valuable insights regarding knee-related function.9,10
Despite advances in ACL reconstruction surgery and rehabilitation, long-term outcomes after ACL reconstruction remain suboptimal, as many individuals do not return to their pre-injury level,11,12 and those who do are at elevated risk of sustaining a second ACL injury.13–15 Therefore, it is important to understand factors that may impact recovery after ACL reconstruction. One factor that has received little attention is the presence of a concomitant meniscus injury, which often accompany ACL tears.16,17 When a meniscus tear has occurred, the injured region will typically either be surgically removed (partial meniscectomy) or repaired (meniscal repair), depending on the location, nature, and extent of the injury.17 Only one previously published study has compared hop test performance among individuals with isolated ACL tears vs. those with ACL tears and concomitant meniscal tears. This previous study by VanZile et al.18 found no difference in single- or triple-hop test symmetry among patients who had undergone ACL reconstruction without an associated meniscal surgery, patients who had undergone ACL reconstruction with a meniscus repair, and patients who had undergone ACL reconstruction with a partial meniscectomy. However, the study by VanZile et al. was limited by a small sample size, with only 34 total subjects; 19 with isolated ACL tears and 15 with ACL tears and concomitant meniscus tears (6 who had undergone partial meniscectomy and 9 who had undergone meniscal repair). A larger sample size would increase statistical power, allowing for detection of more subtle differences in hop performance among the different subgroups who underwent ACL reconstruction.
The purpose of this study was to compare hop test inter-limb symmetry for patients who had undergone ACL reconstruction without an associated meniscal surgery, patients who had undergone ACL reconstruction with a meniscus repair, and patients who had undergone ACL reconstruction with a partial meniscectomy. The results of this study may provide valuable insights for clinicians working with patients after ACL reconstruction, as it could help to inform their expectations for recovery of lower body power and knee function.
MATERIALS AND METHODS
Subjects
Hop test results and patient demographic information were extracted from 192 electronic medical records for patients who rehabilitated at two physical therapy clinics associated with Optimum Performance Therapy (Fort Wayne, IN, USA). Of these patients, 102 (53.1%) had undergone an isolated ACL reconstruction (ACLR group), 60 (31.3%) had undergone an ACL reconstruction along with a meniscus repair (ACLR+mnrepair group), and 30 (15.6%) had undergone an ACL reconstruction along with a partial meniscectomy (ACLR+mnectomy group). An a priori sample size estimate indicated that a minimum of 159 subjects were needed in order to be adequately powered to detect a medium-sized between-group difference (inputs: f = 0.25; alpha level = 0.05; power = 0.80; number of groups = 3). G*Power software was used for sample size estimation (G*Power 3.1.9.7).19 In order to be included in this study, a patient needed to have undergone a primary, unilateral ACL reconstruction (regardless of graft type) and completed rehabilitation and return-to-sport testing at one of the physical therapy clinics participating in this study. Records were excluded for patients with a history of contralateral ACL injury or for those who experienced a concomitant injury involving a structure other than the meniscus, such as a collateral ligament. This project was reviewed and approved by the Institutional Review Board at Lutheran Hospital. The data used for this study was obtained through retrospective chart review; therefore, patient consent was not required. No information that could be used to identify specific patients was extracted (e.g. names, social security numbers) in order to maintain patient confidentiality.
Rehabilitation protocol
The patients who participated in this study received rehabilitation from one of eight physical therapists, who all followed a similar post-operative rehabilitation protocol, which progressed through four phases. Phase 1 focused on controlling knee swelling/edema, maintaining patellar mobility, regaining knee motion, facilitating quadriceps activation, and initiating/progressing weight-bearing. Phase 2 focused on restoring full knee range of motion, improving quadriceps and hamstring strength, minimizing gait deviations, promoting knee control during functional activities, general lower body strengthening, and aerobic conditioning. Phase 3 focused on more advanced strengthening and initiating/progressing general skills such as running, landing, jumping, and cutting. Phase 4 focused on more advanced strengthening and training for sport-/activity-specific skills. While rehabilitation followed this general protocol, patients progressed through the stages at different times, depending on their rate of recovery, surgical factors, etc. An initial return-to-sport testing session was conducted once patients exhibited full knee motion, minimal pain/effusion, symmetrical knee extension strength (within 90% of the uninvolved limb based on strength testing with a handheld dynamometer), and no major movement faults (e.g. excessive knee valgus) during dynamic activities such as landing and jumping.
Hop testing
The hop test data used for this study were recorded at the time of the patient’s return-to-sport testing session. On average, return-to-sport testing was completed 6.4 ± 1.4 months after surgery (5-12 month range), which is consistent with the typical return-to-sport testing timeline after ACL reconstruction.20 Patients completed the single-hop test and triple-hop test during return-to-sport testing. The single- and triple-hop tests are both commonly used to assess lower body power and knee-related function after ACL reconstruction.8 Previous studies indicate that these tests exhibit excellent test-retest reliability,21,22 are sensitive to changes in knee-related function throughout rehabilitation,21 and correlate with more direct assessments of lower body muscular power.23
Hop testing was conducted in a manner consistent with previous studies.21,24 For the single-hop test, patients started standing on one limb with their toes behind a marked line. They then hopped forward for maximal distance, landing on the same limb. The triple-hop test was performed in the same manner, except patients completed three consecutive hops with the same limb, instead of a single hop. A tape measure was used to record hop distances. For both tests, the uninvolved limb was tested first, followed by the involved limb. No restriction was placed on arm movements during hop testing. The hop tests were explained and demonstrated to patients and patients completed a practice trial with each limb prior to testing. For each test, two successful trials were completed with each limb, with the average of the two trials recorded for analysis. Successful trials were those where patients were able to maintain their balance on a single limb for at least two seconds after their final landing, reflecting adequate body control. Trials were repeated when patients were unable to maintain control after landing. Patients completed testing in their own shoes and athletic apparel.
Statistical analysis
The physical therapists who conducted the return-to-sport testing calculated a limb symmetry index (LSI) based on the hop distances recorded for the involved and uninvolved limbs using Equation 1.18,21 These LSIs reflected the ratio of the hop distance for the involved limb, relative to the uninvolved limb, expressed as a percentage. An LSI of 100% reflects perfect symmetry, while a value less than 100% reflects a deficit for the involved limb relative to the uninvolved limb.
Equation 1. LSI = 100 * (involved limb hop distance / uninvolved limb hop distance)
For this study, the primary dependent variables of interest were the LSIs for the single-hop test and the triple-hop test. One-way analysis of variance (ANOVA) was used to compare LSIs across the three groups (ACLR, ACLR+mnrepair, ACLR+mnectomy). The factor “graft” (bone-patellar tendon-bone, hamstring, quadriceps tendon) was added to the statistical model to determine if the between-group differences were dependent on graft type. However, there was not a significant group-by-graft interaction effect for either the single-hop test (p = 0.808) or triple-hop test LSIs (p = 0.798). Therefore, the factor graft was removed from the model. One-way ANOVA was also conducted to compare patient age and time since surgery among the three groups. Tukey post hoc tests were conducted in the case of a significant omnibus test. Cohen’s d effect size (ES) statistics were calculated to describe the magnitude of the differences between the groups by dividing the mean difference by the pooled standard deviation.25,26 Effect sizes of 0.2, 0.5, and 0.8 were considered “small”, “moderate”, and “large” differences, respectively.26 The groups differed with respect to their ages. Therefore, age was considered as a potential covariate. However, the correlations between age and the LSI values were weak, with age explaining only 4% of the variance in the single-hop test LSI (r2 = 0.04) and 2% of the variance in the triple-hop test LSI (r2 = 0.02). Consequently, age was not included as a covariate within the statistical model.
As a secondary analysis, the proportion of patients in each group who achieved at least a 90% LSI was examined, since a 90% threshold is often considered adequate (“passing”) when conducting hop testing as part of return-to-sport testing.27,28 Chi-square tests were conducted to compare the proportions of patients who met the 90% LSI threshold across the three groups. An alpha level of 0.05 was used for all tests of statistical significance. jamovi software was used for statistical analysis.29
RESULTS
Table 1 describes the patient characteristics (sex, age, time since surgery, graft type) for the ACLR, ACLR+mnrepair, and ACLR+mnectomy groups. The groups differed with respect to their age (p = 0.010) (Table 1). Post hoc test results indicated that the ACLR+mnectomy group was older than the ACLR+mnrepair group (p = 0.010), while there was no difference in age between the ACLR group and the ACLR+mnectomy group (p = 0.178) or the ACLR group and the ACLR+mnrepair group (p = 0.173). There were no differences among the groups with respect to their time since surgery (p = 0.972) (Table 1).
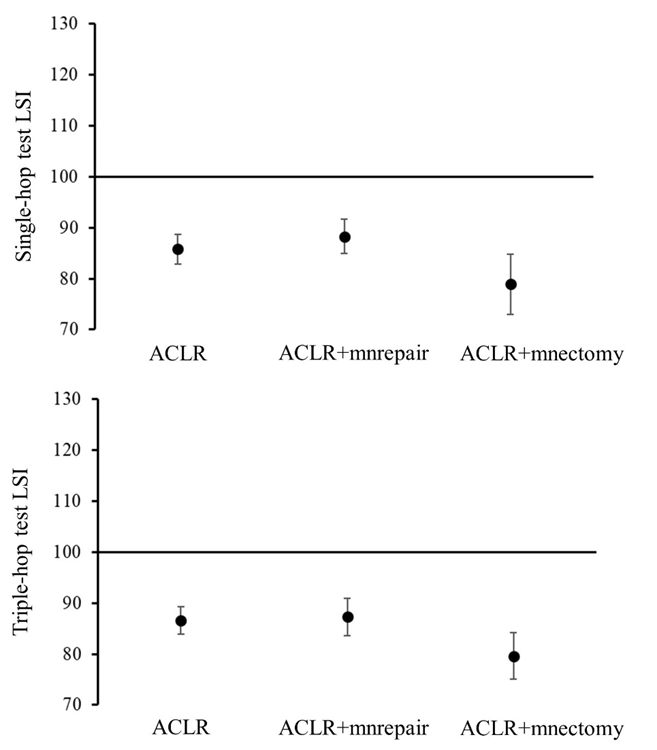
There were significant differences among the groups for the single-hop test LSIs (p = 0.031) and the triple-hop test LSIs (p = 0.024) (Table 2; Figure 1). For the single-hop test, the ACLR+mnectomy group exhibited lower LSIs compared to the ACLR+mnrepair group (p = 0.013; ES = 0.64). The ACLR+mnectomy group also exhibited lower LSIs compared to the ACLR group, with a moderate effect size (ES = 0.47); however, this difference was not statistically significant (p = 0.063). There was no difference in the single-hop test LSIs for the ACLR and ACLR+mnrepair groups (p = 0.553; ES = 0.17). The results were similar for the triple-hop test, as the ACLR+mnectomy group exhibited lower LSIs compared to the ACLR (p = 0.048; ES = 0.49) and ACLR+mnrepair (p = 0.041; ES = 0.55) groups, with no difference between the ACLR and ACLR+mnrepair groups (p = 0.944; ES = 0.05). These results indicate that the ACLR+mnectomy group tended to exhibit greater deficits in hop performance for their involved limb (relative to their uninvolved limb), for both the single-hop test and the triple-hop test, compared to the ACLR and ACLR+mnrepair groups.
_for_the_single-hop_test_(top)_and_triple-hop_test_(bottom)_.png)
For the single-hop test, 53.9% (55 of 102 patients), 56.7% (34 of 60 patients), and 43.3% (13 of 30 patients) of patients achieved the 90% LSI threshold for the ACLR, ACLR+mnrepair, and ACLR+mnectomy groups, respectively (Table 2). This difference in proportions among the groups was not statistically significant based on the results of the Chi-square test (p = 0.476). In contrast, for the triple-hop test, the differences in proportions were statistically significant (p = 0.005), as 56.9% (58 of 102 patients), 61.7% (37 of 60 patients), and 26.7% (8 of 30 patients) of patients achieved the 90% LSI threshold for the ACLR, ACLR+mnrepair, and ACLR+mnectomy groups, respectively (Table 2).
DISCUSSION
The purpose of this study was to compare hop test inter-limb symmetry for patients who had undergone ACL reconstruction without an associated meniscal surgery, patients who had undergone ACL reconstruction with a meniscus repair, and patients who had undergone ACL reconstruction with a partial meniscectomy. In general, the results of this study indicate that patients who underwent ACL reconstruction with a partial meniscectomy exhibited greater hop performance deficits for their involved limb (relative to their uninvolved limb), compared to those who underwent isolated ACL reconstruction and ACL reconstruction with a meniscus repair. This suggests that patients who undergo ACL reconstruction along with a partial meniscectomy tended to experience less complete and/or delayed recovery of involved limb hop performance, which may reflect more persistent deficits in lower body power.
The results of the current study conflict with findings from an earlier study by VanZile et al.18 which found no difference in single- or triple-hop test symmetry among patients who had undergone ACL reconstruction without an associated meniscal surgery, patients who had undergone ACL reconstruction with a meniscus repair, and patients who had undergone ACL reconstruction with a partial meniscectomy. However, the study by VanZile et al. was limited by a relatively small sample size of only 34 total subjects. Therefore, their study may have been underpowered to detect relatively subtle between-group differences in hop performance symmetry. In the current study, the ACLR+mnectomy group exhibited greater inter-limb asymmetry in hop test performance, compared to the ACLR and ACLR+mnrepair groups, with moderate between-group differences (effect sizes ranging from 0.47 to 0.64).
The menisci serve several important functions within the knee joint.30,31 From a biomechanical perspective, the menisci assist with load transmission by dispersing tibiofemoral joint contact forces and attenuating shock during weight-bearing activities, while also providing additional structural stability for the knee joint. The menisci also provide proprioceptive input regarding knee joint position and motion, as they are rich in mechanoreceptors. This proprioceptive information may support neuromuscular control of the knee. There is evidence to suggest that partial meniscectomy may negatively impact these important knee-related functions32,33 and that longer-term patient-reported outcomes tend to be worse among patients who undergo partial meniscectomy vs. meniscal repair along with ACL reconstruction.32,34 The results of the current study appear to provide additional evidence that a patient’s prognosis after ACL reconstruction may be poorer if they have undergone a partial meniscectomy.
Clinically, the data presented in this study seem to suggest that at the time of initial return-to-sport testing, the mean hop test scores did not meet or exceed the typical 90% LSI cut-off suggested in the literature.27,28 In fact, only the ACLR+mnrepair group demonstrated 95% confidence intervals around the mean that contained a 90% LSI score. Thus, at a mean of six months post operative, clinicians might not expect a 90% LSI for hop testing. In fact, the lower bounds of the 95% CIs for the ACLR+mnectomy group were as low as 72.9% and 75.0% for the single- and triple-hop tests, respectively. Since this study represents the largest sample of hop test data for individuals undergoing these surgeries, there is the potential for the values in Table 2 to help guide clinical expectations and goal setting.
Additionally, it appears that a gap exists between LSI values for muscle strength and hop testing, especially in the ACLR+mnectomy group. As the patients in the ACLR+mnectomy group achieved relatively symmetrical knee extension strength (as this was a requirement to be eligible for return-to-sport testing), but still exhibited notable deficits in hop performance. To address these persistent deficits in lower body power, it may be beneficial to factor a higher dosage of muscle power interventions into the plan of care for these patients, especially towards the later stages of rehabilitation. Future research is required to see whether this would help to bridge the gap observed in this study. It may also be worth examining the extent to which other factors, such as kinesiophobia and fear of re-injury contribute to the observed deficits in hop performance, particularly for those who have undergone ACL reconstruction with a partial meniscectomy, as there is evidence to suggest that these types of psychological factors can influence movement performance after ACL reconstruction.35
While the results of the current study may be noteworthy, there are limitations that should be considered. First, the samples included in this study were somewhat heterogenous in terms of their ages and sport/activity backgrounds. Although this is reflective of the types of patients who undergo ACL reconstruction, focusing on more homogenous sub-samples of patients (e.g. adolescent athletes) could have limited some potential confounding variables. In addition, the groups differed with respect to their age, as the patients who underwent partial meniscectomy tended to be older than those who underwent meniscal repair. The authors considered including age as a covariate within the statistical model to account for this difference; however, it was thought to not be appropriate in this case, since the observed age difference likely reflects what occurs in normal clinical practice, where there is a tendency to repair the meniscus with younger patients.36,37 While the differences in age could be considered a confounding variable when comparing outcomes for the different surgeries, statistically eliminating the potential influence of the age difference would produce findings that are not consistent with the reality of clinical practice. Preliminary analyses also indicated that age explained minimal variance in hop test performance (≤4%), which suggests that age has a small impact on hop test symmetry after ACL reconstruction. Another limitation is that hop performance was only assessed once, with the timing of testing varying among patients depending on their rate of recovery. Another option would have been to compare hop test performance at a consistent time point; however, this is not reflective of routine clinical practice, where the timing of return-to-sport testing is individualized for each patient. Also, patient data were extracted from two different physical therapy clinics, which introduces another potential source of variability within the data set. However, preliminary independent t-tests indicated that single-hop test (p = 0.848) and triple-hop test (p = 0.615) LSIs did not differ between patients from the two clinic sites. Finally, the nature, location, and extent of the meniscus injuries were not analyzed as part of this study. Future studies should examine how these factors impact clinical outcomes among patients with ACL tears and concomitant meniscal tears. Although not a limitation per se, it is also important to note that the results of this study do not provide insights into the underlying contributors to hop performance deficits (e.g. strength deficits, motor control adaptations, fear of re-injury).
CONCLUSION
The results of this study suggest that patients who have undergone ACL reconstruction with a partial meniscectomy tend to exhibit greater hop performance deficits for their involved limb (relative to their uninvolved limb), compared to those who have undergone isolated ACL reconstruction or ACL reconstruction with a meniscus repair. Multiple factors may have contributed to the observed differences in hop performance, including persistent deficits in lower body power and age differences among the patient subgroups. Clinicians working with patients after ACL reconstruction should understand how meniscal injury may impact a patient’s recovery.
Conflicts of interest
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
The authors would like to thank Gordon Bokhart and the staff at Lutheran Hospital for supporting this project.