


INTRODUCTION
Some individuals have exercise-induced lower leg pain (ELP) that is occasionally caused by a chronic exertional compartment syndrome (CECS).1 The pathophysiology of CECS is likely associated with an abnormal muscle pressure build-up. Most often, CECS occurs in the anterior tibial compartment (ant-CECS). Symptoms are anterior lower leg pain and tightness occurring during and after exertion.2 If three to six months of conservative measures including gait retraining are to no avail, a diagnostic intracompartmental pressure measurement (ICPM) is advised.3 However, this invasive technique is not patient friendly, and the execution is operator dependent with low diagnostic specificity.4,5
A range of non-invasive tools are currently being tested for diagnosis of ant-CECS.6,7 An ultrasound (US) technique combined with tissue pressure analysis has been used to diagnose acute compartment syndrome (ACS).8–10 However, methodologies of US studies for detection of CECS are not standardized and reports lack detail on external force applied.11–13 Standardization of methodology is crucial for interpreting compartment cross sectional diameter (thickness) or compressibility.14,15
Recent researchers have investigated tibialis anterior (TA) compartment compressibility with a pressure manometer fixed to the US probe demonstrating the importance of standardizing externally applied pressure.14–16 It was concluded that this method is reliable with very high intra- and inter-observer correlations. These findings suggest that US with tissue pressure analysis may play a diagnostic role in suspected CECS. The purpose of the present study was to investigate the reliability of a novel US compressibility technique using two distinct internal landmarks on the lower leg in a diverse group of asymptomatic adults.
METHODS
General Study Information
The study was performed at Máxima Medical Center, Veldhoven between February and June 2023. The departments of sports medicine and surgery are having a long-time collaborative interest in the management of patients with ELP. Yearly approximately 300 patients with suspected CECS undergo analysis including ICPM and treatment at this institution. Procedures of the study complied with the Declaration of Helsinki (1964) and its amendments. The study protocol was approved by MMC’s medical ethical testing committee (NL82601.015.22). In addition, safety of the tool has been confirmed in recent studies.8,9,14–16
Participants
Study participants were locally recruited among relatives and colleagues via public talks and advertisements. They were eligible if >18 years of age without a history of muscle disorders or arteriovenous diseases. The absence of previous lower leg traumas or ELP related complaints (pain, tightness, cramps etc.) were confirmed by completion of a modified Netwerk Inspannings Afhankelijke PijnSyndromen (NIAPS) questionnaire. This questionnaire has been standardly used in a number of Dutch hospitals at the intake of ELP patients since 2013.17 Potential participants were excluded if they judged that they were not able to complete two five-minute walks at 5.5km/hour with a 15% slope (n=1).
Observer training
Three observers participated in this study. They had no earlier professional experience with US imaging techniques. Prior to study initiation, they were informed on specifics of the device and the measurement protocol by the manufacturing company, including subject positioning. Their protocol indicates that measurements should be performed while individuals are positioned on the side with full medial leg support with the transition zone interosseous membrane to tibial bone (TZIT) as the internal landmark. Additionally, three one-hour sessions were used for training in the handling and positioning of the study device, operating of the equipment and interpretation of the data in accordance to the study protocol. Goals of attaining a SD <0.5 for d10 and d80, and a SD <1.5 for compressibility after four measurements were achieved.
Muscle Compressibility Device
The study device (CPMX1, Compremium AG, Switzerland) has previously been described in detail.15 In short, the tool consists of an US probe with an integrated pressure sensor connected to a tablet. The probe is manually placed on an external landmark of the lower leg and is directed towards an internal landmark. As the device is time-synchronized, images are automatically obtained at 10mmHg and 80mmHg external US probe pressure. After manually marking the superficial and deep muscle landmark on the screen, the integrated software displays compartment thickness at both pressures (d10, d80; millimeters) and calculates muscle compressibility using a formula (d10 – d80) / d10 * 100%). A single measurement takes approximately 20-30 seconds.
Protocol of Compressibility Measurements
The study participants were dressed in shorts wearing sport or comfortable shoes and rested for five minutes on an examination bench in supine position in a dedicated examination room with a stable 20-degree centigrade temperature prior to a measurement. Both legs were supported at the knee with a triangular pillow and supported on the ankle joints as recently suggested by van Heeswijk et al. (Figure 1).15 The distance between fibular head at the knee and lateral malleolus at the ankle was measured. At 2/5th of this distance, some 2 centimeters lateral to the anterior tibial crest, the US probe position was provisionally marked with a skin marker. Both earlier and recent studies suggested that, apart from the TZIT, the interosseous membrane (IM) may also serve well as internal landmark.10,12,13,15 At this provisional mark, the probe was oriented perpendicularly towards the internal landmarks (Figure 2). When these were clearly visible, they received their respective definitive skin mark that was used by all three observers. The first observer (OB1) completed the measurement protocol, followed by the second (OB2) and third observer (OB3). Order of observers, leg of measurement (left or right), and internal landmark (IM or TZIT) were randomized.


Intra-observer and inter-observer reliability were obtained by having the observers execute a compressibility measurement four times in each configuration (right leg-IM, right leg-TZIT, left leg-IM, left leg-TZIT) without excluding potential false or wrong measurements. By doing so, a total of 4x4=16 compressibility measurements per observer per study participant were performed. Observers were blinded for each other’s measurements.
Outcomes
The primary outcome variable was inter-observer reliability expressed as intraclass correlation (ICC) regarding values of compartment thickness at two different pressures (10 and 80 mmHg) and compressibility. A secondary outcome variable was intra-observer reliability regarding these values, expressed as ICC as well. Additional possible confounding variables of interest were age (<30 years, 30-49 years, ≥50 years), gender, and BMI (<25kg/m2, ≥25kg/m2).
Sample Size Calculation
The sample size was determined using G*Power 3.1.18 Calculations were based on published data.14,15,19 A one sided 95% target confidence interval width of 0.05 aiming for an ICC≥0.75 based on three observers resulted in a sample size of n=140. As two different internal landmarks per leg per participant were observed, 35 participants were required.
Statistical Analysis
Data were analyzed using SPSS IBM 22. Data variables were checked for normality using kurtosis, skewness and histograms. If normal, they were depicted as mean (± standard deviation; SD). If the distribution was non-normal, data were depicted as median (interquartile range; IQR).
First, mean (or median) compartment thickness at 10 mmHg (d10), compartment thickness at 80 mmHg (d80) and compressibility were averaged across participants and observers. It was tested whether these variables differed between the two landmarks (TZIT and IM), or between left and right leg measurements using student t-tests for normal distributed data and Mann-Whitney U for non-normal distributed data. The literature suggested the possible presence of differences between the internal landmarks or side of measurement.14,15 Similarly, these variables were compared between groups based on age, gender or BMI category.
Second, inter-observer reliability based on d10, d80 and compressibility was presented as ICC with 95%-confidence interval. The data were based on the averages of the four repeat measurements per observer. An absolute agreement with two-way random single observer model was used. In addition, ICCs were presented separately for the two landmarks (TZIT and IM) or for the left and right leg measurements. Data were considered significant for an α<0.05. An ICC <0.5 was considered as poor, 0.5-0.7 as moderate, 0.7-0.9 as good and >0.9 as excellent according to Koo et al.20
Intra-observer reliability of d10, d80 and compressibility were presented for each observer separately as ICCs with 95%-CI. Again, ICCs were based on the averages of the four repetitions and as an absolute agreement with a two-way random single measure model. In addition, ICCs were presented separately for the two landmarks (TZIT and IM) or for the left and right leg measurements.
To investigate the influence of number of measurements on the primary outcome (inter-observer reliability), ICCs were calculated based on one, two, three and four repetitions per measurement site. Absolute agreement was calculated using a two-way random average measure model for the two landmarks (TZIT and IM) separately.
RESULTS
All 35 study participants provided verbal and written consent and completed the measurements without reporting any discomfort. The study population consisted of 21 females and 14 males with a median age of 40 years (range, 19-72 years) and an average BMI of 24.1 kg/m2 (range, 18.3-31.6 kg/m2). Two of a total of 1680 measurements resulted in a negative compressibility value and were excluded as per protocol.
Overall, anterior lower leg compartments were thicker and less compressible using the IM landmark compared to the TZIT landmark. No differences in thickness and compressibility were observed regarding left and right leg. As was expected, male compartments were thicker than female compartments. Interestingly, age did not influence thickness. Details of thickness of the TA using the two different internal landmarks for males and females, age groups, and BMI groups are listed in Table 1.
Inter-Observer Reliability
The overall ICC of d10 and d80 measurements combined for left leg, right leg, IM and TZIT based on the average of four repetitions was considered good, but poor for compressibility.
Figure 3 depicts ICC subdivided regarding internal landmark and leg side. The ICCTZIT for d10 was 0.65 (0.47 - 0.77), for d80 was 0.53 (0.29 - 0.70), and for compressibility was 0.20 (0.05 - 0.37). Conversely, the ICCIM was always higher (d10 0.85 (0.78 - 0.90), d80 0.82 (0.73 - 0.88), as was compressibility 0.51 (0.37 - 0.64)). These data indicate that measurements using the IM internal landmark were more reliable than the TZIT as internal landmark.
Repeatability was different between the two legs. For instance, the ICCleft for d10 was 0.78 (0.67 - 0.86), for d80 was 0.70 (0.54 - 0.81), and for compressibility was 0.24 (0.10 - 0.40). The ICCright was 0.76 (0.65 - 0.85) for d10 and 0.70 (0.53 - 0.81) for d80 but higher for compressibility 0.43 (0.25 - 0.58). These data indicate that compressibility measurements on the right leg were more reliable.
_expressed_as_intraclass_correlation_(two-way_random__abso.jpeg)
Intra-Observer Reliability
The ICC for compartment thickness measurements using either 10 or 80 mmHg external probe pressure (d10, d80) were excellent for all three observers if TZIT, IM, left and right leg measurements were combined.
Focusing on the individual observers (OB1, OB2 and OB3), ICCOB1 for d10 was 0.97 (0.96 - 0.98), 0.96 (0.95 - 0.97) for ICCOB2, and 0.91 (0.89 - 0.93) for ICCOB3. For d80 the ICCOB1 was 0.97 (0.96 - 0.97), ICCOB2 was 0.95 (0.93 - 0.96), and ICCOB3 was 0.90 (0.87 - 0.92). If outcome was subdivided for TZIT, IM, left and right leg, ICC remained excellent for two of the three observers. However, OB3 scored some ICCs as ‘good’ instead of excellent.
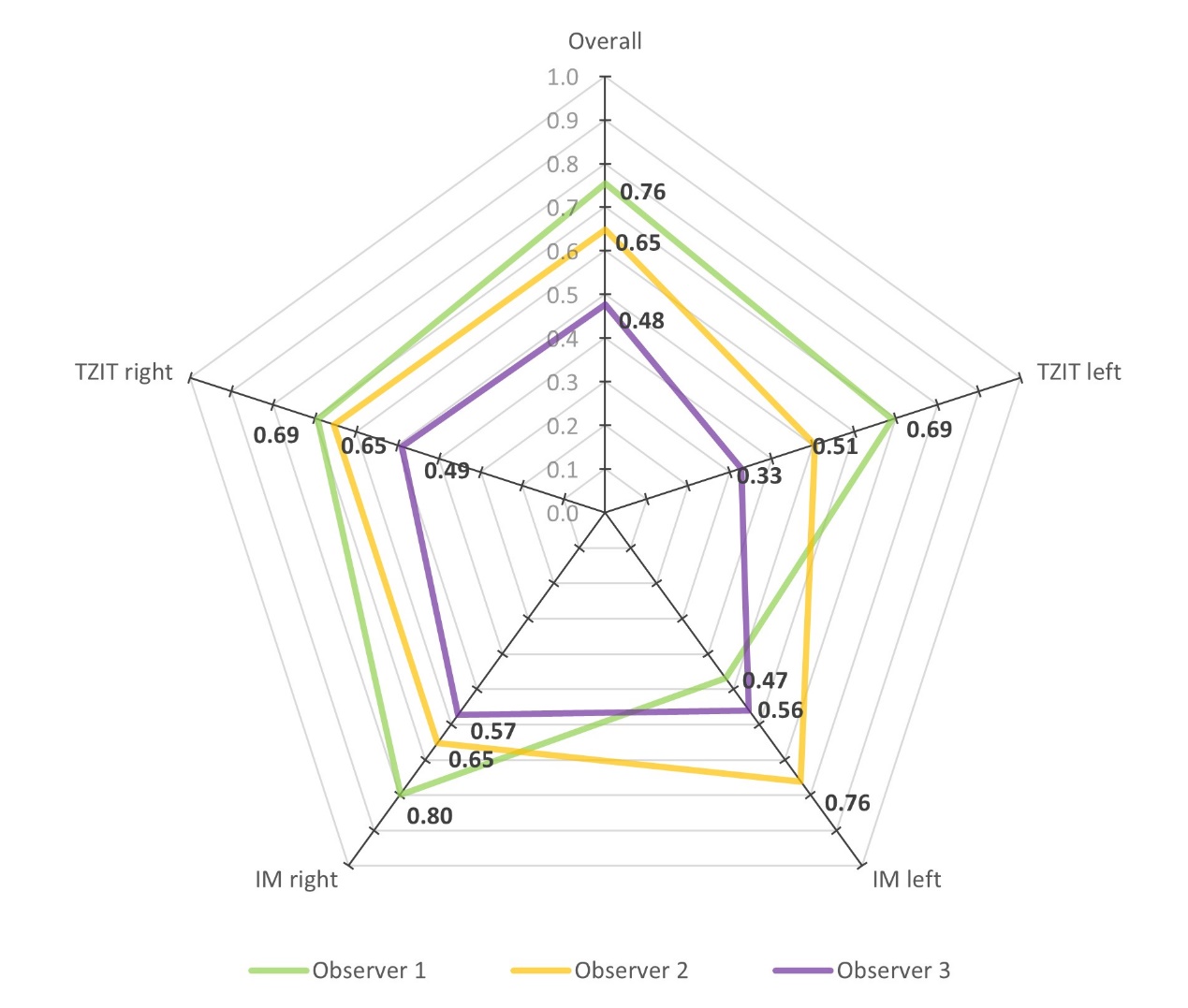
ICCs for compressibility differed among the three observers. Combined for both the TZIT, IM, left and right leg. ICCOB1 was 0.76 (0.70 - 0.81), ICCOB2 0.65 (0.58 - 0.72), and ICCOB3 0.48 (0.39 - 0.56). Figure 4 depicts ICCs for three observers in relation to internal landmarks and leg side.

Repeatability
Considering all measurements combined, the inter-observer ICC for d10 and d80 for the first measurement were 0.90 (0.85 - 0.93) and 0.87 (0.78 - 0.92), respectively. Performing additional measurements did not further improve their ICCs.
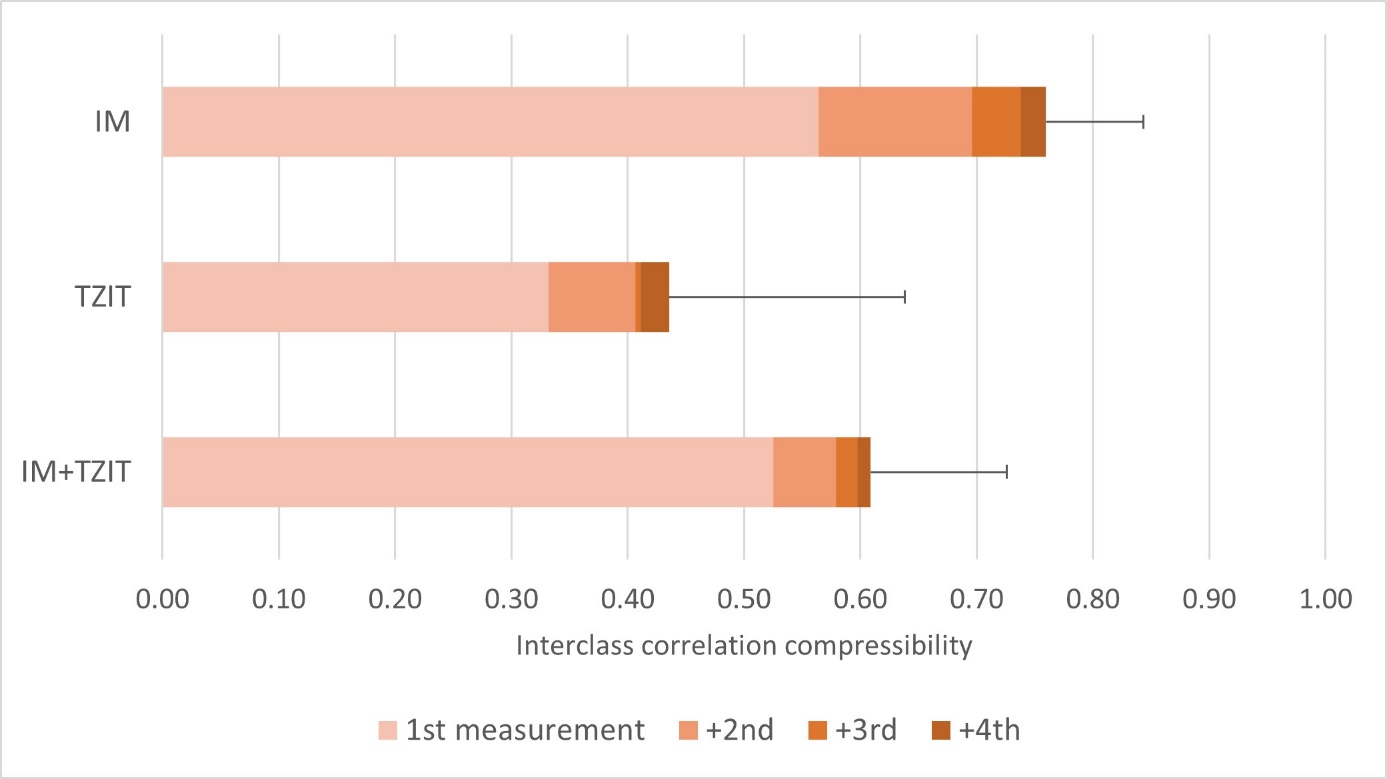
The ICC for both landmarks combined were for one, two, three and four repetitive compressibility measurements 0.53 (0.36 - 0.65), 0.58 (0.42 - 0.70), 0.60 (0.43 - 0.71), and 0.61 (0.44 - 0.73), respectively (Figure 5, lower panel). However, the IM landmark repeatability was higher compared to the TZIT (Figure 5, upper and middle panel). Generally, a stable ICC was achieved after two repetitive measurements.

DISCUSSION
The diagnosis chronic exertional compartment syndrome (CECS) causing exercise-induced leg pain (ELP) is in part based on a suggestive history and physical examination. The current gold standard is provided by an intracompartmental pressure measurement (ICPM), but this tool is associated with several disadvantages. Besides its invasive character, results may be suboptimal as it lacks a potential to predict fasciotomy outcome. Recently, researchers have suggested that ultrasound (US) based techniques may possibly be used to diagnose suspected CECS of the TA.2,6,7,19 The aim of the present study was to investigate the reliability of a new US compressibility technique using two distinct lower leg internal landmarks in a heterogenous group of asymptomatic individuals. Findings of the present study demonstrate moderate to good reliability for the proposed technique. In addition, measurements at proximal portions of the TA using the interosseous membrane (IM) as internal landmark are more reliable compared to the transition zone IM to tibial bone (TZIT).
A small number of studies have reported on the validity of US in possible compartment syndromes.6,11,13,21 Birtles et al. found differences in TA cross-sectional area in CECS patients compared to healthy controls.21 Wasserman and Oschman claimed that a preoperative change of compartment thickness during exercise in CECS was associated with a successful treatment outcome.11 However, muscle compartment thickness is often assessed using a random and not literature supported US probe position. Moreover, the force applied by the US probe is frequently not monitored. The present study demonstrates that compressibility values and compartment thickness vary depending on the internal landmarks. This finding highlights the importance of standardizing probe placement and the pressure applied during measurements to ensure reliable results.
Recent studies focused on optimizing methodology of US techniques by varying externally exerted US probe pressure. The technique was recently found to accurately detect acute compartment syndromes.8,16,22 A study in ten human volunteers measured TA compartment compressibility at two different US probe induced external pressures.14 It was concluded that the method had potential with high intra- and inter-observer correlations. Sellei et al. found a 0.93 ICC between TA compressibility using an US technique and ICPM in six trauma patients with possible ACS.8 Another feasibility study testing a next generation US probe with an integrated pressure sensor found that compressibility measurements at the lower leg with knee and heel support using the IM as an internal landmark yielded the lowest variability (ICC 0.98).15 These studies indicate that US imaging with an integrated tissue pressure analysis mode can determine TA compartment compressibility and may possibly play a diagnostic role in ant-CECS. However, these results required confirmation in larger group of humans of different ages, BMI and sex. The present study in 35 resting healthy individuals demonstrates that the internal landmark IM yields more reliable test results compared to the TZIT.
The current study also tested the potential influence of ultrasonographist position relative to the study subject. As a rule, an observer sits at the right side of the patient during examination. However, this preferential position may possibly introduce bias such as different angles towards internal landmark and altered pressure distribution of left and right leg measurements. For instance, Anwander et al. found a significant 1.8% compressibility difference between the right and left leg, possibly explained by position of the observer or anatomical difference.14 In that study, the observer was seated at the right side of the participant at all times. In the present study, the dominant hand of observers (all three right-handed) was used for both legs. As a consequence, the observer faced the participant during a right leg measurement but was oriented towards the participant’s feet during a left leg measurement (Figure 1). Significant compressibility left-right differences using either landmark were not observed as expected as healthy person’s legs are identical. However, the intraclass correlation of left leg measurements were overall lower compared to the right side suggesting that US measurements for bilateral CECS should be executed with the observer facing the patient.
Interclass correlations in the current study are lower compared to previous studies.8,14,15 One of the contributing factors could be the lack of observer experience. The study aimed to test the technique in a real-world situation reflecting the performance of average young doctors instead of highly experienced ultrasonograpers. The combination of limited US experience, a different observer positioning depending on measurement of left and right leg, and the spread of measurements over consecutive months may have contributed to this moderate ICC. In addition, earlier data were obtained from populations who were small or having extreme values leading to relatively high ICC values.8,14,15 It is expected that compressibility in CECS patients will deviate from healthy volunteers leading to higher values of ICC.
A possible study limitation is a minimal number of internal landmarks. However, it should be appreciated that earlier studies focused on just the TZIT. As previous literature showed that the IM was also an option, it was decided to compare these two.13,15 During this study, the observers experienced that the TZIT was more difficult to identify compared to the IM, likely influenced by lack of ultrasound experience. An additional limitation is generalizability. The volunteers had no ELP and were in a resting state. The present study should thus be regarded as generating normal lower leg muscle compressibility values associated with sex, BMI, and age in normals. TAs thicknesses was not related to age. This may be due to the active lifestyle of our healthy volunteers. Depending on type of internal landmark, compressibility differed among age groups. Small sample sizes and varying subcutis thickness are potential causes. The latter has not been analyzed in this study. Future studies in larger populations following exertion and in patients possibly having CECS should include subcutis thickness measurements.
CONCLUSION
This study reports on specifics of a novel US technique for non-invasively determining lower leg anterior tibial muscle compressibility. The use of the interosseous membrane as internal reference point resulted in most optimal reliability test results. Additionally, observer positioning is of importance as reliability improved when an operator was oriented towards the participant. Future studies should aim to test muscle compressibility after exercise and in CECS patients.
CONFLICT OF INTEREST
The study devices were provided by the manufacturer free of charge. Apart from instructions on use and maintenance of the study devices, the manufacturer was not involved in any way in the conduct, analysis, or reporting of the results of this study.
ACKNOWLEDGEMENTS
The support of Stichting Stimuleren Sportgeneeskunde Zuidoost-Brabant is greatly acknowledged. The study devices (CPMX1) were provided by Compremium AG, Switzerland.