
Introduction
The use of objective functional measures in the return-to-sport (RTS) decision making process is a big step forward in the rehabilitation of individuals who have sustained anterior cruciate ligament (ACL) injuries and subsequent ACL reconstruction (ACLR).1–3 However, in the population of athletes with ACLR, 65% returns to their pre-injury sports level4 and there remains a 20% chance of sustaining a secondary ACL injury.5 These observations justify the continued search for more solid RTS criteria to capture remaining deficits and alterations associated with re-injury that are currently not identified.1,2,6,7 One commonly used RTS assessment is hamstrings and quadriceps strength and the hamstrings-to-quadriceps strength ratio (H/Q ratio).6,8,9 The H/Q ratio is suggested to represent the muscular capacity to actively stabilize the knee joint since the hamstrings work as an agonist of the ACL and might reduce the anterior pull of the quadriceps on the tibia.10–14 Remaining strength asymmetries6,15 and a reduced H/Q ratio6 at RTS have been associated with increased risk for sustaining re-injuries. However, up to 46% of the ACLR patients still return to sport with remaining hamstrings and quadriceps strength asymmetries.9,16 It remains questionable whether these strength asymmetries resolve in the months following RTS without further rehabilitation.9,17 For example, a systematic review by Tayfur et al.18 concluded that there was strong evidence for remaining quadriceps and hamstrings concentric strength deficits in ACLR athletes 24 months after surgery compared to uninjured controls.
Hamstrings and quadriceps muscle strength is frequently evaluated by an isokinetic dynamometer. This assessment provides moment-angle data over a pre-defined range of motion (ROM) from which peak values (e.g. peak moment and angle of peak moment) are typically extracted. Subsequent analyses such as the limb symmetry index and H/Q ratio are consequentially calculated based on these peak values. The reduction of the moment-angle data to peak values however, leads to the loss of potentially relevant clinical information. First, normal peak values could mask strength deficits or asymmetries in other knee flexion angles than the angle of peak moment. For example, Baumgart et al.19 showed that ACLR patients at an average of 6.6 months after surgery have larger between-leg hamstrings strength differences at larger knee flexion angles compared to more extended knee positions. Second, calculating the H/Q ratio by dividing the peak hamstrings moment by the peak quadriceps moment seems physiologically irrelevant as the quadriceps peak moment is achieved at a more flexed knee angle than the hamstrings peak moment, leaving them functionally unrelated.11 Angle-specific H/Q ratios, which are ratios between hamstrings and quadriceps moments reached at identical knee flexion angles, would appear to be more relevant to assess muscle imbalance throughout the entire ROM.11,14,20 Angle-specific analysis of the H/Q ratio and subsequent analysis of the hamstrings and quadriceps moment-angle profile is increasingly used in both uninjured athletes11,20–22 and athletes with ACLR.17,23 Considering that the moment arm of the hamstring muscles becomes suboptimal when the knee joint angle is not in mid-range (particularly in deeper knee flexion), and this in comparison to a relatively constant moment arm of the quadriceps muscles, calculating the H/Q ratio based on peak moments alone could conceal incomplete hamstring muscle strength recovery.24 However, the evolution of angle-specific strength analyses after RTS has not yet been investigated. In conclusion, a longitudinal observational study on angle-specific strength analyses is necessary to fully understand muscle adaptations in athletes with ACLR at RTS and later on. Such information is necessary to improve rehabilitation strategies and RTS decision criteria.
Therefore, the first objective of this study was to investigate moment-angle profiles and angle-specific H/Q ratio profiles in athletes with ACLR at the time of RTS. In order to evaluate the potential added value of angle-specific analyses over peak-based measures, hamstrings and quadriceps peak moments, and peak-based H/Q ratios were analyzed. The hypothesis was that angle-specific analyses will reveal more strength shortcomings compared to peak-based evaluations. The second objective of this study was to assess whether strength asymmetries identified at the time of RTS, persist after six months. It was hypothesized that part of the strength shortcomings persist despite RTS.
Materials and methods
Study design and participants
In this prospective observational study, 20 athletes who underwent ACLR (ipsilateral semitendinosus autograft) were recruited. They all completed rehabilitation with their own physiotherapist and had been cleared by the surgeon to restart training, based on subjective assessment (there were no strict criteria imposed by the study). If ACLR surgery concerned a re-injury, the athlete was excluded from this study. All participants practiced sport at competitive level (from lowest division to National division) before their injury and wished to return to sport. Isokinetic muscle strength tests were performed three times in the ACLR group: at the time of RTS (262 ± 60 days post-surgery and maximum two weeks between the test session and the first full training session), three months post RTS (96 ± 19 days after RTS) and 6 months post RTS (201 ± 20 days after RTS). At the three month post RTS test, four athletes with ACLR dropped out (one hamstrings injury, three lost interest in participation). Two additional athletes with ACLR dropped out at six months post RTS (one ACL re-injury, one lost interest in participation).
Twenty control athletes with no history of an ACL injury and no lower limb injury in the six months before the test session, were also recruited. These control athletes were tested only once. In both groups only competitive athletes who complete at least one training and one match per week (before the ACL injury) were included. The ACLR group and control group were matched for sex and sports type. Two mismatches in sports type could not be avoided. For the identification of strength deficits and asymmetries at the moment of RTS, the data of all 20 athletes with ACLR and control athletes were included. For the follow-up of the strength asymmetries, only the data of the 16 ACLR athletes who were tested at RTS and at three months were included. The data of the two patients (one male and one female) who dropped out between three and six months after RTS were estimated through a data imputation technique (see statistics). All participants provided written informed consent prior to inclusion in the data collection procedure. The study was approved by the local ethical committee(Ethics Committee Research UZ/KU Leuven) and executed in accordance with the Declaration of Helsinki.
Isokinetic testing
All athletes performed isokinetic muscle strength tests on a Biodex System 4 Pro (Biodex Medical Systems, Shirley, NY, USA). A five-minute general warm-up on a cycle ergometer was implemented prior to testing. For the isokinetic testing, the athletes were seated with a hip flexion angle of 95-100°. Straps were applied across the chest, pelvis and distal thigh. The rotational axis of the knee joint and the isokinetic dynamometer crank arm were aligned. The distal attachment pad of the crank arm was firmly attached to the distal part of the shank, two fingers proximal to the medial malleolus. This position was standardised over the different sessions in the ACLR athletes. Every athlete performed a continuous series of five maximal effort trials for concentric knee extensions and flexions at 60°/s with each leg. A practice series was allowed before each test series. Between series, a resting period of 60 seconds was provided.
Data processing
Moment-angle profiles for hamstrings and quadriceps were calculated using the open source Matlab package IKD1D (version 0.02, http://ikd1d.org/). This program standardizes the generation of a representative moment-angle profile from several trials (Appendix A). After joint-angle based gravitational correction of the raw moment values, the selection of valid trials was standardized between participants through an automatic selection procedure. This selection procedure is based on three criteria: the acceptable variation from the target angular velocity, the minimally achieved ROM at the target angular velocity and the between trial variation in peak moment. The target angular velocity was set at 60°/s, the minimal ROM was set at 80° and the acceptable variation between trials in terms of angular velocity, ROM and peak moment were all set at 10%. To avoid the automatic selection picking one outlier, a minimum of three trials for flexion and three trials for extension were included per participant. If less than three trials were automatically selected, moment tolerance was augmented until the minimal number of three trials was included. Next, moment-angle profiles for each participant were averaged over the entire ROM using a moving average with 10 degrees window. These average moment-angle profiles were used to calculate the angle-specific H/Q ratio profile. The average hamstrings and quadriceps moment-angle profiles were also used to determine the hamstrings and quadriceps peak moment values, from which the peak-based H/Q ratios were calculated.
Statistical analysis
In earlier studies20,22,25,26 angle-specific moment values and angle-specific H/Q ratios were extracted at a limited number of joint angles, omitting the fact that the ratio profile is a continual measure. Through the introduction of statistical parametric mapping (SPM) in biomechanical research,27 hypotheses on moment-angle profiles and angle-specific H/Q ratio profiles can be tested without neglecting the interdependence between measures across different joint angles. One-dimensional SPM analyses were performed using the open source package SPM1D (version M.0.4.5, http://www.spm1d.org/).28 For the hamstrings and quadriceps peak moments and the peak-based H/Q ratios, zero-dimensional analyses were performed using IBM SPSS Statistics (version 25, SPSS Inc., Chicago IL, United States https://www.ibm.com/analytics/spss-statistics-software).
Three statistical analyses were performed. First, to identify general strength deficits in the ACLR group at the time of RTS, the injured legs of the 20 athletes with ACLR were compared to the data of the 20 control athletes. For those athletes with ACLR who had their dominant leg injured (n=7), the dominant leg was also selected in their matched control athlete, and vice versa for non-dominant leg. Zero- and one-dimensional independent groups t-tests were used for the statistical analysis of these strength deficits. Second, the data of the injured and uninjured leg of all 20 athletes with ACLR at the time of RTS, were compared to assess strength asymmetries. For the statistical analysis of strength asymmetries, zero- and one-dimensional paired t-tests were used. Finally, to assess strength asymmetries over time, two-way repeated measures ANOVAs (leg time) were used. The data of the injured and uninjured leg of the 16 athletes with ACLR that were tested at the time of RTS and at three months post RTS, were implemented in this analysis. The data of the two participants that dropped out at six months follow-up, were estimated through data imputation (based on adding the average difference between three and six months to their value at three months post RTS). Alpha was set at 0.05 for all statistical analyses. Considering the explorative nature of the study, no correction for multiple testing (Bonferroni) was applied to avoid overly conservative statistical interpretations.
The data of both sexes was pooled, although differences in absolute strength might be expected between women and men. This was justified because the group of athletes with ACLR and control athletes were matched for sex and thus had the same proportion of men/women. Also, the longitudinal analysis is not affected by the pooling of both sexes since the same group of athletes is followed over time and the proportion of men and women is thus not different between conditions. Furthermore, the authors did not expect differences in strength improvements between sexes, based on the meta-analysis of Roberts et al.29
Results
A detailed description of the included participants is provided in Table 1.
Strength deficits at time of RTS
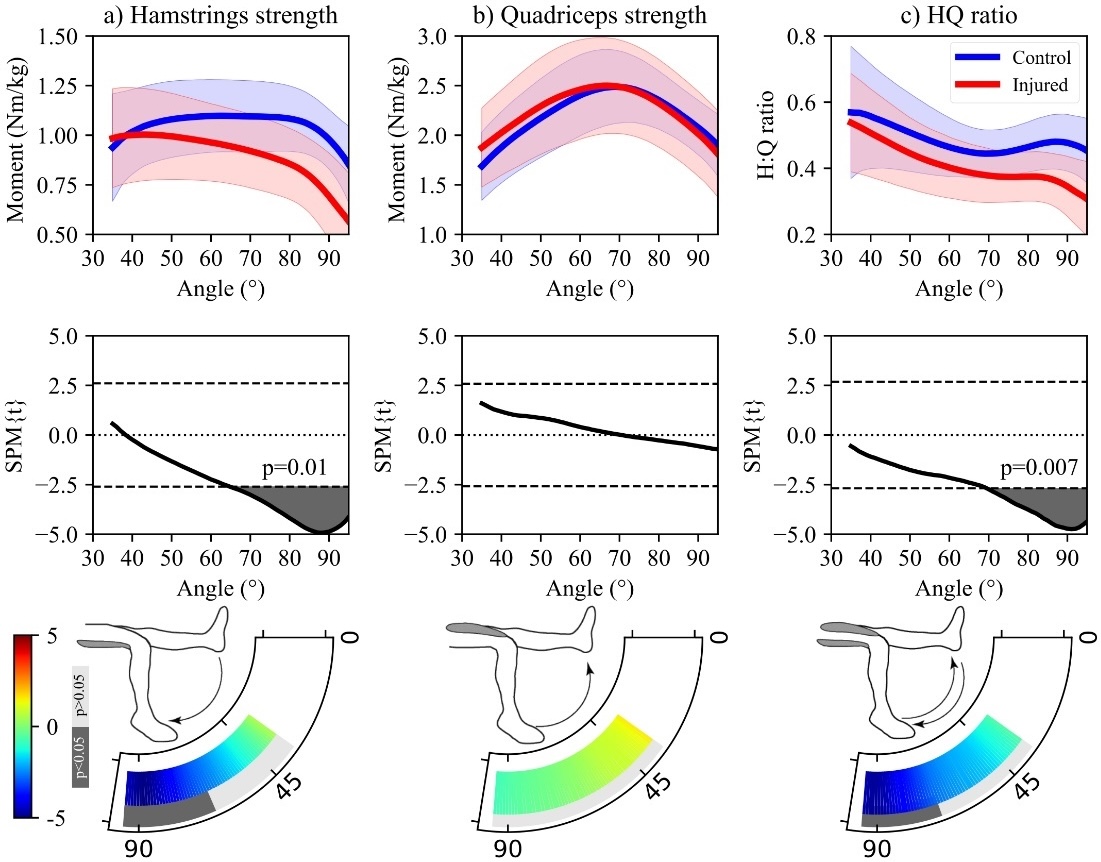
The hamstrings moment-angle profile of the ACLR group was significantly lower between 65° and 95° of knee flexion (p=0.01) compared to the controls (Figure 1). The quadriceps moment-angle profile was not significantly different between groups across the entire ROM. The angle-specific H/Q ratio profile was significantly lower in the ACLR group compared to healthy control subjects between 70° and 95° of knee flexion (p<0.01). The peak hamstrings and quadriceps moment and peak-based H/Q ratio were not significantly different between the ACLR and control group (Table 2).
_hamstrings_and_(b)_quadriceps_moment-angle.jpeg)
Strength asymmetries at time of RTS
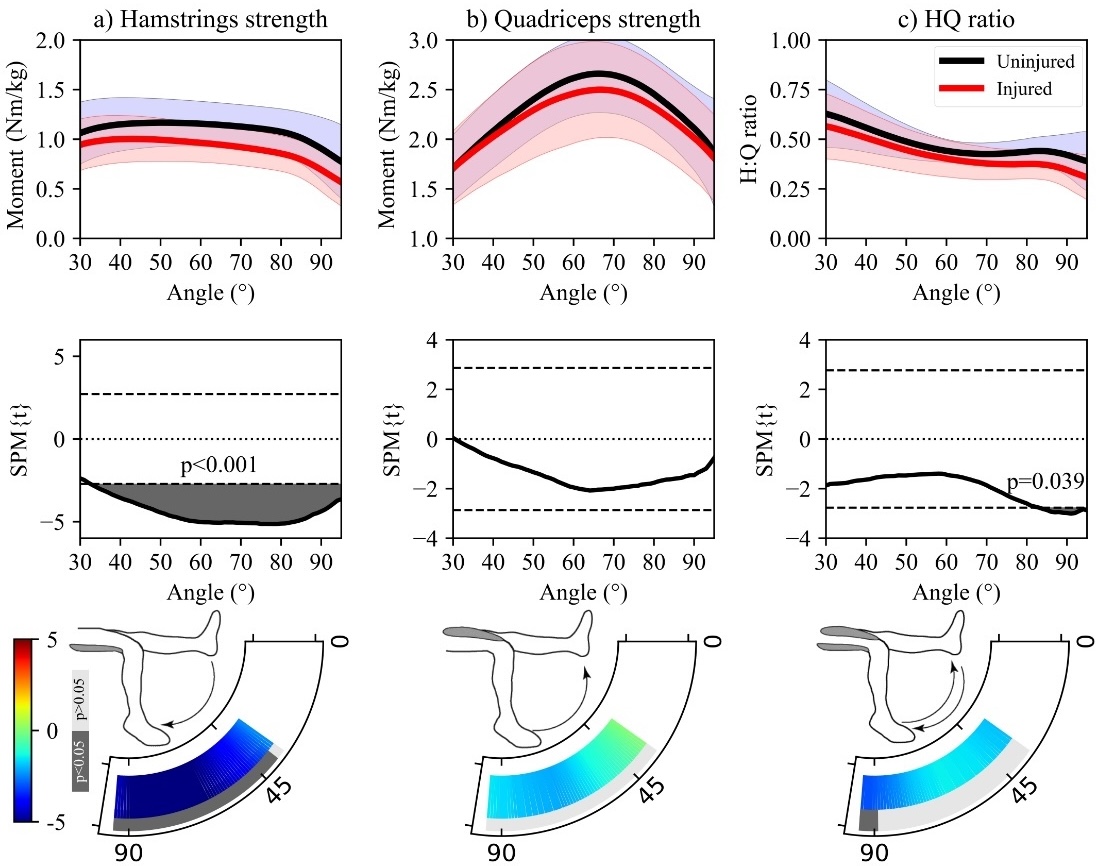
Within the ACLR athletes, the hamstrings moment-angle profile of the injured leg was significantly lower compared to the uninjured leg between 33° and 95° of knee flexion (p<0.001) at the time of RTS (Figure 2). This is most of the measured ROM. There was no significant difference between the legs in the quadriceps moment-angle profile. The angle-specific H/Q ratio profile was significantly lower for the injured leg compared to the uninjured leg, but only between 84° and 95° of knee flexion (p=0.039). Analyses of the peak values showed a significantly lower hamstrings peak moment for the injured leg compared to the uninjured leg (p<0.001) and no significant difference for the quadriceps peak moment or the peak-based H/Q ratio (Table 3).
_hamstrings_and_(b)_quadriceps_moment-angle.jpeg)
Follow-up of strength asymmetries over six months after RTS
The one-dimensional repeated measures ANOVAs showed no main time effects or interaction effects (leg time) for any of the angle-specific profiles (Figure 3). A main leg effect was found for the hamstrings and quadriceps moment-angle profiles, but not for the angle-specific H/Q ratio profile. The hamstrings and quadriceps moments of the injured leg were lower compared to the uninjured leg, respectively during the entire ROM (p<0.001) and around peak moment (61°- 92°) (p=0.013). The absence of a main time effect or interaction effect means that the identified strength asymmetries persisted throughout the six-month follow-up period. The zero-dimensional repeated measures ANOVA showed similar results. No main time effects or interaction effects were found for any of the peak-based parameters (Table 4). A main leg effect was found for the hamstrings (p<0.001) and quadriceps (p=0.004) peak moments, with significantly lower peak moments on the injured side compared to the uninjured side. No main leg effect was found for the peak-based HQ ratio.
_hamstrings_and_(b)_quadriceps_mean.jpeg)
Discussion
Added value of angle-specific strength profiles
The first objective of this study was to assess deficits and asymmetries in the hamstrings and quadriceps moment-angle profiles and angle-specific H/Q ratio profiles in athletes with ACLR at time of RTS. Both the hamstrings moment-angle profile and the angle-specific H/Q ratio profile were significantly lower in the injured leg of athletes with ACLR compared to the control participants at larger knee flexion angles (>65° knee flexion for hamstrings strength and >75° knee flexion for H/Q ratio profile). Comparing the injured to the uninjured leg of the ACLR athletes at the time of RTS, a hamstrings strength asymmetry was unveiled throughout almost the entire measured ROM (>33° knee flexion). The angle-specific H/Q ratio profile showed only significant between leg differences at larger knee flexion angles (>84° knee flexion). The peak-based analyses could only identify between-leg asymmetries for hamstrings peak moment and were not able to reveal the hamstrings strength deficit and H/Q ratio imbalances at larger knee flexion angles. This confirms the importance of analyzing angle-specific strength profiles in ACLR athletes instead of only evaluating restoration of peak strength.
The hamstrings strength deficits at larger knee flexion angles were also identified in other studies that assessed hamstrings strength in athletes that underwent ACLR surgery with a hamstring tendon graft.30–32 This hamstrings weakness in deep knee flexion has been suggested to be a possible consequence of two phenomena: 1) atrophy and shortening of the semitendinosus muscle after its tendon has been harvested for the ACL graft,23 and 2) a lack of compensation from the semimembranosus and biceps femoris.32 First, several studies showed that the musculotendinous junction of the regenerated semitendinosus is proximally shifted (i.e. tendon retraction). This retraction occurs because once the tendon is harvested there is nothing left that keeps the semitendinosus muscles fibres to length.31 Studies showed proximal shifts of the musculotendinous junction from 3.8cm33 up to even 7cm.34 Since the muscle will be of shorter length at a given flexion angle, muscle contractile behaviour will alter. Namely the angle at which the semitendinosus exhibits maximum strength will be at a more extended position of the knee.30 Second, the different hamstring muscles all have a separate origin, insertion, and muscle architecture influencing their contribution to the overall flexion strength and the ability to compensate at a specific joint angle.30 The semitendinosus plays the most important role in larger knee flexion angles because of its fusiform architecture (75-120°) while the biceps femoris, which has a pennate architecture, is the primary flexor at angles between 15-45° of knee flexion.30,32 Semitendinosus harvesting, will thus mainly affect strength in the larger knee flexion angles. The clinical relevance of these strength deficits at larger knee flexion angles during seated isokinetic dynamometry requires further investigation (Appendix B).
Evolution of strength asymmetries after RTS
The second objective of this study was to assess if strength asymmetries resolve spontaneously over the first six months following RTS. Lower hamstrings and quadriceps strength was observed in the injured leg of ACLR athletes compared to their uninjured leg which remained unchanged over the six month follow-up period. The angle-specific analyses revealed a persisting hamstrings weakness in the injured leg over the entire measured ROM and a quadriceps weakness in the injured leg around 60-90° of knee flexion, the range of the quadriceps peak moment. Several authors35–37 attribute prolonged quadriceps weakness to arthrogenic muscle inhibition (AMI), a natural mechanism of reflex inhibition of muscles surrounding an injured joint to prevent potentially detrimental movements. Rice et al.38 state that AMI in ACLR often results in the inability to fully activate the quadriceps muscle, restricting peak quadriceps moment. AMI could thus explain the current findings of prolonged quadriceps weakness around peak moment angles observed in the injured leg compared to the uninjured leg of the ACLR athletes. Early interventions, that target AMI from the first day after injury are crucial. In the acute phase, it is essential to address inflammation, pain and effusion as soon as possible.39 Furthermore, there is growing evidence supporting the efficacy of neuromodulatory strategies such as cryotherapy, TENS, eccentric cross-exercise in treating AMI.39–41
The longitudinal analyses showed that the quadriceps and hamstrings strength asymmetries, did not resolve over time. As the athletes with ACLR returned to their competitive sports without receiving additional rehabilitation after the moment of RTS, this suggests that strength asymmetries do not resolve by sports participation alone. Next to the angle-specific analysis, scientific literature has frequently reported on prolonged hamstrings17,42–44 and quadriceps9,16,17,43–45 peak strength asymmetries and deficits in ACLR athletes.37 Therefore, additional rehabilitation after RTS in the form of strength training, might be required in athletes with ACLR.44 For example, to target the hamstrings weakness, Buckthorpe et al.46 advised to prioritize eccentric hamstring training. They state that eccentric exercises have the potential to shift the moment-angle profile of the knee flexors to more extended knee angles, probably because of the positive effect of eccentric training on fascicle length.47 Similarly, concentric exercises at long muscle length might increase fascicle length48 and as such shift the moment-angle profile of the knee flexors to more extended knee angles. However, the results of this study show hamstrings strength asymmetries over the entire ROM and hamstrings strength deficits particularly at more flexed knee angles. Therefore, future studies should investigate whether adding hamstrings strength exercises at shorter muscle lengths to the rehabilitation programs reduces these persistent flexion strength deficits in athletes with a semitendinosus autograft.
Some limitations of this study have to be noted. First of all, it is important to notify that only isokinetic concentric strength at an angular velocity of 60°/s was measured. Consequently, the absolute values of this study cannot be compared to strength values or H/Q ratios measured at different angular velocities or to functional H/Q ratios that divide the eccentric knee flexor moment by the concentric knee extensor moment.17,20–22,49–51 Second, the rehabilitation program of the ACLR patients up to RTS was performed at their home physiotherapy practices and thus not standardised. Therefore, it is not possible to make any conclusion about the influence of the type of rehabilitation program on strength deficits. Part of the variability in strength deficits and asymmetries might be attributed to the various exercise programs that the ACLR athletes were exposed to during their rehabilitation.52–54 Furthermore, the patients were not all treated by the same surgeon, leading to heterogeneity in surgery technique and decision making on RTS clearance. Third, the ACLR athletes were significantly older than the controls (24.0 ± 4.3 vs. 21.8 ± 1.5 years, p=0.043). Although, strength declines with age, it is not expect that this small difference in age has a relevant impact on the results of this study as strong strength declines are only seen around 40 years of age.55 Finally, the small sample size and relatively short follow-up, did not allow to evaluate the predictive value of angle-specific strength measures or H/Q ratios for ACL re-injury.
Conclusion
This study revealed clear angle-specific strength deficits and asymmetries in ACLR athletes at time of RTS that persisted for six months after athletes who had undergone ACLR returned to sport. More specifically, ACLR athletes have lower quadriceps strength in the injured leg compared to their uninjured leg around the angle of peak moment. Furthermore, their injured leg showed lower hamstrings strength compared to their uninjured leg throughout the entire measured ROM and compared to controls at larger knee flexion angles. The latter deficit was not identified with a traditional peak-based analysis, which stresses the need for angle-specific analyses. Since the strength asymmetries did not resolve naturally in the first six months after RTS, additional targeted interventions are needed to restore these shortcomings.
Acknowledgements
We wish to recognise Ian Poole, Raja Mohammed Firhad Raja Azidin, Anne Delextrat and Vasilios Baltzopoulos for their contribution to the development IKD1D and the drafting of supplementary materials.
Funding
The researchers received funding of FWO Flanders (G068221N) and internal funding of KU Leuven (C24M/21/042).
Conflict of interest
The authors have no conflicts of interest to report.