INTRODUCTION
Dynamic knee valgus (DKV), also known as dynamic genu valgus is defined as a lower limb movement pattern that is a combination of internal rotation and adduction of the femur, knee abduction, anterior tibial translation, and external tibial rotation.1 The normal range of DKV of a single-leg landing task has been reported as 1-9 degrees for males and 5-12 degrees for females when measured from a digital video camera two-dimensionally.2 Anatomical characteristics contribute to DKV, with the Q-angle being the most significant.3–5 Q-angles are measured with similar, although different anatomical landmarks than knee valgus. DKV and static knee valgus are measured from the Anterior Superior Iliac Spine (ASIS) to the mid-patella to a line along the tibia between the medial and lateral malleoli. Meanwhile, Q-angle is measured from the ASIS, through the mid-patella, and ending on a line through the middle of the tibial tubercle.
Health professionals and coaches traditionally have considered DKV as being associated with increased risk of injuries and decreased jump performance. This has commonly led to a “knees out” cueing to prevent DKV during athletic performance, to the point that some clinicians attempt to avoid any degree of DKV. For example, the International Olympic Committee has published a review on ACL injuries encouraging clinicians to avoid excessive dynamic knee valgus and focus on a knee over toe position.6 Additionally, static anatomical measurements, such as Q-angle and Craig’s test, are rarely considered when providing feedback to athletes regarding their DKV.
Presently, there is contradictory evidence on DKV and injury risk.7–13 The 2005 prospective study by Hewett et al. identifying DKV as the primary culprit of ACL injury in female athletes has most commonly been referenced by clinicians as the reason to avoid DKV.10 This study reported those suffering an ACL injury (n=9) had 8 degrees more DKV than those who did not (n=196).10 Conversely with a similar set-up Nilstad et al. identified no association between DKV and ACL tears in female athletes who sustained an ACL injury (n=56) compared to uninjured athletes (n=722).7 When synthesizing the body of literature on DKV and ACL injuries, a 2020 meta-analysis of the nine highest quality articles with over 1300 total subjects found no association between DKV and ACL injuries.8
Additionally, many studies suggest a positive association between DKV and patellofemoral pain, stress fractures, iliotibial band syndrome, and Achille’s tendinopathy. However, these studies have not considered the static bony anatomy of the subjects, overlooking the possible contributions of anatomical characteristics.3–5 In parallel, bony anatomy of static knee valgus was found to have a significant relationship with DKV during a drop-jump, while foot alignment, hamstring strength, quadriceps strength, and hip abductor strength had no association.3 Furthermore, anatomical measurements in both the frontal and transverse planes at the hips and knees have been shown to have an association with DKV during double-leg landing, further adding value to the idea that anatomical differences contribute to dynamic measures.14
Moreover, there is conflicting evidence on the relationship between DKV and jump performance.5,15–17 Confounding variables such as specific training effects and bony anatomy was not considered with these reports. There is also dispute regarding the neuromuscular contributions to DKV, specifically, the association of hip abductor muscle weakness to DKV.5,18–22 Finally, interventional studies for improving DKV have had mixed results, with some studies demonstrating improved DKV with training proximally at the hip and core, while others found no change.23,24 Seeing that there is conflicting evidence surrounding the current consensus on DKV, additional information is needed to establish a better understanding of these relationships. The purpose of this study was to assess jump performance measures and anatomical contributions.
METHODS
Study Design and Subjects
This cross-sectional study recruited 50 subjects from the university wellness center between the ages of 18 and 30 years old who felt they could complete nine single leg depth jumps from a 6-inch box with each leg. A depth jump consists of dropping from a box of a predetermined height and immediately, upon landing a single maximal jump is performed.25 All subjects were recruited from a common area near the entrance of the wellness center. All data were collected at this location as well. The subjects were incentivized with a sports drink for their participation. Fifteen subjects were excluded following poor execution of a cued jump for dynamic knee valgus, primarily due to turning their foot inward. After consenting to the research, background demographic information including sex, age, weight, height, injury history, and past sport participation was collected from subjects. BMI was later calculated based on the subjects’ self-reported height and weight.
Static anatomical measurements of transverse plane femoral anteversion and frontal plane genu valgus were completed by the same researcher. Femoral anteversion was measured with the Craig’s test, while genu valgus was measured with Q-angle26 and static knee valgus. Craig’s test is the most commonly used clinical assessment of femoral anteversion, however, the validity of this test has been questioned.27 Souza and Powers reported good reliability with a strong positive correlation (r=.61, p<0.01) when compared with MRI measurements of femoral anteversion.28 This suggests that Craig’s test can be a useful clinical test for screening femoral anteversion without higher costs associated with imaging.
Static knee valgus and 2-Dimensional DKV utilize the same landmarks: from the subject’s ASIS, through the mid-patella, and ending at the midline of the anterior tibia between the medial and lateral malleoli. Q-angle was measured from the ASIS, through the mid-patella, and ending on a line through the middle of the tibial tubercle. Both the Q-angle and static knee valgus were measured in supine. Landmarks were marked with either tape or marker to facilitate recording of DKV. The sample size was determined using G*Power Version 3.1.9.7 with .05 alpha, .8 power, and a medium-large effect size of .5 resulting in 34 subjects needed, thus, 50 were recruited in anticipation of dropouts and excluded subjects.
Variables
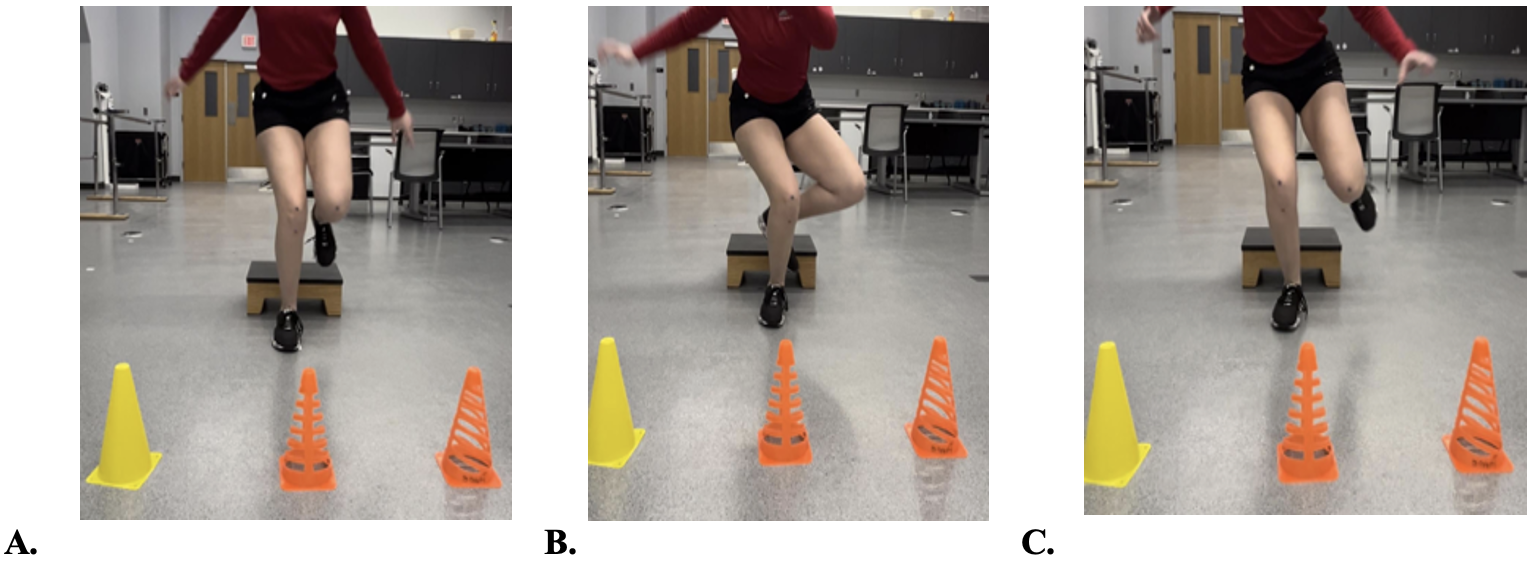
The independent variables were the three single-leg depth jump modes: a natural jump form, jump form with cued DKV, and jump form cued for no DKV. The natural depth jump (Figure 1a) consisted of the subjects jumping with no cue. The DKV cued depth jump (Figure 1b) consisted of a “knees-in” verbal cue with an external reference cone 30 degrees medial. The no DKV cued depth jump (Figure 1c) consisted of a verbal “knees straight forward” cue with an external reference cone directly in front of the landing zone. A single-leg depth jump was chosen over a double-leg, due to the greater amount of knee valgus that often occurs with single-leg.29 The different jump forms were chosen to assess changes in jump performance based on DKV angles.

The dependent variables measured were jump height, ground contact time, reactive strength index (RSI), and DKV of the jump. Additionally, a true DKV measurement, normalized for frontal plane anatomical measurements, was collected consisting of subtracting the subject’s static knee valgus from their DKV measurements. True DKV was calculated as it represents the degree of frontal plane motion that was occurring, controlling for anatomical differences between subjects. True DKV provides insights into DKV motor control. Three trials were collected for each leg and each jump with means being recorded for each subject. Static anatomical measurements included Craig’s test for femoral anteversion, Q-angle for genu valgus, and static knee valgus for genu valgus.26 Static knee valgus was used in calculating true DKV measurement as it was the most ecologically similar to DKV and it had the highest and strongest correlation with DKV (r=.37, p=0.03).
Data sources/measurements
The MyJump2 application was used to measure ground reaction time, RSI, and jump height. MyJump2 is a reliable and valid tool, frequently used in jump studies.30–32 The Coach My Video application was used to measure DKV. DKV was measured at the most extreme point, often at the deepest point of the depth jump. 2-D phone-based apps have been found reliable and validated for assessing kinematics.33–35 The apps were installed on a university issued iPad.
A 6-inch box was used for the depth jump with an iPad placed seven feet in front of the box with the camera mounted 15 inches from the ground to standardize recordings of the jumps. To ensure focus on jump performance, subjects were told to jump as high and as quickly as possible. Each jump was demonstrated by the same researcher for every subject. The subjects were cued with “Point your knee towards the cone.” Subjects were given the option to perform a slow, step-through practice trial as well as full-speed practice trials. Subjects were given as many practice trials as they felt necessary to gain full understanding of the test. All subjects began with their natural jump form (Figure 1a), completing three jumps with their right and then three on their left. Random numbers were used to determine whether the cued DKV (Figure 1b) or cued no DKV (Figure 1c) would be the second or third set of jumps. The same procedure of completing three jumps for the right leg was completed before switching to the left for the cued jumps.
Bias
To ensure reliability of anatomical characteristics, the same researcher placed markers on designated landmarks and measured Q-angle, static knee valgus, and Craig’s test for all sessions. Craig’s test validity is not that of CT or MRI, although it is regarded as an acceptable clinical exam to screen for femoral anteversion in the absence of imaging.27,28 Therefore, transverse plane anatomical contributions to DKV should be interpreted cautiously. Randomization of the DKV and no DKV jumps was used to reduce order effects. Performance bias was controlled with a standardized assessment preserving fidelity of the protocol. The high reliability of the measurement techniques used to assess jump performance and DKV ensures quality of the data. Two blinded researchers not associated with the study assessed the jump performances and kinematics at a different and neutral site, minimizing expectation bias. There was no missing data.
Statistical Methods
All statistical analysis was completed with SAS. All alphas were set at 0.05. Normality of the jump variables were assessed with Shapiro-Wilk, Histograms, and Q-Q plots.36 ANOVA was used to compare jump height, contact time, RSI, and DKV with each jump method. Pearson Correlation Coefficients were used to assess DKV and anatomical measurements, jump height, ground contact time, and RSI. Intraclass correlation coefficient (ICC) was used to assess inter-rater reliability of the measurement tools. Strength of correlations was described using the following scale outlined by the British Medical Journal: 0-0.19 is regarded as very weak, 0.2-0.39 as weak, 0.40-0.59 as moderate, 0.6-0.79 as strong, and 0.8-1 as very strong correlation.37
RESULTS
Subjects
Fifty subjects were recruited and completed the study. Following analysis of the jump data, 15 subjects’ data were excluded as they did not complete the cued DKV jump correctly, pointing their feet too far towards midline. The remaining 35 subjects were included in final data analysis.
Descriptive Data
The average age of subjects was 21.91 years-old (95% CI 21.12-22.71). Their average height was 68.97 inches (95% CI 67.81-70.13). Their average weight was 165.94 pounds (95% CI 154.93-176.96). Their average BMI was 24.38 (95% CI 23.15-25.61). Their average Q-angle was 16.26 degrees (95% CI 14.86-17.66). Static knee valgus was 9.90 degrees (95% CI 8.94-10.86). Craig’s test was 9.40 degrees (95% CI 8.57-10.23). Over half (51.4%) of subjects had past physical therapy, 42.9% had a history of significant lower extremity injury, and 77.1% had past jump training. All subject characteristics can be found in Table 1.
When stratifying the study characteristics by sex, five variables were significantly different between females and males. Weight, height, BMI, Q-angle, and static knee valgus were all statistically different. See Table 2 for subject characteristics stratified by sex.
Outcome Data
The average normal single leg depth jump height was 5.87 inches (95% CI 4.99-6.76). The average contact time was 419.72 ms (95% CI 388.71-450.73). The average RSI was .86 (95% CI .76-.97). The average DKV with the subjects’ natural jump was 13.12 degrees (95% CI 11.29-14.96). The true DKV was 3.22 degrees (95% CI 1.50-4.95). Table 3 contains the jump performance data of the included subjects.
Jump height and DKV were significantly different when comparing the jump performances based on sex. Interestingly, there were no statistically significant differences for DKV between sexes once the measure was normalized for static frontal plane anatomical measures, also known as the true DKV. See all subject jump characteristics stratified by sex in Table 4.
Main Results
Performance and DKV averages for each jump type can be found in Table 5. There was no difference in jump heights between jump types (p=0.59). There was a significant difference between contact times, with the cuing for DKV jumps being longer than the natural (p= 0.03) and cuing for no DKV jumps (p=0.04). RSI was significantly lower for the jump cued for DKV compared to the natural jump (p=0.03). Cuing for DKV was effective, as those jumps had a significantly higher DKV (p<0.01) than the natural jump and cuing for no DKV. Interestingly, the jumps in which subjects were cued for no DKV did not lower the DKV below the subjects’ natural jumps.
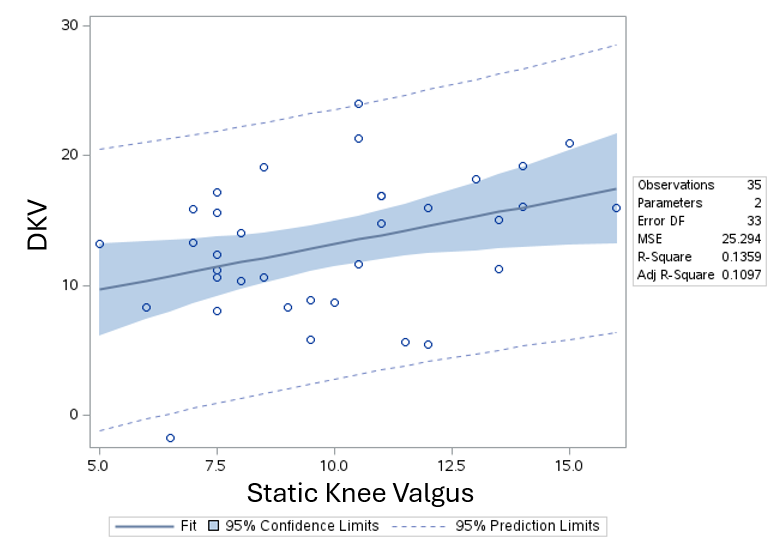
Craig’s test was not correlated to DKV measurements of natural jumps (p=0.72). Both static knee valgus (r=.37, p=0.03) and Q-angle (r=.34, p=0.04) had positive, weak significant correlations with DKV measurements for the subjects’ natural jumps. Static knee valgus demonstrated a greater positive significant correlation with DKV than the traditional Q-angle and the adjusted R-square suggests that the static knee valgus accounts for 11% of the DKV (Figure 2).

The ICC for jump height, ground contact time, and RSI measurements taken with the MyJump2 app was near perfect at .99 for each. The ICC for DKV measured with the Coach My Video app was also very strong at .96.
DISCUSSION
This study highlights the need to consider static bony alignment when assessing DKV with jump performances, as the differences in DKV between sexes was accounted for by the frontal plane anatomy. Poor clinical decision making can occur when making assumptions about movement faults without measuring anatomical contributions. Furthermore, static knee valgus could be considered over the use of Q-angles since using the same landmarks for static and dynamic tasks increases the ecological validity of applying static measurements. That being so, the static knee valgus measurements were more highly correlated to DKV in this study.
Since the no DKV cued jump did not lower the DKV of subjects, in fact, increased it, the researchers question the effectiveness of using an external visual cue. When cued for DKV, ground contact time had a significant correlation with true DKV measurements, suggesting that when a patient has high DKV, instead of cuing to keep the knee from caving in, clinicians could cue for less contact time to indirectly control DKV. While external cuing has demonstrated effectiveness, it traditionally has not focused on contact time for improving DKV.38–40 Motor learning studies have found that cuing for contact time has improved both ground contact time and RSI, however, these studies have not assessed the impact on DKV.41,42 RSI was significantly lower for the jump cued for DKV compared to the natural jump (p=0.03), likely related to the contribution of contact time on RSI. However, increased impulse and impact forces have been associated with cueing for less ground contact time, both of which have been linked to increased injury risk.41,43,44
When considering improving jump height, this study did not find any difference within subjects when considering DKV. This is comparable to findings on squat jumps and countermovement jumps in past research.16 This study’s findings were contrary to a 3-month interventional study that found improved jump height with an exercise program targeting less DKV.17 However, that interventional study only had eight subjects complete the intervention and did not control for confounding that the improvements in jump height could be linked to improved strength and power from the exercise program and not decreased DKV.17
The high reliability of the apps found in this study is encouraging for clinicians without an expensive performance laboratory. These apps are readily accessible and do not require extensive time and monetary investments. When considering this along with the high reliability and validity of 2-D phone apps found in past studies, clinicians can be confident in the reliability of using app-based 2-D analysis tools for assessing jump performance and DKV.30–35
It must be noted that the population used in this study was primarily college students, but that does not change the fact that their anatomical alignment contributes to their DKV. These considerations are most dramatic for females, as females typically have increased frontal plane knee valgus and femoral anteversion, both of which can masquerade as DKV if not assessed.4 Additionally, the validity of craig’s test has been questioned, potentially over or underrepresenting transverse plane anatomical contributions in this study. Thirty percent of subjects were excluded due to not being able to complete the cued DKV jump correctly, these subjects could have swayed the results or could have added statistical power if included. Additionally, the fact that 30 percent of the subjects struggled with the cued DKV jump suggests difficulty in completing the task and possibly less validity when comparing to natural jumping mechanics. Participants who had experienced past injuries, physical therapy, and jump training were not excluded from this study. The influence of previous rehab and jump training may have impacted performance throughout this study. Additionally, the external cuing may have caused subjects to focus more on the cone rather than their best jump performance.
CONCLUSION
Bony alignment should be considered with kinematics, as normalization of DKV measurements by static anatomical measurements controlled for the differences in DKV between men and women during subjects’ natural jumping performance. When jumping with cued DKV alignment, ground contact time had a significant positive correlation with DKV measurements, therefore cueing for less ground contact time may be an external cue to use to control for excessive DKV, although prospective studies would be needed to test this in the future.
Conflicts of interest
The authors declare no conflict of interest.