INTRODUCTION
Squatting exercises are described in clinical practice guidelines for patellofemoral pain (PFP) both for diagnosing PFP and to be used as an rehabilitation intervention.1 While several studies have quantified patellofemoral force and stress during squatting exercises,2–10 it is unclear how different types of squat exercises load the patellofemoral. Moreover, it is not well understood what patellofemoral joint force or stress magnitudes, and over what time interval, can lead to PFP. There are several factors that can contribute to PFP, including weakness in the quadriceps or hip external rotators, tight quadriceps, hamstrings, or iliotibial band, overuse or trauma, dysfunctional extensor mechanism, malalignment of the lower extremity, and excessive rear-foot pronation.1,11 Repetitive and high patellofemoral stress may result in or worsen PFP and adversely affect soft tissues surrounding the patellofemoral joint, including infrapatellar fat pad, synovial plicae, retinacula, joint capsule, and patellofemoral ligaments.11 High magnitude patellofemoral joint force can also increase subchondral bone stress in the patellofemoral joint.12 Because subchondral bone plates are abundant in pain receptors,13 high subchondral bone stress may result in or exacerbate PFP.11 High magnitude patellofemoral joint stress can result in a decreased ability of the cartilage to distribute and absorb patellofemoral force, resulting in cartilage degeneration.12 A better understanding of patellofemoral joint force and stress magnitudes among different squatting exercises, technique variations, and functional activities may facilitate rehabilitation of those with PFP.
Repetitive and large patellofemoral force magnitudes that occur during sport can result in high patellofemoral joint stress (patellofemoral force/patella contact area), which over time can result in PFP. Squatting exercises, such as those performed on an unstable BOSU ball (also referred to as BOSU Balance Trainer) versus a stable level ground, are often used for strengthening of thigh and hip musculature and are important training and rehabilitation exercises to enhance patellofemoral joint stability and improve optimal articulation between the femur and patella during sport and activity.2–10 Understanding the force and stress magnitudes at the patellofemoral joint and how they vary while performing one-legged and two-legged BOSU and floor squats may be helpful to clinicians when prescribing and progressing squatting exercises to individuals with PFP.
There are no known studies that have examined patellofemoral force and stress between the bodyweight one-legged and two-legged BOSU and floor squat exercises. In patellofemoral rehabilitation progression, squatting exercises are usually initially performed with no external resistance (bodyweight only) and progressed to employing external weights (dumbbells or barbells) or other external resistance, such as resistance bands.1 This progression increases both hip and thigh muscle recruitment and patellofemoral force and stress.2–4 The floor squat, and presumably the BOSU squat also, are commonly progressed in knee rehabilitation starting with a two-legged squat and progressing to a one-legged squat.1 Although progressing the exercises may increase the loads on hip and thigh musculature and subsequently increase hip and thigh strengthening, these exercises may also increase PFP as patellofemoral joint loading increases, and this needs to be considered when progressing patients with PFP using squatting exercises. Through visual observation, squatting on BOSU versus squatting on a level ground produces differences in squat kinematics, such as a greater forward trunk tilt when squatting on a BOSU. It is plausible that these differences in squat kinematics may affect patellofemoral loading (which is directly proportional to quadriceps loading) given that squatting with a more forward trunk tilt likely increases hamstrings activity and may also decrease quadriceps activity, which would imply potentially less patellofemoral loading with the BOSU squat compared to the floor squat. Therefore, the purpose of this study was to quantify patellofemoral force and stress between two squat type variations (BOSU squat versus floor squat) and between two leg variations (one-legged squat versus two-legged squat). The hypotheses were that patellofemoral force and stress would be greater performing the floor squat compared to the BOSU squat, and greater performing the one-legged squat compared to the two-legged squat.
METHODS
Subjects
Sixteen healthy participants without a history of patellofemoral pathology were recruited by bulletin board announcements, posters, flyers, brochures, and e-mail distributions within the California State University, Sacramento community. Inclusion criteria were being able to perform BOSU and floor squats pain-free with proper technique for 12 repetitions using bodyweight and having at least five years’ experience in performing squatting exercises, including previous experience squatting on a BOSU. Based on pilot work measuring forward trunk tilt in experienced squatters during one-legged and two-legged squats, inclusion criteria also included a forward trunk tilt from a vertical position at the lowest portion of the squat of approximately 30°-40° for the floor squat and approximately 40°-50° for the BOSU squat. Exclusion criteria were not being able to perform both one-legged and two-legged BOSU and floor squat exercises, not being able to achieve approximately 100°-100° of knee flexion at the lowest position of the squat, and any history of lower extremity surgery or injury. All participants provided written informed consent in accordance with the Institutional Review Board at California State University, Sacramento.
Exercise Description
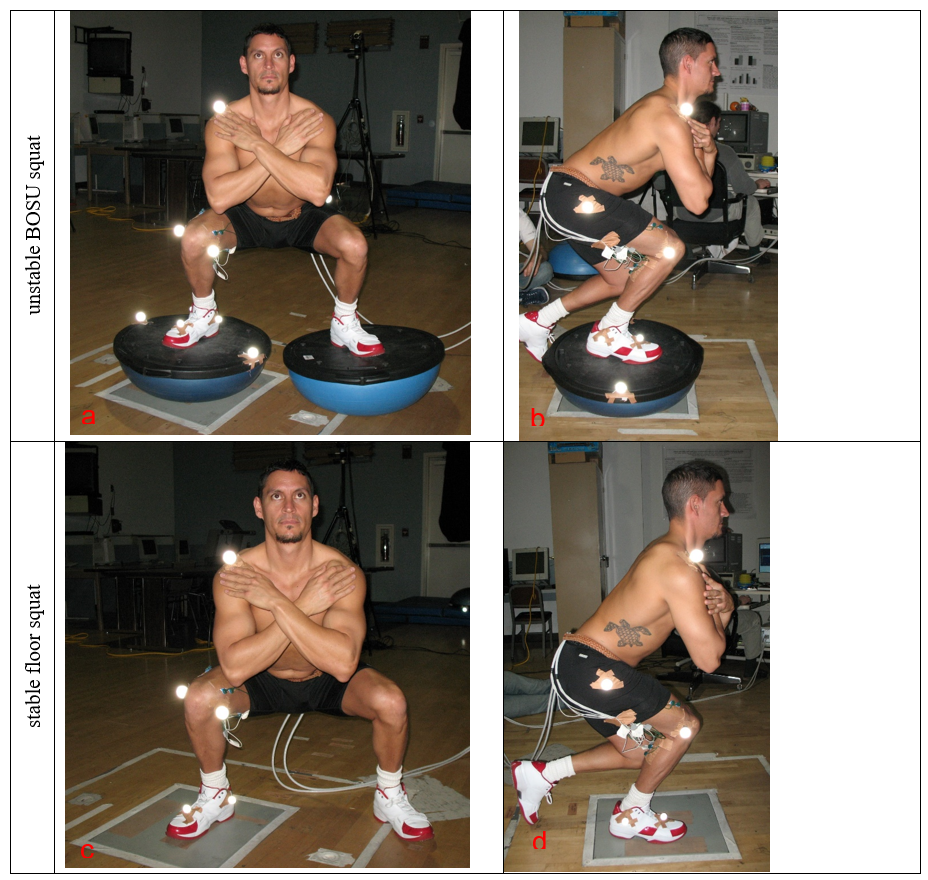
Each participant attended a pre-test session one week prior to testing and practiced performing the one-legged and two-legged BOSU (Figures 1a and 1b) and one-legged and two-legged floor squats (Figures 1c and 1d). The position of the feet for both the two-legged BOSU and floor squats were the same for both exercises for each subject and in accordance with each subject’s preference. Both feet were positioned slightly wider than hip width and had a mean±SD inside heel to inside heel distance of 50.1±3.3 cm for males and 47.9±1.2 cm for females. Moreover, both feet were slightly turned outward from the direction the subject was facing, with a mean±SD foot angle of 20.8±4.3° cm for males and 23.1±5.2° for females. For both the one-legged and two-legged floor squat, the right foot was positioned on an AMTI force platform (Model OR6-6-2000, Advanced Mechanical Technologies, Inc.) which was flush with the floor. For the two-legged floor squat the left foot was positioned on the floor. For the one-legged squat, the right foot was positioned on an AMTI force platform for the floor squat and on the flat platform side of the BOSU for the BOSU squat, with the dome side of the BOSU positioned on an AMTI force platform (Figures 1b and 1d). For the two-legged BOSU squat, each foot was placed on the flat platform side of the BOSU with the dome side of one BOSU positioned on an AMTI force platform and the dome side of a second BOSU positioned on the floor (Figure 1a).
The starting position for the two-legged squat exercises was with both knees fully extended, and the ending position was at maximum knee flexion at the lowest position of the squat, as shown in Figures 1a and 1c. The starting position for the one-legged squat exercises was with the right knee fully extended and the left knee flexed, and the ending position was in a squat position with the right knee maximally flexed at the lowest position of the squat, as shown in Figures 1b and 1d. A metronome was employed for all squat variations and set at 25 bpm to help ensure the knee(s) flexed and extended slowly at approximately 45°/s during both the squat descent and squat ascent. This resulted in a squat descent of approximately 2.33 sec to achieve approximately 100°-100° knee flexion at 45°/s, and a squat ascent of 2.33 sec to fully extend the knees at 45°/s. Therefore, for each squat repetition, a first metronome beat presented the start of the squat descent, the second metronome beat represented maximum squat descent, and the third metronome beat represented the end of the squat ascent.
__unstable_bosu_squat_one-legged_(b)__stable_floor_squat.png)
Data Collection
Blue Sensor (Ambu Inc., Linthicum, MD) disposable surface electrodes (type M-00-S; 22 mm wide, 30 mm long) were used to collect EMG data and were positioned along the longitudinal axis of each muscle in a bipolar configuration, with a center-to-center distance of 3 cm between electrodes. Before applying the electrodes, the skin was shaved, abraded, and cleaned with isopropyl alcohol wipes in order to decrease skin impedance. Using locations previously described,3,4,8 electrode pairs were placed on the participant’s right side for the following muscles: a) rectus femoris; b) vastus lateralis; c) vastus medialis; d) medial hamstrings (semimembranosus and semitendinosus); e) lateral hamstrings (biceps femoris); and f) gastrocnemius (middle portion between lateral and medial bellies).
For three-dimensional (3D) motion capture, spheres (3.8 cm in diameter) covered with reflective tape were attached to adhesives and positioned over the following bony landmarks as described previously3,4,8: a) medial and lateral malleoli of right leg; b) third metatarsal head of right foot ; c) upper edges of lateral and medial tibial plateaus of right knee; d) posterosuperior greater trochanters of left and right femurs; and e) lateral acromion of right shoulder.
After the spheres and electrodes were in place, the participant warmed-up and practiced all squat exercises until they felt warmed up and ready to be tested, and then data collection began. An eight-camera Vicon-Peak Performance motion analysis system (Vicon-Peak Performance Technologies, Inc., Englewood, CO) was employed for 60 Hz video data collection. Force data were collected at 960 Hz using an AMTI force platform (Model OR6-6-2000, Advanced Mechanical Technologies, Inc.). EMG data were collected at 960 Hz using a Noraxon Myosystem unit (Noraxon USA, Inc., Scottsdale, AZ). EMG amplifier bandwidth frequency was 10-500 Hz with an input impedance of 20,000 k. The common-mode rejection ratio was 130 dB. Video, force, and EMG data were all electronically synchronized and simultaneously collected employing a randomized order with each participant performing one set of three repetitions for one-legged and two-legged BOSU and floor squat exercises. A two minute rest period was given between performing each of the four exercise variations. The BOSU ball was filled with an amount of air which caused the dome to be approximately 21.6 cm high, as recommended by the manufacturer.
Subsequent to completing the four squat exercises, EMG data were collected during maximum voluntary isometric contractions (MVIC) to normalize EMG data, as described previously.3,4,8 The MVIC for the rectus femoris, vastus medialis, and vastus lateralis were collected in a seated position at 90° knee and hip flexion during a maximum effort knee extension. The MVIC for the lateral and medial hamstrings were collected in a seated position at 90° knee and hip flexion during a maximum effort knee flexion. MVIC for the gastrocnemius was collected during maximum effort unilateral stance heel raise while standing, employing an ankle position halfway between neutral and full plantar flexion. Two trials (each five seconds in duration) were collected for each MVIC for each muscle in a randomized order for all three muscle groups, and a two minute rest interval was given between the two trials and between each muscle tested. The MVIC was calculated using the highest EMG signal over a one second time interval during the five-second MVIC trials, as described previously.3,4,8
Data reduction
Video images from the reflective markers were tracked and digitized in 3D space with Vicon-Peak Performance software, employing the direct linear transformation calibration method. The calibration system accuracy resulted in reflective markers that could be located in 3D space with an error less than 0.3 cm. Raw position data were smoothed using a double-pass fourth-order Butterworth low-pass filter, using a cut-off frequency of 6 Hz.3,4,8 Joint angles, linear and angular velocities, and linear and angular accelerations were calculated employing appropriate kinematic equations, as described previously.3,4,8
The raw EMG signals were full-wave rectified, smoothed with a 10 ms moving average window, and linear enveloped throughout the knee flexion range of motion for all repetitions.3,4,8 EMG data were then normalized for each muscle and expressed as a percentage of each participant’s highest corresponding MVIC trial. Normalized EMG data for all three trials (repetitions) were averaged at corresponding knee angles between 0°-100° with 0° defining full knee extension, 0°-100° defining the squat descent, and 100-0° defining the squat ascent. EMG data were used to calculate patellofemoral force and stress in a knee biomechanical model (see Appendix) and were not analyzed separately.
Data Analysis
A repeated-measures 2-way analysis of variance (ANOVA) was employed for each 10° knee angle (from 10° to 100°) during the squat descent and each 10° knee angle (from 100° to 10°) during the squat ascent in order to assess the effects of squat type (BOSU versus floor squat) and leg type (one-legged versus two-legged) on patellofemoral compressive force and stress. The level of significance employed was p < 0.01. Bonferroni t-tests were used to assess pairwise comparisons among the four squat conditions.
RESULTS
Sixteen healthy participants were studied, with a mean (±SD) age, mass, and height of 29.3±7.6 y, 76.9±6.5 kg, and 176.0±2.4 cm, respectively, for males, and 30.7±9.6 y, 61.4±6.6 kg, and 166.5±8.3 cm, respectively, for females. Tables 1 and 2 provide patellofemoral joint force and stress values between the two squat type conditions collapsed across both leg conditions. The p-values shown in Tables 1 and 2 for the squat type conditions represent the main effects of the ANOVA. When collapsed across the one-legged and two-legged squat type conditions, patellofemoral joint force and stress were significantly greater (p < 0.01) in the floor squat compared to the BOSU squat at 40°, 50°, and 70° knee angles during the squat descent and 60° and 50° knee angles during the squat ascent.
When collapsed across the BOSU squat and the floor squat, patellofemoral joint force and stress were significantly greater (p < 0.01) in the one-legged squat compared to the two-legged squat for all knee angles during the squat descent and the squat ascent.
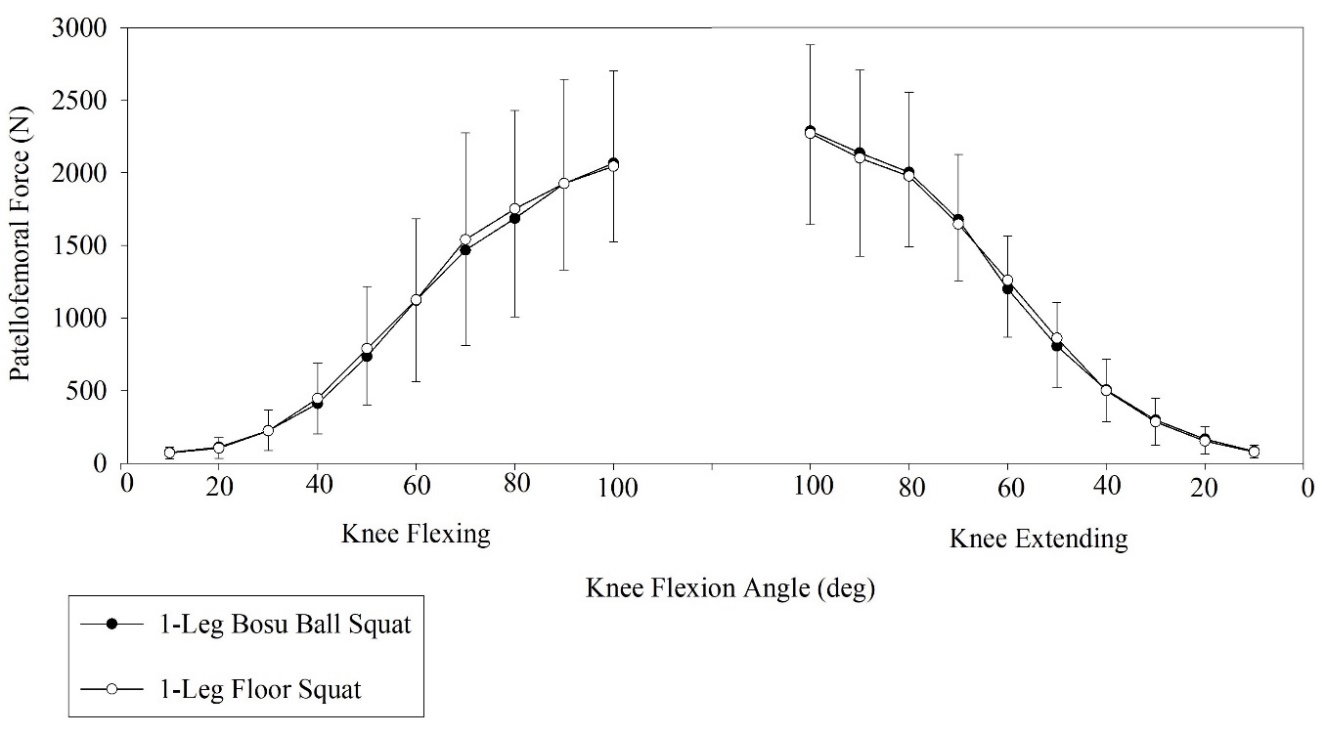
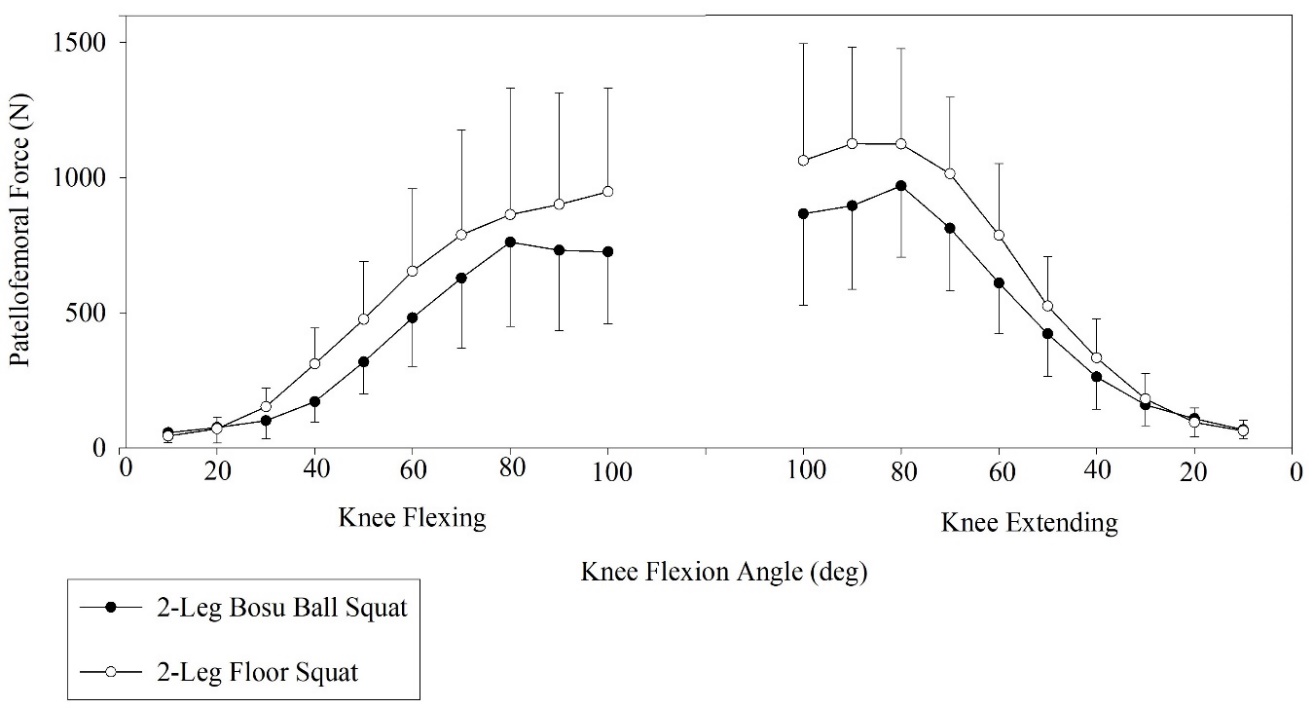
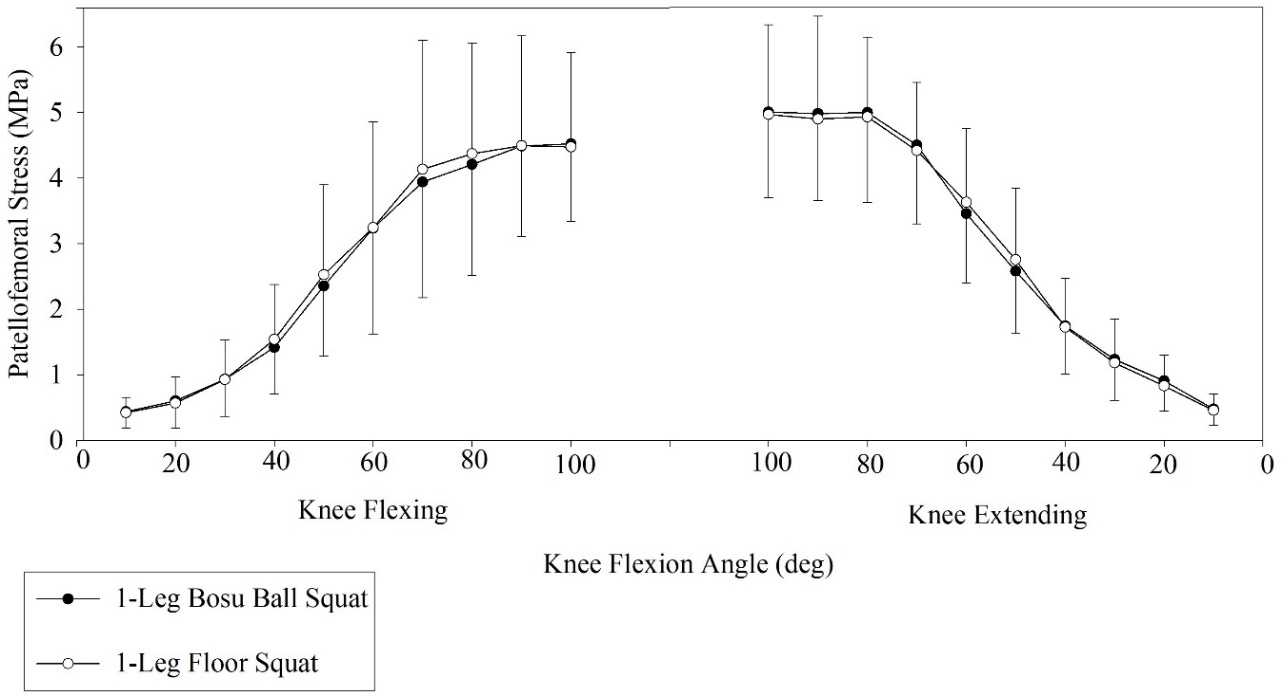
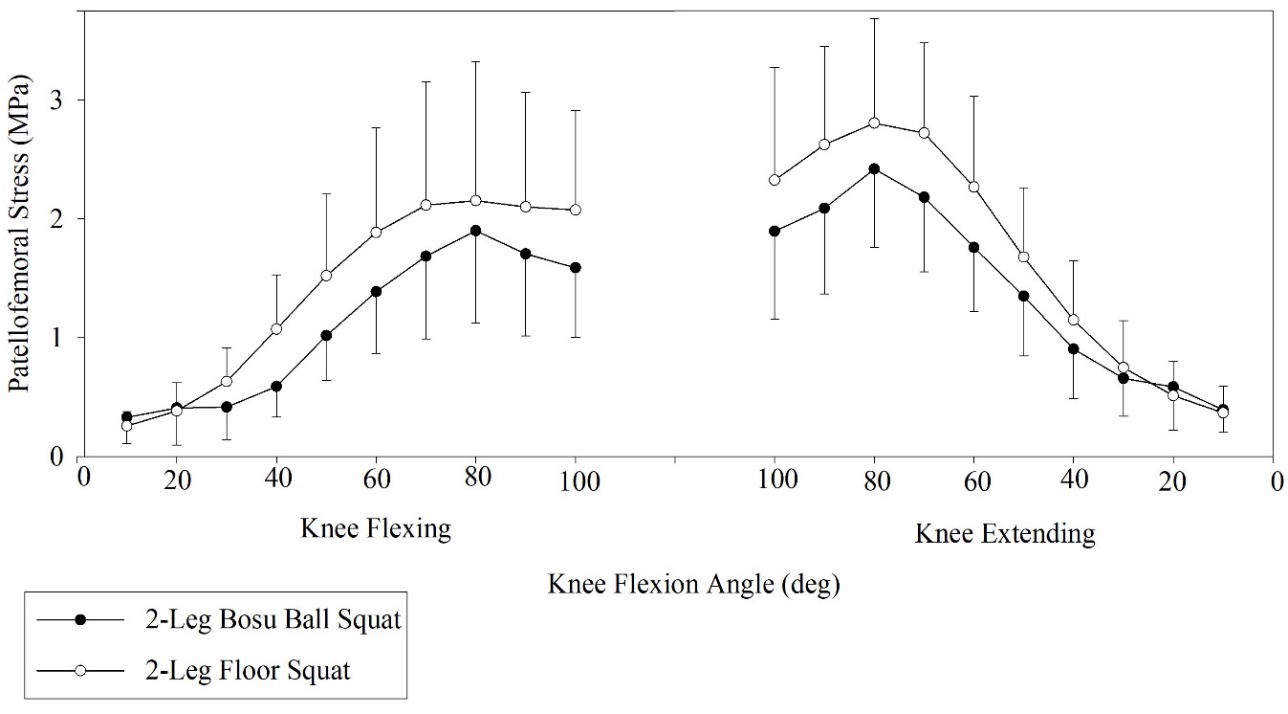
Significant interactions (p < 0.01) between squat types and leg conditions were found at 30°, 40°, 50°, 60°, and 100° knee angles during the squat descent, and 100°, 90°, 80°, and 70° knee angles during the squat ascent. Patellofemoral joint force and stress were significantly greater (p < 0.01) in the two-legged floor squat compared to the two-legged BOSU squat, but no significant differences were found between the one-legged floor squat and the one-legged BOSU squat (Figures 2a, 2b, 3a, and 3b). Patellofemoral joint force and stress generally increased progressively as knee flexion increased during the descent phase and decreased progressively as knee flexion decreased during the ascent phase. Moreover, for a given knee angle, patellofemoral joint force and stress were generally slightly greater during the ascent phase compared to the descent phase. For the one-legged and two-legged floor squat exercises, at the lowest portion of the squat the trunk was tilted forward approximately 30°-40° from a vertical position. In contrast, for the one-legged and two-legged BOSU squat exercises, at the lowest portion of the squat the trunk was tilted forward approximately 40°-50° from a vertical position.
_patellofemoral_compressive_force_between_one-legged_bosu_squat_and_one-legged_f.jpeg)
_patellofemoral_compressive_force_between_two-legged_bosu_squat_and_two-legged_f.jpeg)
_patellofemoral_compressive_stress_between_one-legged_bosu_squat_and_one-legged_.jpeg)
_patellofemoral_compressive_stress_between_two-legged_bosu_squat_and_two-legged_.jpeg)
DISCUSSION
This is the first known study that examined the effects of performing one-legged and two-legged BOSU and floor squats on patellofemoral force and stress. As hypothesized, patellofemoral force and stress were greater performing the floor squat compared to the BOSU squat, and greater performing the one-legged squat compared to the two-legged squat. The greater patellofemoral force and stress when performing the floor squat compared to the BOSU squat may in part be due to less forward trunk tilt in the floor squat (approximately 30°-40° from a vertical position) compared to the BOSU squat (approximately 40°-50° from a vertical position). One plausible explanation is that squatting with less forward trunk tilt (floor squat) moves the center of mass (COM) of trunk/arms/head posterior away from the knees, thus increasing the external knee flexor moment arm and torque produced by COM of trunk/arms/head. Conversely, squatting with greater forward trunk tilt (BOSU squat) moves the COM of the trunk/arms/head anterior towards the knees, thus decreasing the external knee flexor moment arm and torque. Thus, a greater knee extensor muscle torque and quadriceps force would be needed during the floor squat to overcome the greater external knee flexor torque, and less knee extensor muscle torque and quadriceps force is needed during the BOSU squat because of less external knee flexor torque. Since patellofemoral loading is directly proportional to quadriceps force (Figure A2 in Appendix), potentially greater quadriceps force in the floor squat may result in greater patellofemoral loading in the floor squat compared to the BOSU squat. However, this simplistic explanation is actually more complex due to the biarticular hip and knee rectus femoris and hamstrings musculature, which simultaneously generates hip and knee torque during squatting. Although increasing forward trunk tilt decreases the external knee flexor moment arm and torque, it simultaneously increases the external hip flexor moment arm and torque. To overcome this external hip flexor torque, a hip extensor muscle torque from the hip extensors (hamstrings, gluteus maximus) is needed, which must be even greater given that rectus femoris force simultaneously produces hip flexor muscle torque and knee extensor muscle torque. Given that hamstrings force simultaneously generates hip extension muscle torque and knee flexor muscle torque, greater hamstrings force and knee flexor muscle torque results in greater quadriceps force and knee extensor muscle torque being needed, and less hamstrings force and knee flexor muscle torque results in less quadriceps force and knee extensor muscle torque being needed.
One of the more interesting findings were the interactions between squat types and leg conditions, which demonstrated that patellofemoral joint loading was similar between the BOSU squat and floor squat when squatting on one leg, but significantly higher in the floor squat compared to the BOSU squat when squatting on two legs. Clinical applications are that early in the patellofemoral rehabilitation process when the goal is to minimize patellofemoral loading, two-legged squatting should precede one-legged squatting, and the BOSU squat should precede the floor squat. Subsequently, when the patient is able to sustain greater patellofemoral loading, one-legged squatting should be employed over two-legged squatting, and floor squatting should be employed over BOSU squatting. These findings may be due to differences in how the two squat type exercises were performed with varying amounts of stability. With one-legged squatting, one leg was on a stable surface (floor squat) or one leg was on an unstable surface (BOSU squat), while with two-legged squatting, both legs were either on a stable surface (floor squat) or on an unstable surface (BOSU squat). Regardless of what influenced these differences or similarities in patellofemoral loading between one-legged and two-legged squatting, these findings provide insight to how the patellofemoral joint can be loaded and progressed in PFP rehabilitation using one-legged and two-legged BOSU and floor squats.
Escamilla et al.6 also quantified patellofemoral force and stress during the two-legged bodyweight squat, while their participants performed the ball and wall squats with their back against a swiss ball or against the wall. The ball and wall squats in that study were performed with the trunk in a vertical position instead of tilted forward 30° - 50° as in the current study, which is a functional squat position. Escamilla et al.6 reported a peak patellofemoral force and stress of 1223±348 N and 3.05±0.87 MPa, respectively, during the ball squat and 1385±393 N and 3.45±0.98 MPa, respectively, during the wall squat, at 80° knee angle during squat ascent. In contrast, peak patellofemoral force and stress in the current study were 970±264 N and 2.42±0.66 MPa, respectively, during the two-legged BOSU squat, and 1125±353 N and 2.80±0.88 MPa, respectively, during the two legged floor squat (18-22% less compared to the two-legged bodyweight ball and wall squats), also occurring at the 80° knee angle during squat ascent. Average patellofemoral force and stress throughout the squat descent (10° - 100°) and squat ascent (100° - 0°) was also 22% less in the BOSU squat compared to the ball squat, but was nearly identical between the wall squat, ball squat and floor squat. Thus, when the goal is to minimize patellofemoral force and stress and gradually progress patellofemoral loading, the BOSU squat should be performed first, followed by the floor squat, ball squat, and finally wall squat, which had the highest peak patellofemoral force and stress.
Kernozek et al.9 also examined the two-legged bodyweight squat using two techniques - one squatting involving the knees progressing past toes (SPT) and one squatting with knees positioned behind toes (SBT). These authors reported mean patellofemoral force and stress of approximately 1450 N and 3.4 MPa, respectively, for SBT, and approximately 1950 N and 4.2 MPa, respectively, for SPT, which were slightly greater than the force and stress values than those in the current study. Wallace et al.10 reported peak patellofemoral joint force and stress magnitudes of approximately 1700 N and 9.3 MPa, respectively, during the bodyweight squat at 90° knee angle. Almonroeder et al.7 reported a mean patellofemoral joint force and stress magnitudes of approximately 2300 N and 11 MPa, respectively, during the bodyweight squat. Patellofemoral force and stress magnitudes from both Wallace et al.10 and Almonroeder et al.7 are considerably higher than those reported in the current study, which may be due to methodological differences among studies.
The results from the current study can be compared to patellofemoral joint loading during squatting with greater intensities to help clinicians progress a patient with PFP. Escamilla et al.2,3,8 reported peak patellofemoral joint force and stress magnitudes of 4500-4700 N and 11-12 MPa, respectively, at 90° knee angle during the 12 RM barbell squat, which is 4-5 times greater than peak magnitudes in the current study. Escamilla et al.4 also reported peak patellofemoral joint force and stress magnitudes of approximately 3500 N and 9 MPa, respectively, between 70°-80° knee angle during the 12 RM one leg squat and wall squat, 3-4 times greater than peak magnitudes in the current study. Wallace et al.10 reported peak patellofemoral joint force and stress magnitudes of approximately 2400 N and 13 MPa, respectively, during the barbell squat with a 35% bodyweight external load, a little over twice the force magnitudes and five times the stress magnitudes from the current study.
When considering patellofemoral loading from the aforementioned and current studies, squatting exercises during PFP rehabilitation can be progressed from lower to higher loads by initially performing two-legged and BOSU bodyweight squat exercises, then one-legged and floor bodyweight squat exercises, then lower intensity barbell squats (eg, 1/3 bodyweight external load), then higher intensity ball or wall squat (e.g., 12 RM external load), and then higher intensity barbell squats (e.g., 12 RM external load).
Peak patellofemoral joint force and stress magnitudes from the current study are similar, lower, or higher compared to many functional activities. Peak patellofemoral joint force and stress in healthy participants performing fast walking are approximately 900 N and 3.13 MPa, respectively,14 similar to peak magnitudes in the current study. Peak patellofemoral joint force and stress magnitudes in healthy participants ascending and descending stairs are approximately 2500 N and 7 MPa, respectively,14 2-3 times the peak magnitudes in the current study. Based on these findings, when the goal is to minimize and later progress patellofemoral loading, the order of progression when integrating functional activities with one-legged and two-legged squatting could be to start with slow walking, progress to fast walking, progress to two-legged BOSU squat followed by two-legged floor squat, progress to one-legged BOSUs-ball and floor squats, and finally progress to ascending and descending stairs.
The injury risk to the patellofemoral joint may not increase with knee angles between 70°-100° or greater because of similar magnitudes seen in patellofemoral joint stress during these knee angles. The benefits of exercising in deeper knee flexion angles include greater quadriceps, hamstrings, and gluteus maximus activity during training at 70°-100° knee angles or greater when compared to training at lesser knee angles between 0° - 60°. Exercising in smaller knee flexion angles between 0° - 60° becomes more quadriceps dominant with less hamstring and gluteus maximus involvement.3,4,8
All biomechanical models have modeling limitations (see Appendix for an overview of biomechanical model employed, and its potential limitations). Firstly, knee kinematic MRI data have shown that during the weight bearing squat the femur moves and rotates under a relatively stationary patella, and excessive femoral rotation may increase patellofemoral joint stress on the contralateral patellar facets.15 Unfortunately, knee kinematic MRI data do not currently exist for BOSU and floor squat exercises through functional ranges of motion. Therefore, it is unknown how much the femur rotates and how this rotation varies among healthy individuals when compared to those with pathologies. Secondly, patellofemoral joint stress magnitudes were calculated employing patellar contact area values from MRI data in the literature and were not measured directly for each subject. However, the contact areas employed from the literature were determined while performing loaded weight bearing exercise in healthy female and male participants, similar to the current study. Moreover, the near linear and direct relationship between knee angle and contact area has been shown to be similar among studies.12,16,17 Therefore, it is a fair assumption that patellofemoral joint stress curve patterns in Figures 3a and 3b using contact areas from the literature are similar to patellofemoral joint stress curve patterns for contact areas measured directly from MRI. Patellofemoral joint stress patterns are important for clinicians to understand to help determine what knee range of motions patellofemoral joint stress increases or decreases, which can exacerbate PFP. Finally, the focus of the current study was to compare right knee patellofemoral force/stress between the BOSU squat and floor squat, so the authors arbitrarily chose the right leg to use in the knee model to assess this using only one force platform. The focus was not to compare patellofemoral force/stress between left and right knees and assess symmetry between left and right sides of the body during two-legged squatting, although symmetry was assumed in these healthy subjects.
CONCLUSIONS
Patellofemoral joint loading changed according to variations in both squat type and leg variations. Squatting progression employing lower to higher patellofemoral loading over time during PFP rehabilitation may be considered: 1) two-legged BOSU squats at lower knee angles (0° - 50°); 2) two-legged floor squats at lower knee angles (0° - 50°); 3) one-legged BOSU and floor squats at lower knee angles (0° - 50°); 4) two-legged BOSU squats at lower and higher knee angles (0° - 100°); 5) two-legged floor squats at lower and higher knee angles (0° - 100°); 6) one-legged BOSU and floor squats at lower and higher knee angles (0° - 100°). Future research could focus on examining using external loads on patellofemoral force and stress while performing similar squatting exercises, and investigating the clinical relevance of performing these exercises in patients with PFP.