INTRODUCTION
Partial weightbearing (PWB) is an integral rehabilitation instruction following lower limb surgery or conservative fracture management, serving to stimulate bone healing and avoid complications such as thrombosis, muscle atrophy, and inactivity-induced osteoporosis.1 PWB may also be a treatment option for soft tissue injuries. While biofeedback devices have been available for many years, the standard of care for teaching PWB relies on using a bathroom scale, a method that only measures force in a stationary stance and not during the dynamic act of walking.2,3 This limitation poses a challenge for all patients, irrespective of age, as the inability to apply the correct force during ambulation may result in structural failure of osteosynthesis or secondary dislocation of conservatively treated fractures, potentially compromising recovery outcomes.4 Therefore, adherence to weightbearing restrictions is crucial for all patients to mitigate the risk of such failures.
While the bathroom scale method provides limited feedback during stationary training, real-time biofeedback offers continuous information about the actual load throughout the entire training process. Since maintaining weight-bearing limitations becomes more challenging during movement, biofeedback enhances monitoring and helps participants develop greater awareness of weight applied to the affected leg. PWB aims to navigate the balance between protecting the surgical site, soft tissue or conservatively treated fracture and promoting bone growth.5,6 Weightbearing is deliberately restricted to prevent implant failure from excessive load, which can cause deformation or breakage of the implant, with the greatest risk arising from repetitive loading beyond a tolerance threshold. Conversely, controlled weightbearing encourages osteoblastic activity, essential for bone repair.7 In clinical practice, definitions of weightbearing levels vary, with some institutions defining specific poundage for touch-down and partial weightbearing, while others use a percentage of the patient’s body weight.1 Despite clinical research into biofeedback devices for PWB, there remains a lack of studies focusing exclusively on the training method itself, particularly using healthy subjects to eliminate confounding factors like varying fracture types. This study aims to fill that gap by comparing traditional SOC training methods to a biofeedback device in a healthy, young adult cohort. This approach is innovative in its exclusive focus on the training modality, setting aside the potential influences of different injury profiles. Furthermore, this study compares training protocols, including one utilizing audio-visual biofeedback, that can be seamlessly integrated into day-to-day physical therapy with only minor investments. These protocols require no significant changes to current practices, making them practical and accessible for widespread adoption. Additionally, the study investigates the usability and user experience of the biofeedback device, providing valuable insights into its practicality and acceptance in clinical settings.
The primary objective of this study was to compare SOC training in PWB with a biofeedback device (insole). Secondary objectives included assessing participant satisfaction with the biofeedback device and evaluating its usability.
METHODS
Trial Design
This study was conducted as a randomized controlled trial, adhering to the principles outlined in the CONSORT Checklist. Approval was obtained by the institutional review board (IRB).
Participants
Eligible participants were between 18 and 60 years old, healthy, able to walk unassisted, free from cognitive impairments, and willing to participate in the study. The primary inclusion criterion was the ability to use crutches. Those unwilling to participate or with sensor incompatibility were excluded.
Interventions
During the study, all participants were equipped with force-measuring insoles (Loadsol®, novel electronics inc., Pittsburgh, PA-15237, USA) fitted into both shoes. Participants were randomly assigned to one of two groups: a cohort utilizing the biofeedback function of the Loadsol® device during partial weight-bearing (PWB) training (training only, not during the assessment) and a control group engaging in standard care training without the biofeedback activated.
The Loadsol® device is a mobile, in-shoe sensor system that measures plantar forces during both static and dynamic activities. It provides real-time auditory and visual feedback, designed to enhance training by facilitating quicker learning and promoting adherence to weight-bearing restrictions. The system has been validated in multiple studies, demonstrating accuracy comparable to traditional force plates and utility in clinical settings, including monitoring load-bearing compliance and improving rehabilitation outcomes.8 The weight-bearing limit was set to 20 kg, as 15–20 kg is a common restriction recommended in the AO guidelines for various lower limb injuries.9,10
Standard of Care (SOC) Group
A comprehensive training and assessment protocol was developed and approved by a group of board-certified physical therapists, orthopedic surgeons, and research staff (Appendix 1). This standardized regimen, thoroughly documented and video-recorded, began with foundational instructions on crutch-assisted ambulation and the importance of adhering to weightbearing limitations. Participants practiced on a bathroom scale to gain proficiency in maintaining prescribed weight limits, interspersed with walking exercises and verbal guidance, repeating this cycle at least three times to ensure confidence in compliance.
Although various methods for partial weight-bearing (PWB) training exist, such as verbal instructions, the hand-under-foot method, and the use of a bathroom scale, the standard of care (SoC) in this study was defined as the bathroom scale method. This choice was based on its status as the standard practice at the university hospital where the study was conducted, as well as evidence from the literature suggesting that the bathroom scale method is either superior to or at least as effective as the other two methods.11,12
Biofeedback (BF) Group
Participants in the biofeedback group received auditory alerts from the BF device (Loadsol®) when exceeding weightbearing thresholds, along with visual feedback on an iPad during stationary exercises. This group underwent the same training sequences as the SOC group, with the added biofeedback component.
Both groups continued their training until participants self-reported their readiness to observe PWB (using crutches) independently. Following this, the biofeedback system was deactivated, and participants were required to complete a standardized mobility course, which included activities ranging from sitting to walking a set distance, returning and climbing as well as descending five stairs (assessment). Gait data collected during this assessment phase were immediately analyzed by certified research staff for compliance with the weightbearing restrictions. Training success was defined as adherence to these restrictions, specifically not exceeding the weightbearing limit (20 kg) by more than 50% (maximum load of 30 kg) throughout the assessment phase. If compliance was achieved, training was suspended. In cases where compliance was not met, participants received a detailed report based on the data collected during the assessment, and the entire process was then repeated. After completing the second assessment, training was suspended regardless of whether the participant complied with the weightbearing restrictions.
After completing the study, participants filled out a questionnaire to provide feedback on their training experience.
Primary Outcomes
The primary objective of the study was to evaluate compliance with weightbearing restrictions, specifically not to exceed 150% of a predetermined limit of 20 kg. Measurement of compliance involved various parameters, including maximum and average load borne by participants, the rate at which this load was applied, and the number of steps taken, all monitored using the insole force sensors. Additionally, participant walking speed (time required to cover a distance of 5 meters) and the total duration needed to complete the training program were measured.
Secondary Outcomes
Secondary outcomes focused on participant satisfaction and the usability of the training protocol. These were quantified through a structured questionnaire, providing insight into the participants’ perceptions and the functional application of the training methods. (Appendix 2)
Sample Size
For the SOC group, the estimated training time was 15 minutes with a standard deviation (SD) of 5 minutes. In the BF group, the estimated training duration was 12 minutes (SD = 5 minutes). To determine the necessary sample size, a power analysis was performed. Targeting a power of 0.9 at an alpha level of 0.05, the analysis indicated that a sample size of 59. Consequently, the sample size was set to 60 participants to ensure the study had sufficient statistical power.
Randomization
Randomization was executed via computer in Redcap by the enrolling research staff, with a 1:1 ratio to one of the two groups. The “affected” leg (left or right) was also randomized in a 1:1 ratio.
Statistical Methods
The study employed descriptive statistics, inferential statistics, and regression analyses. Descriptive statistics included calculating means, standard deviations, and frequencies for demographic and outcome variables. For inferential statistics, t-tests and non-parametric equivalents (e.g., Mann-Whitney U test) were used to compare the primary outcome between groups. ANOVA or Kruskal-Wallis tests were employed for comparing secondary outcomes, like compliance overload percentages. Data normality was assessed, and appropriate transformations were applied as needed. Cohen’s d was calculated to determine the effect sizes.
RESULTS
Demographics
In this study, a total of 60 patients participated, with 33 assigned to the Biofeedback (BF) group and 27 to the Standard of Care (SOC) group. The study included 32 male and 28 female participants, aged between 18 and 47 years (Table 1). The mean age was 26.48 years (SD = 5.65). All participants randomized into the study were retained for analysis.
Gait analysis
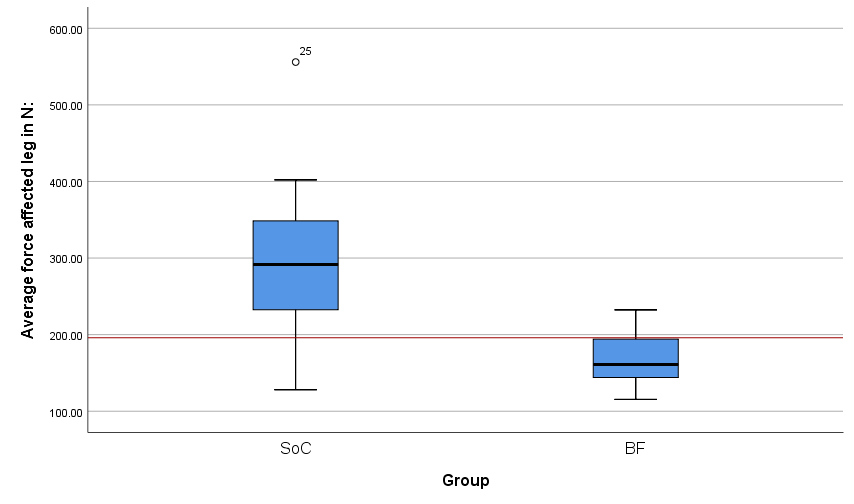
A force limit of 20 kg (equivalent to 196 Newtons) was uniformly set for all participants. Throughout the training and assessment sessions, gait data were continuously collected using Loadsol force-measuring insoles. A significant disparity was observed in the peak and average forces applied between the two groups. Participants in the BF group exhibited a peak force of 330 Newtons, whereas those in the SOC group reached up to 600 Newtons, surpassing the allowed weight by more than threefold (p ≤ 0.001). The average peak force across all steps was 167 Newtons for the BF group and 296 Newtons for the SOC group (p ≤ 0.001).
Post-training assessment during a standardized mobility course showed a reduction in peak forces to 220 Newtons for the BF group and 459 Newtons for the SOC group (p ≤ 0.001), with average peak forces recorded at 125 Newtons (BF) and 289 Newtons (SOC). Notably, there were no significant differences in the peak forces exerted by the healthy leg (p = 0.453; BF: 916 N vs. SOC: 878 N) or in gait speed (p = 0.369; BF: 2.40 km/h vs. SOC: 2.30 km/h). Average peak forces of the affected leg during the first assessment (standardized mobility course) for each group are depicted in Figure 1.

Compliance with weightbearing restrictions, defined as not exceeding 150% of the set weight limit in peak force during the assessment (30 kg or 294.3 Newtons), varied markedly between groups. A substantial 88% (29 out of 33) of participants in the BF group adhered to this criterion, compared to only 19% (5 out of 27) in the SOC group, as determined by Fisher’s exact test (p ≤ 0.001).
Participants who did not comply with the weightbearing restrictions during the initial assessment were provided with a detailed analysis of the gait data collected from the assessment. Following this, they underwent a repeat of the training and assessment protocol. In the second assessment, compliance with weightbearing restrictions improved markedly. All participants in the BF group adhered to the set restrictions, while 59% of the SOC group achieved compliance (p ≤ 0.001). Despite this improvement, 33% (9 out of 27) of the SOC group participants still failed to meet the compliance criteria after two rounds of training.
Regarding total training duration, there was a significant difference between the two groups. On average, participants in the BF group required 9 minutes and 00 seconds (± 3 minutes and 06 seconds) of training. In contrast, participants in the SOC group required a longer duration of 12 minutes and 49 seconds (± 3 minutes and 01 second) to complete their training (p ≤ 0.001).
Large effect of real-time audio-visual biofeedback compared to the bathroom scale (SoC) was found for average (Cohen´s d = 1.82) and maximum peak force (Cohen´s d = 1.89) as well as training time (Cohen´s d = 1.24).13
Participant satisfaction and usability
In the study’s questionnaire, participants rated their agreement with various statements on a scale from 1 (strongly disagree) to 5 (strongly agree). Although participants in the BF group tended to give slightly higher ratings for statements such as “learning PWB was easy” (BF: 4.15 ± 0.87 vs. SOC: 3.74 ± 0.98; p = 0.163) and “I would recommend this training method” (BF: 4.52 ± 0.62 vs. SOC: 4.26 ± 1.02; p = 0.238), these differences were not statistically significant. The usability of the Biofeedback device was rated as almost perfect. Detailed results from selected questions of this survey are presented in Table 2.
DISCUSSION
The current study demonstrates that real-time audio-visual biofeedback significantly enhances compliance with weightbearing restrictions and reduces the training duration required for healthy participants. Additionally, the BF device was found to be user-friendly and easily comprehensible for participants.
A notable finding was the SOC training’s inability to achieve satisfactory levels of compliance. Notably, none of the 27 healthy participants in the SOC group could maintain the peak load below 30 kg (150% of the weightbearing limit) during training. The average peak load during SOC training was 600 Newtons, three times higher than the set limit of 196 Newtons. Furthermore, the average peak load across all steps in this group was 296 Newtons, indicating a consistent overloading of the affected limb. In some cases, this overloading was even more pronounced, with over 20% (6/27) of SOC participants reaching an average peak load exceeding 40 kg during the assessment. This indicates a repeated and excessive overload on the ‘affected’ limb.
These outcomes challenge the efficacy of using a bathroom scale as a sole tool for acquiring a sense of 20 kg PWB. The primary issue appears to be the stationary nature of this training approach, contrasting with the need to maintain limits during dynamic movement. Most patients in both groups could replicate 20 kg while standing after brief training. However, insole data revealed significantly higher loads during actual gait, even though it felt similar to the participants. Therefore, based on our findings, real-time audio-visual biofeedback emerges as an effective tool for teaching weightbearing limits in dynamic scenarios, thereby enabling safer and more efficient training in PWB. These results are consistent with existing literature.3
Considering the widespread application of SOC training in instructing real patients with fractures post-osteosynthesis our results would suggest a high failure rate of the osteosynthesis itself. Intriguingly, the failure rates reported in actual patients and documented in the literature are significantly lower, presenting a contrast to our study’s results.14,15 This discrepancy prompts two potential explanations.
One hypothesis is that osteosynthetic implants may possess a greater load-bearing capacity than typically expected by surgeons. This resilience could account for the lower failure rates observed in clinical practice compared to the laboratory setting of our research.
Alternatively, patients with genuine fractures might inherently comply more effectively with PWB restrictions, driven by pain from the fracture and the fear of causing a refracture. This natural cautiousness could lead to a more stringent adherence to weight-bearing limits especially in the early post-surgery phase, thus reducing the likelihood of osteosynthesis failure.
While numerous studies have demonstrated that many patients fail to comply with weightbearing restrictions, and conventional methods such as “hand-under-foot”, “bathroom scale”, and “verbal instructions” are often ineffective in accurately replicating a specific weight limit, these methods continue to be employed as the Standard of Care for most patients.1,12,16,17 However, complication rates in these studies did not differ significantly from other research not focusing on weightbearing restrictions, suggesting that non-compliance does not necessarily lead to increased rates of osteosynthesis failure.17
Further evidence suggesting that osteosynthesis may be more robust than previously thought is seen in the growing trend towards early weightbearing. Several studies have highlighted the benefits of early weightbearing following various lower limb fractures, notably in decreasing return-to-work or activity times without a significant rise in complication rates.18–20
However, randomized controlled trials (RCTs) advocating for early weightbearing are specific to each fracture type and treatment modality. These RCTs are necessary to safely generalize the application of early weightbearing to patients. Given that osteosynthesis failure remains a common complication in orthopedic surgery, it is unlikely that immediate weightbearing will be universally recommended for all fractures at any time. Consequently, PWB remains an essential aspect of post-fracture care for lower limb injuries.
Our study underscores the importance of effective PWB training. We have shown that live audio-visual biofeedback significantly improves compliance rates, reduces the training duration, and is easily integrated into routine physical therapy practices. These findings highlight the need for more efficient training methods in PWB to ensure patient safety and better treatment outcomes.
Potential limitations of the study include the unique characteristics of the healthy participant group. These individuals, unlike actual patients, do not experience pain or the fear of exacerbating an injury, which might lead to a diminished focus on adhering to weightbearing limits. Additionally, the demographic profile of our study group, being predominantly young and healthy, does not fully represent the general population. It is conceivable that elderly, obese, or severely ill patients may exhibit different outcomes when subjected to either of the training methods explored in our study. Another limitation may be the reliance on a uniform force standard (20 kg) rather than individualizing it as a percentage of body weight. This may have affected participants’ ability to meet the task requirements, as the relative effort needed to achieve the target weight-bearing limit varies based on individual body weight. Nonetheless, this should not have influenced the study results, as body weight was nearly identical across the groups.
However, the strength of our study lies in its randomized design and the implementation of a highly standardized training protocol. These elements enable an accurate comparison of different training methods. The utilization of healthy participants eliminates confounding factors such as varying fracture types, quality of reduction, and osteosynthesis. Moreover, the sample size in our study surpasses that of most comparable research, yielding results that are not only statistically significant but also broadly applicable.
CONCLUSION
This study demonstrates the inadequacy of bathroom scales for reliable training in PWB. Such traditional tools lack precision in monitoring and enforcing weightbearing limits. Conversely, biofeedback devices, exemplified by Loadsol® force sensors, have significantly enhanced compliance with weightbearing restrictions. They have also been instrumental in reducing the training duration required for patients. Additionally, their integration into routine physical therapy is both feasible and practical.
Based on these findings, it is recommended to incorporate real-time audio-visual biofeedback mechanisms in PWB training protocols. This incorporation not only aligns with the goal of precise weightbearing management but also optimizes the efficiency of rehabilitation processes post-injury or surgery.
Competing interests
The authors report no conflicts of interest.
Acknowledgements
We thank Morgan Dauk and Darek Keeney for their support in administering this study.