INTRODUCTION
One of the primary goals of early rehabilitation after anterior cruciate ligament reconstruction (ACLr) is to normalize gait. Although the resolution of observable gait deviations is expected by 12 weeks of surgery,1–3 biomechanical analyses describe altered sagittal plane knee mechanics that persist well past this time point.4–13 The hallmark of these deficits is reduced extensor moment and power absorption in the surgical knee during loading response phase of gait.4 Knee extensor deficits as large as 35% and 29% have been reported during gait at 3-5 months,5,6 and 4-6 months6,7 post-ACLr, respectively. These deficits are observed along with decreased knee power, knee flexion excursion, and vertical and posterior ground reaction forces (GRFs).4,5 Longitudinal work suggest that these extensor moment deficits persist long term.6–10,14 Those observed at six months persist with clinically meaningful deficits at one and two years post-surgery.7,9,14,15 Restoration of sagittal plane knee mechanics in early recovery is critical as their long-term persistence is attributed, in part, to the progression of knee osteoarthritis.16–19
The chronic nature of knee loading impairments during gait suggests that traditional rehabilitation is not sufficient. Outside of describing clinical expectations for restoration of gait, current clinical recommendations provide little guidance for specific interventions. The absence of gait specific training recommendations assumes that gait deficits will recover spontaneously. However, traditional rehabilitation does not guarantee recovery of knee mechanics during gait. This is highlighted in the results from a clinical trial that found rehabilitation plus additional balance training improved performance of clinical hop tests and patient reported outcomes without restoration of gait mechanics.9,10,14 These findings underscore the need for gait specific interventions.
Treadmill gait training can provide a steady-state stimulus and is generally accessible to patients in rehabilitation settings. In non-injured healthy individuals increasing gait speed has been found to increase knee extensor moments,20,21 knee flexion excursion,21,22 and GRFs.21 Treadmill gait training at increased gait speeds may provide a controlled stimulus for improving knee loading deficits. Previous work assessing the effects of gait speed on limb and knee mechanics in individuals following ACLr has largely focused on individuals greater than six months post-surgery.23,24 While one study found that increases in treadmill speed in individuals less than three months post-surgery resulted in greater between limb GRFs asymmetries, the effect of treadmill gait speed on knee mechanics was not explored.25 Moreover, the application of the experimental protocol to clinical prescription is not clear as the self-selected gait speed determined from overground walking was used for treadmill testing. Clinically, determination of an individual’s comfortable gait speed should done be on the treadmill as individuals in early recovery may be less comfortable on a treadmill, electing for a slower speed. Currently, it is not known how increased speed influences GRFs and more importantly sagittal plane knee loading variables in individuals four months post-ACLr, a time point where gait is expected to normalize and progression to more demanding tasks takes place.
Understanding how treadmill gait speeds influences knee extensor moment, power absorption, and related kinematics and kinetics in this population will inform interventions aimed at improving gait mechanics in early recovery. Therefore, the purpose of this study was to determine how individuals four months post-ACLr respond to the demands of increased speed during treadmill gait. It was hypothesized that increasing speed from self-select to speeds 25% and 50% greater will increase knee extensor moments and power, knee flexion excursion, and vertical and posterior GRFs systemically in individuals 12-20 weeks post-ACLr and non-injured controls. It was also hypothesized that the steady state, symmetrical stimulus provided by the treadmill will improve between limb symmetry in individuals who present with knee extensor moment asymmetry in overground gait.
METHODS
A cross-sectional design was used to compare the response to increasing gait speed demands in individuals post-ACLr and non-injured controls.
Participants
Participants were recruited from a university campus and local physical therapy clinics for control and ACLr groups. To be included in the ACLr group participants had to be 12-20 weeks post-ACLr and demonstrate knee extensor loading deficits during overground gait defined as decreased surgical knee extensor moment of 15% asymmetry or higher. Surgeon, surgery type or treating physical therapist were not controlled for; however, all therapists followed standard rehabilitation protocols that emphasized early restoration of range of motion and progression off crutches when patients demonstrated gait without observable deviations. Participants were excluded if they had concurrent knee pathology that limited their weight-bearing status after surgery. Healthy non-injured participants were recruited for the control group; they were excluded if they had a history of lower extremity surgery or injury or were unable to perform the study tasks.
A priori sample size analyses on primary variables of interest (knee extensor moment and power, and knee extensor moment and power symmetry) from four individuals in each group (ACLr and Control) determine that a minimum sample size of 8 per group was needed to detect an interaction between group and speed with a power of 0.80 and alpha level of 0.05.
Procedures
Prior to testing, all procedures were explained to each participant, and informed consent was obtained as approved by the Institute Review Board of the University of Southern California Health Sciences Campus. To characterize recovery status, participants completed the Knee injury and Osteoarthritis Outcome Score (KOOS)26,27 and underwent knee extensor strength testing. Isometric knee extensor strength was assessed at 60 degrees knee flexion bilaterally (HUMAC2009 dynamometer; CSMi Inc., Stoughton, MA, USA). The maximum torque of four trials was used for analysis. A strength limb symmetry index was calculated as surgical (or right control) / non-surgical (or left control) *100.
Gait assessments took place in the Musculoskeletal Biomechanics Research and Locomotor Control Laboratories in the Division of Biokinesiology and Physical Therapy at the University of Southern California (Los Angeles, CA). Kinematic data (43 reflective markers) were collected using a 10-camera motion-capture system at 100 Hz (Qualisys AB, Gothenburg, Sweden). Reflective markers (14-mm spheres) were placed on the following anatomical landmarks to define body segments: the L5-S1 junction, and bilaterally on the end of second toes, first and fifth metatarsal heads, medial and lateral malleoli, medial and lateral epicondyles of femurs, greater trochanters, posterior superior iliac spines, and iliac crests. Tracking marker clusters mounted on semi-rigid plastic plates were secured to the thighs, shanks, and heel plates of shoes, bilaterally. A static calibration trial was collected with all markers attached. Tracking marker clusters, as well as markers on the end of the second toe, iliac crests, posterior superior iliac spines, and the L5-S1 junction, remained on the participant throughout the entire testing, while other markers were removed after the static calibration trial. Ground reaction forces were obtained using two force platforms at 1000 Hz (AMTI®, Newton, MA, USA) embedded into the floor surface (overground gait; to determine inclusion criteria) or underneath the treadmill (Instrumented Treadmill, Bertec Corporation, Columbus, OH, USA). Kinematic and kinetic data were collected synchronously (Qualisys Track Manager Version 2.17).
During treadmill gait, participants wore a harness designed to prevent falls while providing no body weight support. Self-selected (SS) speed was determined via stair-case method.28 Briefly, treadmill speed started at 1 m/s and maintained for 30 seconds, speed was adjusted in increments of 0.1 m/s in a series of faster and slower speeds; maintaining each speed for 30 seconds before asking the participant if it felt faster or slower than their comfortable everyday speed. This was repeated until they indicated that the treadmill speed felt like their comfortable speed. This process took between 5-10 minutes and allowed for familiarization with treadmill walking. Testing speeds were based on the SS treadmill speed, two faster speed conditions were calculated as 25% faster (SS25) and 50% faster (SS50) than SS speed. Next, data were collected with participants walking at each speed (SS, SS25, SS50) for 3 minutes. The two faster speed conditions were tested in random order. To allow for accommodation to changes in speed, data were analyzed within the last 30 seconds of the 3-minute trials.
Data Analyses
Marker coordinate data were labeled and digitized (Qualisys Track Manager Version 2.17) and lower extremity kinematics and net joint moments were calculated (Visual3D: C-Motion, Inc, Germantown, MD). Coordinate and GRF data were filtered using a fourth-order, zero-lag, 6Hz Butterworth low-pass filter. Joint kinematics were calculated using joint coordinate system approach.29 Body mass, kinematics, and GRFs were used to calculate sagittal plane net joint moments at the knee using standard inverse dynamics equations.30 Moments reported as internal moments, were normalized to body mass (Nm/kg). Knee power was calculated as the scalar product of joint angular velocity and sagittal plane net joint moment.
Dependent variables were identified from 0-30% of stance capturing loading response of gait. Initial contact was determined using a 20N vertical ground reaction force threshold. Dependent variables were identified during loading response in both limbs in the ACLr and control groups: peak knee extensor moment, peak knee power absorption, peak vertical GRF (vGRF), peak posterior GRF (pGRF), and knee flexion excursion. Knee flexion excursion was calculated from initial contact to the subsequent knee flexion peak. All dependent variables were identified using a customized MATLAB program (version 2017a, the MathWorks, Inc., Natick, MA). The average of 6 consecutive steps for each limb was used for analysis.
To characterize deficits in the surgical knee, between limb symmetry was defined using a limb symmetry index (LSI) using the following equation: ratio = surgical / non-surgical, LSI less than 1 indicates surgical is smaller than non-surgical limb. For the control group, the limb with the smaller knee extensor moment during gait at SS speed was considered “surgical limb”, while the other limb was considered “non-surgical limb”. LSI was calculated for peak knee extensor moment, knee power absorption, vGRFs, and pGRFs. For knee flexion excursion, between limb differences were used to characterize symmetry in both groups, where a negative value indicates that the surgical/matched limb is smaller than the non-surgical limb.
Statistical Analysis
Data are expressed as mean ± standard deviation (Supplementary tables 1&2). Independent samples t-tests determined differences between groups in descriptive data including anthropometrics, self-reported function and strength (Table 1). Effects of speed and group on knee mechanics, peak knee extensor moment, peak knee power absorption, peak vGRF, peak pGRF, and knee flexion excursion from the surgical limb (ACLr group) and control limb (average of right and left limbs) were determine with separate two-way mixed-ANOVAs [speed (SS vs. SS25 vs. SS50) X group (ACLr vs. control)]. In case of group x limb interactions, main effect analyses were performed to determine between and within group differences. Effects of speed and group on LSI for knee extensor moment, knee power absorption, vGRFs, and pGRFs, and between limb differences in knee excursion were determined using separate two-way mixed-ANOVAs [speed (SS vs. SS25 vs. SS50) X group (ACLr vs. control)]. Pearson’s product-moment correlation was used to examine the relationship between isometric knee extensor strength ratio and knee extensor moment ratio in all three gait speed conditions. Analyses were performed using SPSS statistical software (Chicago, IL, v.25); α<0.05.
RESULTS
Participants
Twenty-four individuals performed overground gait trials (n=11, ACLr; n=13, control). One participant was excluded (ACLr group) because they did not meet the inclusion criteria of 15% knee extensor moment deficits during overground gait. Knee extensor moment LSI in one control participant was excluded as an outlier falling outside the interquartile range and variability whiskers of the boxplot for control data.
Subject characteristics (mean ± SD) are reported in Table 1. Twelve individuals (sex: 5 females, 7 males) were included in the control group, ten individuals (sex: 6 females, 4 males) 109.2 ± 19.9 days post-surgery were included in the ACLr group; surgery type and surgeon varied. Concurrent injuries, that did not require weightbearing restrictions, were reported in five participants. One participant reported previous ACLr to the contralateral knee at least one year prior to re-injury and had returned to pre-surgical level of physical activity. One individual in the ACLr group did not perform the knee extensor strength assessment.
Effects of Speed on Lower Extremity Mechanics
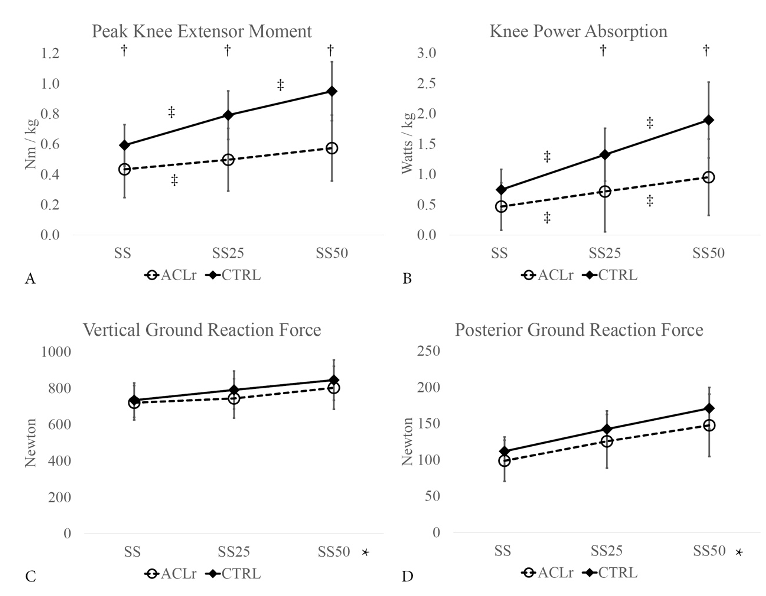
Significant group x speed interactions were observed for knee extensor moment (Figure 1a; p<0.001) and power absorption (Figure 1b; p<0.001). Post-hoc tests revealed that knee extensor moment was smaller in the surgical compared to the control limb at each speed (p=0.032 SS, p=0.001 SS25, p<0.001 SS50). Power absorption was not different at SS but was smaller in the surgical compared to the control limb at SS25 (p=0.018) and SS50 (p=0.002). Knee extensor moment increased between SS and SS25 for both groups (p=0.037 ACLr; p<0.001 control) and between SS25 and SS50 in the control group only (p<0.001 control). Power absorption increased between SS and SS25 (p=0.030 ACLr; p<0.001 control) and between SS25 and SS50 (p=0.039 ACLr; p<0.001 control) for both groups.
Main effects of speed (p<0.001) and group (p<0.001) were observed for knee flexion excursion. Regardless of group, excursion increased between SS and SS25 only (mean difference = 2.466 degrees, p<0.001). Regardless of speed, the ACLr group knee flexion excursion was smaller than the control group (mean difference = 5.118 degrees; p<0.001).
Only a main effect of speed was observed for vertical (Figure 1c; p<0.001) and posterior (Figure 1d; p<0.001) GRFs. Regardless of group, vGRF and pGRF increased between SS and SS25 (mean difference = 39.890 N, p<0.001 vGRF; mean difference = 28.699 N, p<0.001 pGRF) and between SS25 and SS50 (mean difference = 56.705 N, p<0.001 vGRF; mean difference = 25.315 N, p<0.001 pGRF).
__25__faster_than_ss_speed_.png)
Effects of Speed on Between Limb Symmetry
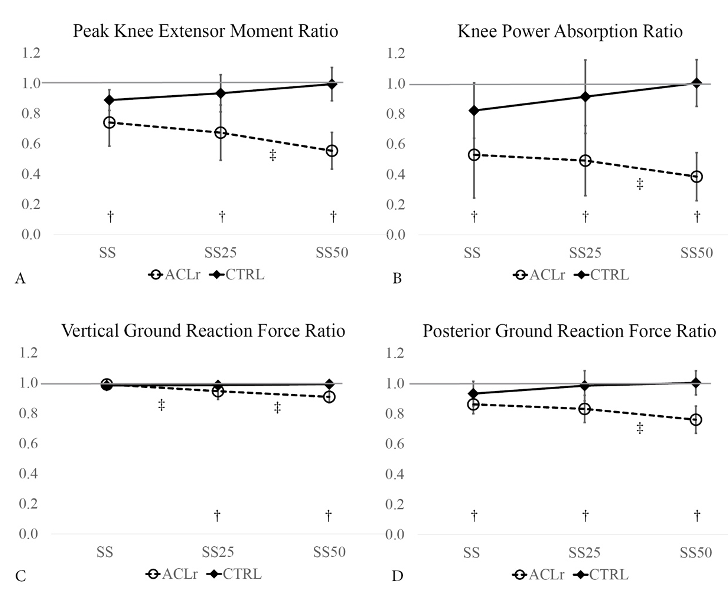
Significant group x speed interactions were observed for knee extensor moment (Figure 2a; p<0.001) and power absorption LSI (Figure 2b; p<0.001). Post hoc tests reveal that knee extensor moment LSI was smaller in the ACLr versus control group at each speed (p=0.008 SS, p=0.001 SS25, p<0.001 SS50). Knee extensor moment LSI did not change from SS to SS25 but decreased from SS25 to SS50 in the ACLr group (p=0.006). The control group did not differ across speeds. Knee power LSI was also smaller in the ACLr versus control group at each speed (p=0.009 SS, p<0.001 SS25, p<0.001 SS50). Knee power LSI did not change from SS to SS25 but decreased from SS25 to SS50 in the ACLr group only (p=0.017) with no differences observed across speeds for the control group.
Significant group x speed interaction was observed for between limb differences in knee excursion (p=0.021). Between limb differences in knee excursion were greater at each speed (5.3 degrees p<0.001 SS, 6.4 degrees p<0.001 SS25, 7.7 degrees p<0.001 SS50) in the ACLr versus control group.
Significant group x speed interactions were observed for vGRF (Figure 2c; p<0.001) and pGRF (Figure 2d; p<0.001) LSI. Post hoc testing revealed that compared to the control group, vGRF LSI was smaller in the ACLr group at SS25 (p=0.041) and SS50 (p<0.001) and pGRF LSI was smaller in the ACLr group at all speeds (p=0.036 SS, p=0.001 SS25, p<0.001 SS50). Within groups, vGRF LSI decreased from SS to SS25 (p=0.013) and from SS25 to SS50 (p=0.029) and pGRF decreased from SS25 to SS50 (p=0.041) in the ACLr group only.
__25__faster_than_ss_speed_(ss25)__and_5.png)
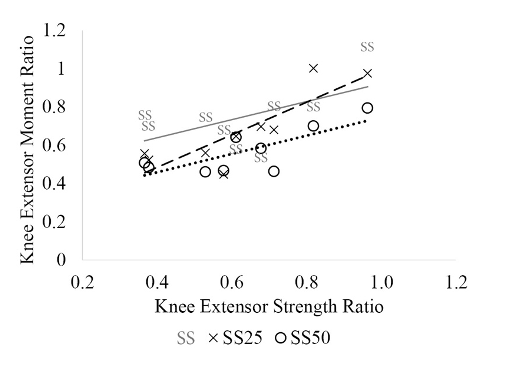
A statistically significant positive relationship was observed between isometric knee extensor strength ratio and knee extensor moment ratio during SS25 (r= 0.85, p= 0.002) and SS50 (r= 0.77, p= 0.008) conditions but not SS (r= 0.55, p= 0.060) in the ACLr group (Figure 3).

DISCUSSION
The chronic nature of altered sagittal plane knee loading mechanics during gait suggest that existing rehabilitation guidelines are not sufficiently addressing this issue. Retraining gait on the treadmill during early recovery by increasing gait speed provides implicit increases in gait specific knee demands. The authors found that individuals 12-20 weeks post-ACLr improved knee loading mechanics in response to the demands induced by a moderate increase in treadmill speed. However, when the treadmill speed and demand were higher, compensatory patterns emerged. These findings have implications for gait retraining interventions in early rehabilitation following ACLr.
Individuals following ACLr were able to increase GRFs in their surgical limb similar to controls when treadmill speed was increased 25% faster than their self-selected speed. This moderate increase in speed also resulted in significant increases in knee extensor moments and power (Figure 1). While greater increases in moment and power were observed in the control limb (34% and 77 %, respectively), individuals in the ACLr group increased moments and power on average 15 % and 53 %, respectively with negligible changes in between limb asymmetry (Figure 2). Only a small increase from 1% to 5% asymmetry in vGRF was observed in the ACLr group between SS and SS25. On average, knee moment and power symmetries remained the same between SS and SS25 conditions (Figure 2). When taken together, these data suggest that this moderate increase in treadmill gait speed may provide a stimulus to promote greater knee sagittal plane loading. However, these data do not support the hypothesis that the steady state, symmetrical stimulus of treadmill gait would improve between limb symmetry. When considering individual data, a varied response to SS25 was seen across participants with respect to knee extensor moment symmetry (Figure 3).
Differences emerged between groups in response to even greater increases in treadmill speed from SS25 to SS50 indicating that individuals post-ACLr had difficulty meeting the higher demands easily accommodated by the control participants (Figure 1). Despite similar increases in surgical and control limbs in vertical and posterior GRFs, no further improvements in knee extensor moment were observed in the ACLr group. This contrasted with a 20% increase in knee extensor moments in the control group. Knee power improved in the ACLr limb but to a smaller degree than for controls (33% versus 43%). In the ACLr group, between limb symmetry worsened for all variables from SS25 to SS50. Deficits of 33% and 51% in knee moment and power, respectively, at SS25 increased to 45% and 62% at SS50. Between limb vGRF and pGRF deficits worsened when speed increased from SS25 to SS50. Together these data appear to reflect a pattern of compensation with their non-surgical limb in the ACLr group at SS50 speed. Individual knee extensor moment symmetry data suggests a more consistent response across individuals when speed was increased 50% (Figure 3). Only two participants exhibited small increases in symmetry (less than 0.6). All other participants decreased their symmetry relative to the SS condition.
Average KOOS scores and knee extensor moment strength LSI indicate that the participants in the ACLr group were on a typical recovery path.31 In addition, it was not surprising that only one individual recruited for the study did not meet the inclusion criterion of a knee extensor moment deficit greater than 15% during overground walking given reports of larger deficits at this time post-surgery.5–7 On average, individuals in the ACLr group had 37% deficits in knee extensor muscle strength with deficits ranging from 4% to 63%. Strength asymmetries were positively related to knee extensor moment deficits; participants with greater knee extensor muscle weakness had larger knee moment asymmetries. This association did not reach significance at SS speed but it was strong at the two faster speeds SS25 and SS50. While an a prior sample size calculations indicated only eight participants per group were needed to detect interactions between groups and condition, this sample size did not allow for extensive exploration of associations among variables. Individual data and correlations across conditions are presented in Figure 3. Future studies should include larger samples and explore relationships between strength and the ability to respond to gait training interventions.
The current findings add to recent work investigating the effects of increased gait speed in individuals post-ACLr.23 Garcia and colleagues observed increasing asymmetries in GRFs with increased gait speed in individuals two months post-ACLr. Unlike the previous study, these participants had similar self-selected gait speed as healthy controls. To mimic how treadmill gait training would be prescribed in a clinical setting, the authors determined the individual’s comfortable self-selected speed on the treadmill. As a result, the self-selected treadmill speeds were slower than those reported in the previous study and more similar to their slower gait condition. The absence of changes in asymmetry across GRFs and knee loading variables from our self-selected condition and SS25 contrast the previous results suggesting that the current data may reflect additional recovery. An additional six weeks could represent a time of substantial progress towards improved gait mechanics. The current study provided specific information regarding knee loading in the surgical limb. Considering changes in both limbs reveal no changes in asymmetry but improved knee loading at only at SS25. While the introduction of conditions was randomized, it is possible that effects of fatigue or practice could have influenced subsequent performance in conditions. Similarly, it is not known how mechanics would change over a longer training period. There is the possibility that they would degrade over time due to fatigue or improve with practice. Furthermore, it is not known how increased demands translate to overground gait or to long-term improvements in mechanics.
CONCLUSION
In conclusion, the findings of this study suggest that moderate increases of gait speed may be an appropriate stimulus to improve knee loading mechanics 12-20 weeks following ACLr. Larger increases of gait speed should be exercised with caution to avoid use of compensatory strategies. Clinically, these data highlight the need for a progressive increase in demand to improve knee loading deficits to avoid the need for undesirable compensations. These data represent the average response of a small sample, further work with larger sample and consideration of patient specific recovery variables is needed to determine how treadmill training programs in early rehabilitation influence gait specific knee impairments.
Conflicts of interest
The authors declare no conflict of interest.