INTRODUCTION
Sport-related concussions (SRCs) are prevalent, with approximately 3.8 million occurring each year in the United States.1 Individuals who sustain SRCs experience cognitive and motor dysfunction acutely, with some such symptoms persisting beyond the acute phase.2–4 These sequelae, particularly neuromotor control deficits, can contribute to the increased risk of subsequent concussion and lower extremity injury which are observed among athletes following SRC.5–7 Currently there exists a need for validated clinical objective measures to assess residual neuromotor control deficits following concussion injury. Therefore, it is important for clinicians to be capable of objectively measuring the deleterious effects of concussion on neuromotor control to monitor rehabilitation progress and identify appropriate timing for athletes who have suffered SRCs to return-to-play.
Recently, several groups have identified lingering effects of concussion during tasks related to various constructs of neuromotor control.3,8–11 Studies by Patejak et al., Howell et al., and Martini & Broglio indicate that medial-lateral center of mass (CoM) sway velocity during gait is significantly different between individuals with and without concussion even following the acute phase, particularly when a cognitive task is added to the motor task of gait.3,9,10,12 Additionally, studies by Oldham et al. and Howell et al. have found that individuals with a history of concussion demonstrate a more conservative gait strategy, observable in spatiotemporal parameters (STP), and marked by shorter stride length and slower stride time.13–15 Regarding static balance, Rochefort et al. identified significant differences in center of pressure (CoP) 95% ellipse area one month post-concussion during static balance eyes open (EO), eyes closed (EC), and during a cognitive-motor dual-tasking (DT) condition.11 Regarding reaction time, Eagle et al. found significant differences in reaction time between healthy individuals and individuals with a history of concussion far past the acute phase (Mean = 264 days post-concussion).8
These studies demonstrate that the lasting effects of concussion on neuromotor control can be quantified using force plates, inertial measurement units, and reaction time measurement systems even once they are not detectable using the balance error scoring system (BESS) or posturography tools such as the Neurocom Sensory Organization Test (SOT).11,16 A recent systematic review on the topic of assessing movement deficits following concussion recommended future research focus on low-cost and feasible tools to objectively assess balance and gait tasks due to their accessibility and ability to discriminate between those with and without concussion.17 Evidence suggests that instrumented analysis of gait, balance, and reaction time can objectively and accurately quantify post-acute movement pattern deficiencies following concussion.11,16 However, these tools are often too expensive, large, or time-consuming to be practical for clinical use. For these reasons, there exists a need for the development of objective and cost-efficient measurement devices which accurately assess neuromotor control following concussion using a combination of multiple assessments.18,19
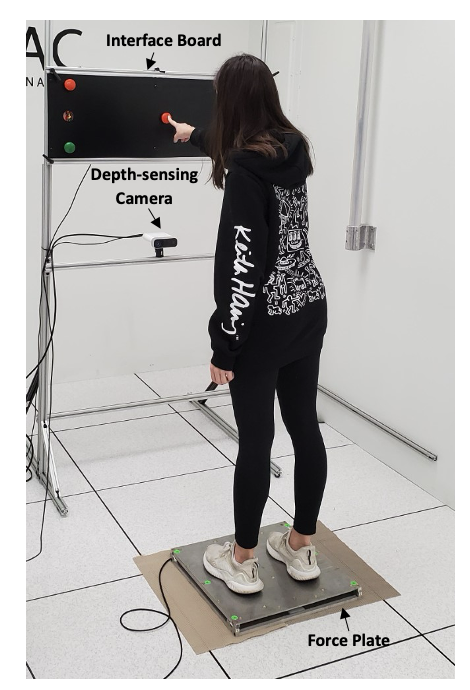
The Mizzou Point of Care Assessment System (MPASS) (Figure 1) has been developed to address this need by combining a depth-sensing camera for motion capture, a custom-built force plate, and a microcontroller-based interface board to measure multiple aspects of neuromotor control following concussion. Prior work using this system has found high correlation values between the MPASS force plate outcome measures and a gold standard AMTI force plate outcome measures during static balance; as well as high levels of agreement between the depth camera motion capture and Vicon marker-based motion capture in detecting spatiotemporal parameters during gait.20,21 The system is designed to cost less than $1,500 and its graphical user interface is designed for clinical use.
_with_components_labeled.png)
The purpose of this feasibility study was to determine the usefulness of MPASS outcome measures for creating a discriminant model classifying individuals as being either healthy or in the post-acute phase of concussion (having suffered a concussion within the prior three months). This study’s central hypothesis was that a linear combination of movement-based outcome measures as assessed by the MPASS will produce a statistically significant discriminative model. The study’s goal is to determine the feasibility of such a device for discriminating between healthy individuals and those recovering from concussion and to demonstrate a framework for future, larger studies to continue the development of this system and others like it.
METHODS
Participants & Research Design
University Institutional Review Board approval was obtained (IRB #2028203) prior to the study and twenty-two participants were assessed (21.95 ± 1.69 yrs., 16 females). Ten participants (9 females) were in the post-acute phase of concussion recovery (>2 weeks post-concussion), and all 10 had sustained concussions within two months prior to data collection (M = 3.9 ± 1.66 wks. post-concussion). The remaining twelve (8 females) had no previous concussions. Aside from concussion diagnosis (determined via physician diagnosis), inclusion criteria included individuals aged 18-35 years. At the time of data collection, average symptom severity (as assessed by the Sport Concussion Assessment Tool- 5th edition, or SCAT5) for the concussion and control groups was 15.33 and 0.91, respectively. Exclusion criteria included musculoskeletal injury within the prior three months. All participants completed written informed consent forms prior to data collection.
Data Collection
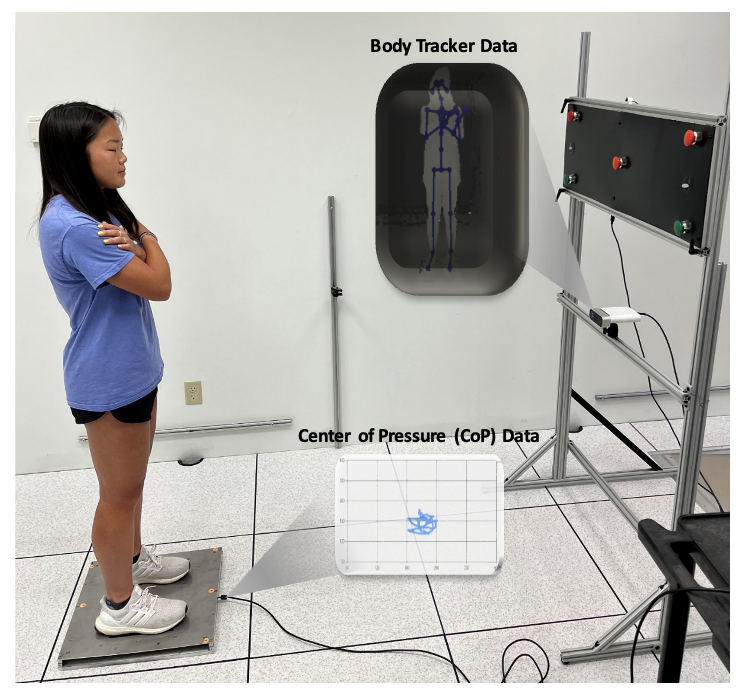
Participants completed one testing session in a laboratory environment. Participants wore athletic clothing and shoes. For MPASS testing, participants were instructed to perform three trials lasting 30 seconds of each static balance task. Static balance tasks included Romberg eyes open (EO) and Romberg eyes closed (EC). All balance tests were completed on a firm surface and in a dual-limb stance. During each condition, participants were instructed to stand as still as possible. Force plate and body motion data were recorded (Figure 2) and then converted to outcome measures.
Participants then performed three trials each of three different conditions of a gait task. These included normal walking, DT (serial subtraction by seven) walking, and head shaking (HS) walking. For each condition, participants were instructed to walk at their normal, comfortable pace from the far end of the lab toward the depth camera until they reached the MPASS device (9.8 m walkway). Numbers for the DT condition were randomly generated from within the MPASS application GUI for each task. These random numbers were constrained between 70-99. For all HS conditions, a metronome embedded within the MPASS beeped at 100 bpm and participants were instructed to turn their head from side-to-side each time they heard a beep.
Finally, participants completed three trials of a 30-second reaction time task. First, participants were positioned at the end of their functional reach such that they could barely touch each button prior to the beginning of each trial. Next, LEDs on either side of the MPASS interface board lit up either red or green with corresponding red and green buttons above and below the LEDs and participants were instructed to press the corresponding button as fast as possible, bringing their hands back down to their sides after each pressed button. Light patterns were pseudo-random such that each trial included a different pre-programmed random pattern of lights, but the patterns for each trial were kept the same between participants. A microcontroller controlled light patterns during reaction time trials and measured the time between LED flashes and button presses, as well as the number of correct buttons pressed.
Data Processing
MPASS data consisting of force plate, reaction time, and body tracking data were stored in text files and then processed using a MATLAB pipeline which first screened the data for capture errors and then calculated the final outcome measures based on trial type (gait, balance, or reaction time). Raw MPASS measurement data included CoP and vertical ground reaction force from the force plate, skeletal joint center and body segment orientation data from the depth camera (Azure Kinect) with body tracking SDK, and reaction time and number of correct button presses from the microcontroller (Arduino).
For balance tasks, outcome measures for both CoP and CoM included principal sway direction,22 95% confidence ellipse area,23 mean total velocity (MTV), mean total velocity in the anterior-posterior (AP) direction, and mean total velocity in the medial-lateral (ML) direction. CoM location was calculated from measured skeletal joint center locations using Winter’s leg, thigh, and head, arms, trunk (HAT) model.24 Prior work has found high agreement between CoM measured with Kinect and with Vicon using the same CoM calculation methods.25 CoM data were then converted into the discrete outcome measures listed above with the addition of sagittal and frontal hip displacement. Hip displacement is defined here as the perpendicular distance, in mm, of the pelvis relative to a line drawn between ankle joints and clavicle joints in the frontal and sagittal planes. Differences in hip displacement measures are indicative of different strategies used to maintain postural control.
For each gait trial, STPs were calculated from joint centers according to previous methods.20 Outcome measures included stride length, step length, step width, and stride time. These measures were calculated for both right and left legs and distance measures were normalized to participant leg length using the Euclidian distance between ankle, knee, and hip joint centers obtained from the depth camera with body tracker during static balance tasks. Values for the right and left legs were then averaged. In addition to spatiotemporal parameters, 95% confidence ellipse area and mean total velocity of CoM in the ML direction were also calculated. These measures were calculated during each stride. Once outcome measures had been calculated for each task and trial type and raw data had been screened for capture errors, outcome measures were automatically uploaded to a structured query language (SQL) database. From there, data were imported into RStudio where trials were averaged by participant identification (ID) number.
Principal Component Analysis
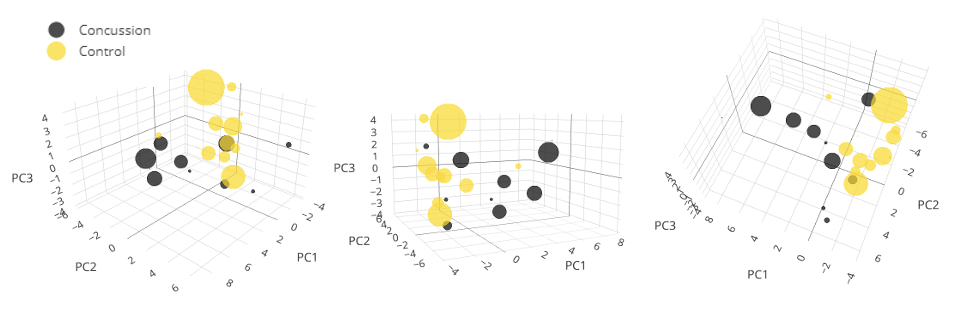
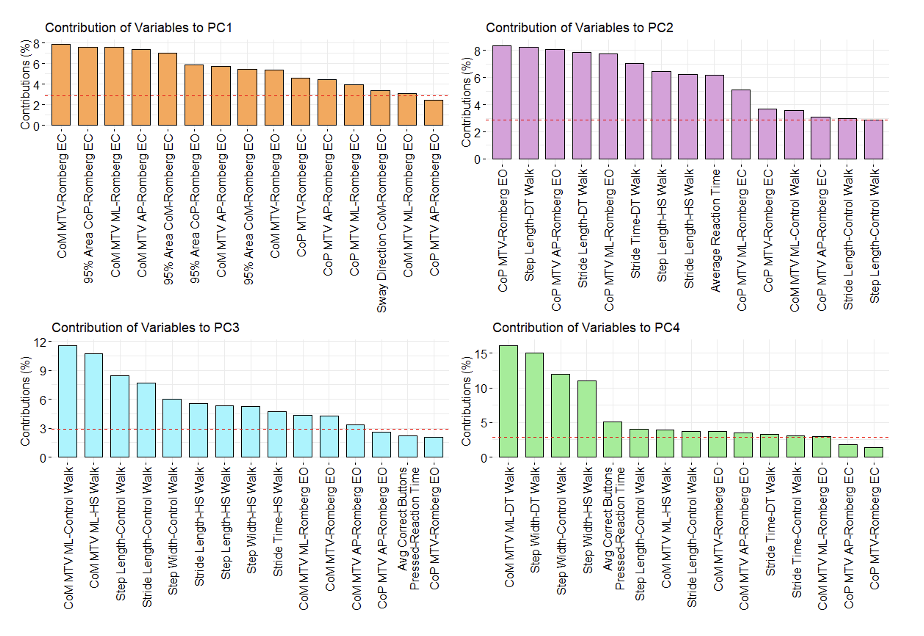
Data processing resulted in 47 unique MPASS variables for each participant. Principal component analysis (PCA) was used to reduce dimensionality and maximize the explained variance within the dataset. This approach was selected both for dimensionality reduction and because many variables were correlated, making them unsuitable inputs for a linear discriminant analysis model. PCA creates new and orthogonal linear combinations of these variables which then serve as inputs for linear discriminant analysis (LDA), as LDA is sensitive to multicollinearity. Four principal components (PCs) which explained 71.6% of dataset variance were retained using Horn’s Parallel Analysis (Figure 3). Contribution analysis was used to determine which MPASS variables significantly contributed to retained PCs (Figure 4). PCA was completed using the stats package (version 4.3.2) in RStudio (v4.3.2).

_to_the_given_pc_liste.png)
Linear Discriminant Analysis
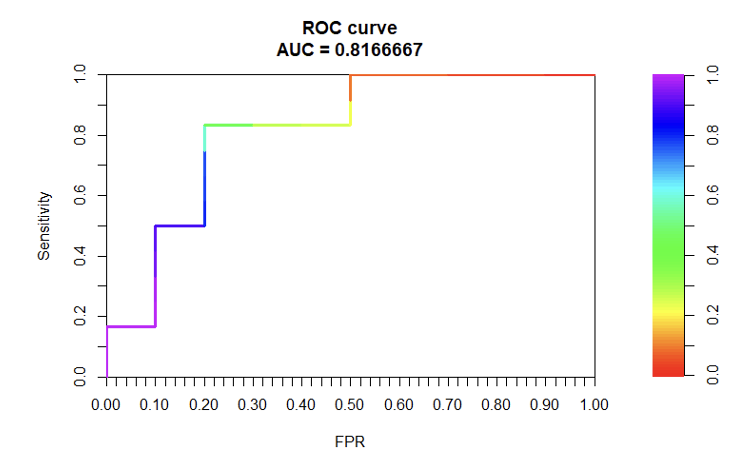
Following PCA, the four retained PCs were used as inputs for a LDA model. LDA was chosen for its previously demonstrated usefulness for creating classification models based on biomechanical and anatomical variables.26–28 The model was trained and tested using the leave-one-out (LOO) cross-validation method. This means that for each of the 23 iterations, the model was trained on 21 samples and tested to predict the sample which was left out. This hidden sample changed on each iteration. LOO was chosen over k-fold cross-validation as it is more appropriate for our small sample size. The statistical significance of the LDA model was determined by comparing its accuracy to the no information rate (NIR), which is the accuracy of the model which could be achieved by predicting only the majority group; healthy, in this case. Area under the curve (AUC) for the receiver operating characteristic (ROC) curve, as well as the model’s sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were also evaluated to assess the performance of the model. Alpha was set a priori at p < 0.05. LDA was completed using the MASS package (version 7.3-60) in RStudio (v4.3.2).
RESULTS
PC1 was comprised entirely of static balance measures, PC2 was comprised of both static balance and gait measures, PC3 was primarily comprised of spatiotemporal gait measures with some balance and reaction measures also present, and PC4 was dominated by postural control measures during gait (Figure 4). It also appears (Figure 3) that much of the discrimination between groups was due to PC1. The resultant LDA model was statistically significant (p < 0.01). The ROC Curve AUC was 0.8167 (Figure 5), giving the model an accuracy of 81.67%. The model’s sensitivity was 80%, specificity was 83%, PPV was 80% and NPV was 80%. These results demonstrate high levels of agreement between predicted and actual counts for each group (Table 1).
_and_sensitivity_plotted_on_the_x-_and_y.png)
DISCUSSION
This work presents a framework for evaluating a multifaceted assessment tool for neuromotor control following concussion. A statistically significant classification model between healthy individuals and those in the post-acute phase of concussion recovery was created using linear combinations of multiple variables. Though sample size was limited, and this model is not generalizable, results indicate promise for continued development of multi-dimensional assessment tools for measurement of post-acute neuromotor symptoms of concussion.
The study’s central hypothesis, that a linear combination of movement-based outcome measures as assessed by the MPASS would produce a statistically significant discriminative model between healthy individuals and those in the post-acute phase of concussion recovery, was supported. Additionally, each of the outcome measures which were previously identified as being significantly different between healthy individuals and those in the post-acute phase of concussion, including reaction time, STPs, ML CoM velocity during complex (head shaking and dual-task) gait, and 95% confidence ellipse area during EC static balance, significantly contributed to at least one of the four retained PCs included in the LDA model (Figure 4).11,13,15,29 This approach combined measurements from various constructs of neuromotor control, measured using one tool, into a single classification model. This is important, as prior studies have indicated that unidimensional measurements, such as SOT composite scores, are not significantly different between individuals with and without concussion in the post-acute phase.18,30 Variables which significantly contributed to retained PCs highlight the necessity of a multifaceted tool for detection of lasting impacts of concussion on neuromotor control. Though further research is needed, the measurement of many discrete variables across various constructs of neuromotor control by one low-cost and portable device addresses a need specified by clinicians and researchers.18,19
Outcome measures during DT gait contributed significantly to multiple retained PCs (Figure 4). Pairing motor and cognitive tasks has previously been shown to degrade motor performance during gait and postural control in the post-acute phase of concussion recovery.5 Higher level neuromotor control ability is extremely important for safe return to sport to include the ability to perform cognitive-motor dual tasking.31 Low-cost and objective measurement technology has the potential to help clinicians implement targeted interventions which address neuromotor control deficits during cognitive-motor dual tasking and reduce the risk of subsequent secondary injury post-concussion. According to the American Physical Therapy Association’s Clinical Practice Guidelines for mild traumatic brain injury, physical therapists should design a personalized intervention plan that aligns with a patient’s movement related impairments.32 Future studies should continue to assess the importance of neuromotor control during cognitive-motor DT as it relates to recovery in the post-acute phase of concussion injury.
Within this sample, it was possible to detect neuromotor control deficits in the post-acute phase of concussion using a low-cost assessment tool. Overall, variables which did significantly contribute to retained PCs point toward lingering changes in gait pattern, differences in reaction time, and differences in postural control as measured by CoP and CoM excursion during static balance by individuals with concussion compared to healthy participants. These findings in the post-acute phase of concussion have been reported by various other groups as well.11,13,15,29 Additionally, while prior studies outside of a gait laboratory have investigated single constructs measured across multiple different assessment systems, the use of a multi-faceted assessment tool allows for the integration of multiple constructs of neuromotor control into one score. This can provide a more objective assessment of critical movement differences, such as spatiotemporal constructs, compared to current clinical assessment tools such as the Functional Gait Assessment and Dual Task Tandem Gait Test which have inherent subjectivity in their scoring.33,34 Creating a platform with easy interpretable objective data for clinicians to use for return to sport/activity has the potential to improve clinical decision making in concussion care.
As previously stated, results from this study lack generalizability due to low sample size. Because of this, the authors are limited in identifying specific tasks or variables which are most important for discriminating between these two groups. However, future studies with larger samples can use the methodology presented within this manuscript to identify important measures for informing precision rehabilitation interventions to address lingering neuromotor control deficits present in the post-acute phased on concussion recovery. Though these limitations exist, the results of the present study demonstrate promising results for future work in using multi-faceted movement-based assessment tools to quantify the effects of concussion on human movement. Future work, in addition to increasing the sample size, should use similar tools to monitor recovery of neuromotor control following concussion. Future studies should also investigate whether the battery of tests administered in this study along with their outcome variables are optimal for detection of neuromotor control deficits only in the post-acute phase of concussion, or if the same tasks are appropriate for individuals in the acute phase of concussion using devices similar to MPASS.
CONCLUSION
This feasibility study used measurements from a low-cost movement assessment tool, the MPASS, to create a classification model using LDA. The work presents a framework for assessing the discriminative power of multidimensional and clinically feasible tools for assessing human movement. Within this study’s sample population, a statistically significant classification model was achieved using MPASS outcome measurements. Future, larger studies should continue to investigate the usefulness of such tools in clinical settings where the technology is most needed.