



INTRODUCTION
The use of mechanical percussive massage treatment using handheld devices has grown immensely among clinicians and athletes. Different manufacturers (e.g., Theragun and Hypervolt) provide percussive devices that vibrate at various frequencies and can be used either as a self-massage or by a healthcare professional. Athletes, both recreational and professional, of all skill levels, playing in various sports use these mechanical devices. Percussive massage devices are used by applying a rapid percussion stimulus at a high frequency to the myofascial tissues of the targeted region.1 These percussive massage devices are often used for therapeutic benefits.1 Therabody, the company that created Theragun, claims that the healthcare benefits of using a massage gun include relief of tension, hydration of muscle tissue, decreased lactic acid, increased blood flow, and improved range of motion by increasing muscle extensibility.2 Although increasing in both popularity and usage, clinicians report varied reasons for the application.1
Prior research demonstrates acute range of motion (ROM) gains from massage therapy, vibration therapy, static stretching, and mechanical percussive massage treatment. Specifically, Davis et al. showed that conventional massage can acutely increase ROM.3 Similar to a conventional massage, vibration therapy of the whole body, as well as vibration of specific muscles, can also increase ROM.1,4 Konrad et al. investigated the effects of percussion treatment of the calf muscles on ROM and maximum voluntary contraction torque of the plantar flexor muscles and found that handheld percussive massage treatment can increase ROM without affecting muscle strength.5 However, a limitation to the Konrad et al. study is that it had a limited sample size (16 healthy male subjects) and no control group.
Research strongly supports that static stretching enhances the extensibility of muscle-tendon units, making it an effective method for increasing range of motion (ROM). Evidence indicates that stretch durations of 12 to 30 seconds are just as effective as longer durations, up to two minutes, in achieving immediate increases in periarticular tissue length.6–8 However, these acute improvements may be attributed to a combination of plastic deformation and neuromodulated changes within the muscle-tendon unit.9
To the authors’ knowledge, no other studies have investigated the acute effects of percussive massage therapy on knee ROM, and no study has compared mechanical percussive massage therapy to traditional stretching. Therefore, the purpose of the current study was to examine the effect of mechanical percussive massage therapy applied to the hamstrings versus static stretching of the hamstrings on passive knee extension (PKE) range of motion.
METHODS
Experimental Design
Data were collected in two locations on two separate days. Subjects were then randomly assigned to one of three groups: mechanical percussive massage treatment, static stretching, or a control group. This was achieved by having them blindly select a poker chip from a bag, which assigned them to the one of the three groups. All subjects were blinded to the intervention they would receive. The study was approved by the institutional review board, and written informed consent was obtained from all subjects before the onset of the experimental procedures.
Subjects
Division II NAIA and NCAA Division III male football players were recruited for participation. Exclusion criteria included any participants with a history of hip, knee, or back injuries that had not returned to full activity/sport or participants still receiving treatment for those injuries.10–12 Subjects with an initial knee extension angle, as described by Gajdosik et al., of 65 degrees (155 degrees total) or greater from the initial 90-degree testing position were excluded.13 Finally, subjects with any complaints of pain, burning, and/or tingling in the extremities were also excluded.
The passive straight leg raise test (Figure 1) was used to differentiate between a musculoskeletal response and an abnormal neurodynamic response. A positive straight leg raise test, indicating an abnormal neurodynamic response, would be a reproduction of radicular type pain along the sciatic nerve distribution or asymmetry in neurodynamic responses between the subject’s two extremities.14 Subjects who screened positive for the passive straight leg raise test were excluded.
The dominant leg was used as the subject’s testing extremity. Leg dominance was established by asking the participant “if you had to kick a ball right now, which leg would you use?”. The kicking leg was deemed the dominant leg. Following the random group assignments, subjects were informed about the procedure they were assigned to participate in but were not informed about the study’s purpose.

Range of Motion Measurement
Passive knee extension (PKE) range of motion was measured (Figure 2) using a universal goniometer. Range of motion was measured on the subjects’ dominant lower extremity in a supine position on a standard treatment table. The hip was placed in 90 degrees of flexion using a goniometer at the following landmarks: greater trochanter for the center fulcrum, lateral midline of the pelvis for the proximal arm, and lateral midline of the femur using the lateral epicondyle for the distal arm.15 The femur was held in place using a Swiss ball at the posterior thigh. The Swiss ball was stabilized on the table using two mobilization straps around the ball and the table. Another mobilization belt was placed around the proximal femur to maintain the hip in 90 degrees of flexion in the sagittal plane. A towel roll was also placed under the participant’s lower back to stabilize the lumbar spine.
A single examiner then passively extended the knee. For this study, the ROM measurement was recorded when the examiner first felt passive resistance of the participant’s hamstring, as described by Norkin & White’s distal hamstring length test.15 A second examiner measured knee ROM with the universal goniometer using the lateral epicondyle and the greater trochanter of the femur and the shaft of the fibula as the landmarks described by Norkin & White.15 To maintain reliability and consistency, a single examiner palpated and marked the landmarks and recorded all the goniometer measurements. The recorded measurements were not shared with the subject or the other examiner who passively extended the knee. Three measurements were recorded pre- and post-treatment (six total measurements).

Mechanical Percussive Massage Treatment
During the mechanical percussive massage treatment (Figure 3), subjects were placed in a prone position on the treatment table. The Hypervolt Pro 2 (Hyperice, California, US) was used for the treatment by the same examiner for the entire study. It was set at medium speed (40 Hz) and the ‘ball-shaped’ attachment head was used for the treatment. The percussive massage treatment was performed on the dominant leg’s hamstring muscle for five minutes. During the first 2.5 minutes, treatment was administered on the lateral hamstrings. For the second 2.5 minutes, treatment was administered on the medial hamstrings. The examiner began treatment to the targeted hamstring muscle on the more medial aspect and moved the massage gun longitudinally, in a straight line, from distal to proximal and back to distal within about 20 seconds. Once back at the distal end, the examiner moved the massage gun to the lateral side of the muscle and again moved the massage gun longitudinally from distal to proximal and back to distal within about 20 seconds. The examiner used the pressure indicator on the speed dial staying at two lights to ensure consistent pressure within the treatment session and between subjects throughout the study.

Static Stretching Treatment
During the stretching treatment, subjects were placed and stabilized in the same supine 90-90 position, described when measuring knee range of motion. The same examiner performed all hamstring stretching throughout the entire study. The examiner performed the hamstring stretch passively by slowly extending the subject’s knee of the dominant leg. The stretch was performed until the subject reported a “moderate to strong pulling sensation” in the posterior thigh.6 The stretch was held for 30 seconds and repeated three times with a 10-second rest between each repetition.6,9
Control Group
Subjects in the control group were placed in the same prone position as the mechanical percussive massage treatment group for five minutes; however, no massage treatment or stretching was performed.
STATISTICAL METHODS
SPSS version 25 was used for all the statistical analysis. To assess the reliability and internal consistency of the three replicate preintervention measures and three post-intervention measures, Cronbach’s alpha was utilized to measure internal consistency. An intraclass correlation coefficient was used to test the reliability of the replicated measures. To investigate the effects of the three treatment conditions on hamstring ROM, a full factorial 2 x 3 mixed ANOVA design was used. The within factor includes two levels, pre, and post-test; each level represents the average of three measures. The between factor comprises the three treatment conditions: control, stretching, and mechanical percussive massage. The ANOVA results estimate the two main effects, pre-post and treatment group, and the interaction term of time x treatment.
RESULTS
Seventy-nine male collegiate football players, 37 NCAA Division III and 42 NAIA Division II (mean age 19.8 years +/- 1.2) participated in this study. Table 1 summarizes the three pretest measures, Cronbach’s alpha =.987 and the intraclass correlation coefficient (ICC) = .99 for the average measures, indicating high consistency and reliability for the three pretest measures. The post-test measures also revealed very high consistency (alpha = .992) and reliability (ICC = .99). In consideration of the high reliability of the pretest and post-test measures, the data were combined into the average pretest score and average post-test score to facilitate a more parsimonious model. Table 2 summarizes the average factor level scores for pre-posttest and the treatment groups and the simple effects scores for the interaction term.
All three of the featured effects are statistically significant indicating the posttests are significantly higher than the pretest F (1, 76) = 66.2, p <o .001, = .465 there are significant differences between the treatment groups F (2, 76) = 7.3, p = .001, = .161 and there is a significant interaction between time and treatment F (2, 76) = 27.0, p<.001, = .415. In Table 3, pre-test, post-test, and average group scores were compiled.
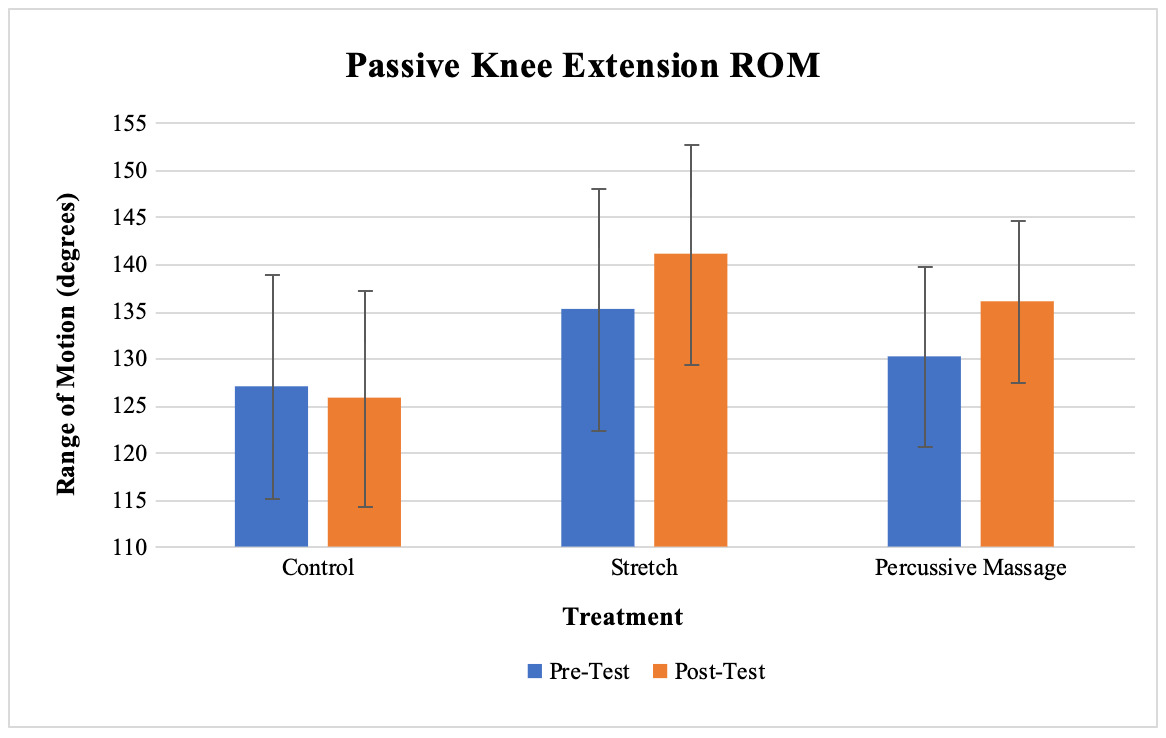
The bar graph below (Figure 4) indicates the average values for all three groups in respect to their range of motion measurement. The gap in the lines between the pretest and posttest for the stretch and percussive massage groups reveal the significant differences identified in Table 4. The equality in the control group between the pre-post-tests when compared to the stretch and percussive massage group is the source of the significant interaction term, that is, the differences in the pre-post scores depend on the treatment group. The pre-post gains for the stretch group drops (when adjusted for the variability) resulted in an effect size (d = 2.1) nearly twice as large as the effect for the percussive massage group (d = 1.1). While the average posttest scores between the groups was not significantly different, the effect size for the stretch group indicates a greater relative increase in ROM. There is evidence the intervention resulted in significant increases for the stretch group and percussive massage group. The simple effects reveal that in the pretest scores the percussive massage group was equal to the control group but scored significantly higher than control in the post-test. The stretch group started at a significantly higher level than the control group and remained higher in the post-test. The observed differences between the mechanical percussive massage and stretch groups were not statistically significant for either testing period.
DISCUSSION
The aim in this study was to investigate the effects of a five-minute mechanical percussive massage treatment versus static stretching of the hamstring muscles on PKE ROM. Both treatments, mechanical percussive massage and static stretching, resulted in significant increases in PKE ROM compared to a control group. However, no significant differences existed between the two treatment groups.
These results are similar to the findings of Konrad et al.5 who examined mechanical percussive massage treatment of the plantar flexor muscles and effects on ankle dorsiflexion range of motion and performance. Like this study’s findings, Konrad et al. found that mechanical percussive massage to the plantar flexors resulted in increased ROM (dorsiflexion).5 However this study differed as it compared percussive massage treatment to static stretching and did not examine maximum voluntary contraction torque.
There is little evidence to show or explain the effect found after percussive massage treatment. Previous studies have discussed how mechanical percussive massage treatment may create physiological, neurological, and psychological changes. Examples of these changes include increasing blood flow, decreasing pain perception, and increased muscle relaxation, were outlined by Weerapong et al.16 Mechanical pressure increases arteriolar pressure, as well as increasing muscle temperature, and increasing blood flow to the area could also provide a physiological response to the treated muscle region. Mechanical pressure also decreases neural excitability, as measured by the Hoffman reflex.17
Cheatham et al. compared the effects of a vibrating roller and a non-vibrating roller to the quadriceps muscle on knee range of motion and pain perception.18 They found that a vibrating roller applied to the quadriceps increased the knee flexion range of motion and decreased pain perception. These findings suggest that percussion or vibration massage decreases pain perception threshold as well as muscle stiffness and improves muscle relaxation, therefore increasing ROM.18 Percussive massage combines the mechanical pressure from the device as well as the vibration, making the conclusions from Cheatham et al. and Weerapong et al. potentially relevant to this study. The increase of PKE with the percussive massage treatment group may be due to physiological, psychological, and neurological changes, but more conclusive research is needed to further explore these results. No matter the reason for the changes, practitioners like physical therapists and athletic trainers can utilize percussive massage treatment on the hamstring muscle group to acutely improve knee extension range of motion.
There is a vast amount of research explaining mechanisms for why static stretching increases ROM.19–24 Most of the research explains the effects to be a result of a decrease in soft tissue stiffness and/or pain perception. However, other forms of stretching like dynamic, active, or proprioceptive neuromuscular facilitation (PNF) stretching (contract-relax or hold-relax) have been found to be more effective than static stretching to increase ROM of hamstrings and should be implemented prior to sporting activity.17 The examiners of the current study elected to perform static stretching over other forms of stretching because of the abundance of evidence demonstrating its effectiveness and the ease by which static stretching can be consistently performed compared to the variability that may be present with other forms of stretching. To the authors’ knowledge, no other studies have compared any forms of stretching to percussive massage treatment. Although no significant differences were found between the treatment groups, different results might occur if the percussive massage device were compared to other forms of stretching.
This study provides clinicians with information that can be utilized in the decision-making process regarding either purchasing a mechanical percussive massage device or simply performing manual static stretching exercises. As there was not a significant difference between using a mechanical percussive massage percussive massage device and static stretching to increase PKE ROM acutely, either could suffice. The decision to purchase one of the many percussive massage devices can be based on clinician preference and financial ability.
As noted in the current study and by Konrad, percussive massage devices can facilitate an increase joint ROM, which can be beneficial.5 Additionally, the application of percussive massage devices can be applied by many practitioners. These devices could have a positive impact in settings such as outpatient orthopedics, sports medicine, neurological rehabilitation, acute care, inpatient rehab, and skilled rehab.
The current study was limited to one session of treatment performed on a single day. Results could change if subjects were treated with static stretching or mechanical percussive massage consistently over a period of time. PKE was only measured immediately after the treatments were performed, accounting only for acute changes. Changes may occur over longer periods of time, however, further research is needed to evaluate the longer-term effects on passive knee extension range of motion. Furthermore, although no significant differences were found between ROM between interventions acutely, it cannot be concluded whether one treatment is superior to the other when testing hours or days. Only young, healthy, male football players were included. Therefore, the results of the study could differ with other populations. Finally, all percussive massage devices are not the same and there are many parameters that can be chosen. More research needs to be performed on evaluating the effects of utilizing different parameters (frequency, pressure, time of treatment, delivery attachments) on human subjects.
While the current study only focused on hamstring extensibility, future studies should investigate the effects on pain, muscle performance, and delayed-onset muscle soreness. Mechanical percussive devices could also be compared with other forms of stretching or even other common modalities utilized in physical therapy, such as foam rolling, dry needling, and soft tissue massage instruments.
CONCLUSION
This was the first study to compare static stretching to mechanical percussive massage therapy and their acute effects on hamstring extensibility. The results indicate that static stretching and mechanical percussive massage therapy both produced significant immediate increases in PKE compared to a control group. However, there were no significant differences between the two treatment groups. These findings suggest that static hamstring stretching and mechanical percussive massage therapy are both viable options for increasing hamstring extensibility acutely.
CONFLICT OF INTEREST
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
The completion of this study would not have been possible without the support of the football programs.