Introduction
Basketball has one of the highest injury rates among team sports.1,2 Professional basketball players tend to have a higher injury rate compared to players at other levels.3,4 The incidence of BRMIs is estimated to be between 10.8 to 19.1 injuries per 1000 hours of athletic exposure in professionals,5,6 with the lower limbs being the most affected region, accounting for 64.7% of injuries, followed by injuries to the trunk/spine (12.9%), and upper limbs accounting for 12.2%.7 A recent systematic review indicates that the most common orthopedic injuries that occur in the National Basketball Association (NBA) were hand fractures (3.5 to 5.5/year), lower limb stress fractures (4.8/year), meniscal injuries (2.3 to 3.3/year), and anterior cruciate ligament injuries (1.5 to 2.6/year).8
Studies have been conducted to identify the most common BRMIs among basketball players.7,8 However, heterogeneity in injury definitions, classification methods, and study populations does not provide clear direction regarding the most common BRMIs, nor their functional consequences. Investigating sports injuries is valuable to confirm and/or formulate hypotheses about the injury mechanism(s) which may help to guide coaches, healthcare professionals, and researchers to direct resources regarding development of specific prevention and intervention strategies to decrease both the incidence and severity of these injuries.2 Therefore, the purpose of this study was to investigate the clinical incidence, rate, location, type(s), severity, and nature of BRMIs in Brazilian professional basketball players, and to quantify their impact on sports performance.
Methods
Study Design
An observational cohort study, with an epidemiologic focus was employed.
This study was approved by the Research Ethics Committee of the Federal University of São Paulo/Paulista School of Medicine. Male professional basketball players from the Brazilian professional male basketball national championship (“New Basketball Brazil” NBB) were recruited. Inclusion criteria required active participation in the league and a signed Consent Form, while exclusion criteria included athletes with incomplete survey responses. Nine out of the sixteen Professional teams authorized their athletes’ participation in the study.
All included athletes signed the Informed Consent Form (ICF). Data were collected on a weekly basis over 22 weeks (from November 2019 to March 2020) through electronic questionnaires distributed by team Physical Therapist (PT). The questionnaire collected demographic data (age, height, and weight), sports-related factors (playing position), exposure to practice and games, and recorded BRMIs.
BRMIs were defined as any musculoskeletal-origin pain resulting in consultation with a PT that was related to practice or game participation.9 The Orchard Sports Injury Classification System (OSICS) was used to provide anatomical and diagnostic classification of BRMIs.9,10
A single experienced healthcare professional evaluator (with over 15 years of clinical practice) analyzed each reported injury. BRMIs were classified as acute (onset linked to a specific injury event) or overuse (not linked to a clearly identifiable event),11 and whether it was recurrent injury (defined as the same type and in the same location as an injury that occurred in the previous year).12
The Oslo Sports Trauma Research Center questionnaire (OSTRC)11 was also distributed weekly to athletes with BRMIs through an online survey. It consisted of four questions: 1) sports participation; 2) practice or game volume; 3) performance; and 4) symptoms of injuries. BRMIs were categorized as major severity (resulting in moderate or large reductions in practice volume and performance or completely unable to practice or game) or minor severity (resulting in no or slight reduction in practice volume or performance), according to the results of questions 2 and 3 of the OSTRC questionnaire.13,14
A severity score, ranging from 0 to 100 (the higher the score the higher the impact on sports performance) was calculated for each BRMI based on the OSTRC questionnaire. The accumulated severity score (sum of the severity scores measured each week) was calculated as an estimate of the total impact each BRMI had during the study period. BRMIs average weekly severity score was calculated by dividing the cumulative severity score by the number of weeks the problem was reported.14
Data Analyses
Qualitative variables were represented by frequency and proportions, and quantitative variables by mean and standard deviation. The normality of quantitative variables was tested using the Shapiro-Wilk test. As an athlete may have had more than one injury during a follow-up period, clinical incidence was calculated by dividing the number of BRMIs by the total number of individuals at risk.15 Incidence was also expressed as a rate by dividing the number of BRMIs (total, in games or practice) by exposure in hours (total, in games or practice).15,16 Practice exposure time was defined as the mean number of practice hours offered by teams multiplied by 22 weeks of the study, and the accurate game exposure time of each athlete in the evaluated season was obtained on the “New Basketball Brazil” (NBB) website.17 Analyses were performed using R version 4.0.2 software, and significance was considered at p<0.05.
Results
The mean participant age was 28.8 years (± 5.4 years), mean BMI 24.9 kg/m2 ( ± 1.7 kg/m2), and 31 (30.1-%) were shooting guards, 7 (6.8%) small-forwards, 24 (23.3%) power-forwards, 22 (21.4%) point guards, and 19 (18.4%) centers (Table 1).
A total of 164 injuries were reported during the study period, with a clinical incidence of 1.6 injuries of the course of the study. Out of these, 122 (74.4%) occurred in the lower limb, 22 (13.4%) in the upper limb, and 20 (12.2%) in the head/trunk/spine. Among these, 155 (94.5%) were new, of which 95 (57.9%) presented as minor severity, and 127 (77.4%) were acute. More than half of the injuries, 102 (62.2%) occurred during practice, and 62 (37.8%) during games. The mean time off was 6.1 days (SD ± 14.6) (Table 2).
The 103 athletes had a total exposure time (between games and practice occurring during the season) of 19,323.43 hours, with 18,556.88 hours of practice and 766.55 hours of games. Considering the 155 new injuries, an incidence of 8.0 injuries per 1,000 hours of practice/game was observed, with 5.1 injuries per 1,000 hours/practice and 79.6 injuries per 1,000 hours/game.
The most frequently affected anatomical location by BRMIs was the knee (19.5%; n=32), followed by hip/groin (15.2%; n=25), thigh (14%; n=23), and ankle (12.8%; n=21) (Tables 3 and 4).
Muscle injuries occurred most frequently (33.5%; n=55), followed by traumatic injuries (18.3%; n=30), joint sprains (15.2%; n=25), and tendon injuries (14.0%; n=23) (Tables 4 and 5).
The accumulated OSTRC score for the total amount of BRMIs was 18,065 points, with a mean of 39.04 points (SD ± 30.67) (Table 6).
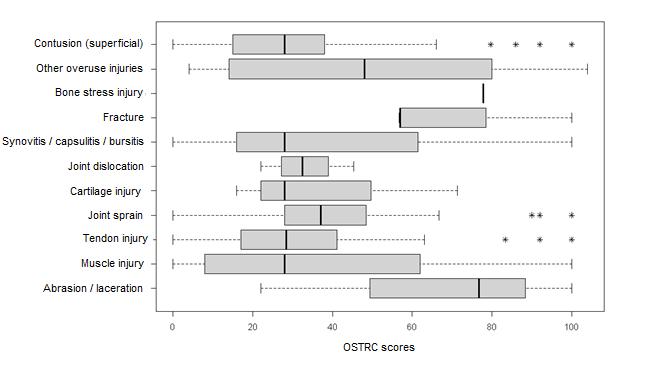
Injuries with the highest cumulative severity were muscle injuries (4,070 points), tendon injuries (3074 points), other overuse injuries (3,489 points), and joint sprains (2,748 points) (Figure 1), but the injuries with the highest mean severity score were stress fractures (77.8 points), bone fractures (71.2 points), and lacerations and abrasions (66.3 points).

The anatomical location with the highest mean severity score was the head (57 points), followed by the pelvis, buttocks (53.6) and foot (46.9) (Table 7).
Discussion
The present study aimed to investigate the clinical incidence, rate, location, types, severity and nature of BRMIs, as well as to assess their burden on sports performance, through the OSTRC score. To date, this is the first study to prospectively collect epidemiological data on BRMIs in professional basketball players in Brazil.
In this study, 74.4% of all injuries occurred in the lower limbs (i.e. 122), corroborating with literature findings showing this area as the most affected by injuries in professional basketball players (64.7% to 62.4%).1,4 As basketball is a sport that involves sudden changes of direction, lateral movements, jumps, and landings,7 these results are not surprising and BRMIs are expected to be more frequent in the lower limbs.
Regarding the affected area, a 2018 systematic review7 reported that most injuries occurred in the ankle (21.9%) followed by the knee (17.8%). Most authors have described the ankle as the most common injury site in basketball.1,3,18–20 However, some authors report the knee as the most affected anatomical location.18,19 In the present study, the knee was the site with the highest number of injuries, 32 (19.5%), followed by the hip/groin 25 (15.2%) and the thigh 23 (14%). This fact may be related to the widespread adoption by players of combinations of neuromuscular preventive exercises for the ankle and the use of external protection (brace) or rigid tape (taping).21
Regarding the type of BRMIs, muscle injuries were the most common in this study occurring in 55 players (33.5%). Drakos et al.6 found muscle spasm and strain injuries as the third most common injury in professional basketball players. Other authors have also found a high frequency of muscle injuries, 21.2% to 21.8% of all injuries, which is lower than the current findings.5,6 The lack of primary attention to muscle injuries with preventive measures and assessments to detect strength asymmetries between the most affected muscles may be contributing factors to this high percentage.
The second most common injuries were traumatic, occurring in 30 players (18.3%), which likely had direct trauma as a causal factor. This is to be expected since basketball involves a lot of physical contact. According to the literature, although traumatic injury occurs (10.4%) in professional athletes,6 that reported incidence differs from that observed in the Brazilian championship (NBB). Different playing and defense styles may influence this discrepancy. Studies conducted with school and college athletes in the United States have shown contact with another athlete was the main cause of injury, in 47.8% and 49.5% of athletes, respectively.22,23 The third most common injury in the present study was joint sprain (25, 15.2%), which differs from the literature that describes joint sprain as the main injury in basketball players.6
Regarding the situation during which injury occurred, the most frequent BRMIs that occurred during practice were muscle injuries (38. 37.3%), tendon injuries (19, 18.6%), and joint sprains (14, 13.7%), however, during games, traumatic injuries (19, 30.6%), muscle injuries (17, 27.4%), and joint sprains (11, 17.7%) were the most common. Drakos et al6 reported joint sprains (35.5%), traumatic injuries (21.3%), and muscle injuries (19.5%) as the most common injuries that occurred during games. Traumatic injuries are possibly more common in games due to competitiveness, intense battles for the ball, and vying for position on the court, which increase the possibility of collisions between players. In addition, player substitutions are less frequent in games and the physical and mental stress that stem from game participation can lead collectively to a higher incidence rate of BRMIs in games than in practice.5 Consistent with this thinking, the present study reports a higher incidence rate of BRMIs in games 79.6 per 1000 hours/game compared to 5.1 per 1000 hours/practice which are very similar values found in the literature.5
When compared to the literature,5 a factor that may help explain to the lower incidence rate of BRMIs in practice in this study may be the fact that many athletes did not report their injuries to the club’s health department to avoid missing practice and/or game sessions. Additionally, the high workload and travel of club professionals may hinder the identification and registration of some complaints during championship play.
BRMIs with the greatest impact (higher cumulative OSTRC score) were muscle injuries (4,070 points), tendon injuries (3,074 points), other overuse injuries (3,489 points), and joint sprains (2,748 points). Although these types of injuries are not the most frequent, (except for muscle injuries) they have a significant impact on athletes’ performance.
Of the reported BRMIs, 74 did not result in absences from practice and games, but 90 did. BRMIs without absences had a cumulative OSTRC score of 1,649, and those with absences had a cumulative OSTRC score of 16,416 which illustrates the importance of using the OSTRC not only to know the incidence and prevalence of injury but also to record the burden on the athlete’s practice and games. For instance, an athlete, even without being absent from practice, may be markedly affected by training and game time and intensity, due to the burden of the injury, as shown by the OSTRC score results, what may negatively affect the technical and physical quality of the practice week. This could have an impact on both game results and the possibility lead to increased number and severity of injuries.
The highest mean OSTRC score values were found in stress fractures (77.8 points), bone fractures (71.2 points), lacerations and abrasions (66.3 points), and other overuse injuries (47 points). The variability of the OSTRC scores was greater in overuse injuries, muscle injuries, and synovitis. The outliers of traumatic injuries, joint sprains, and tendon injuries show that, despite the low OSTRC median, there were athletes who had sustained these injuries with high OSTRC values, which is atypical for this type of injury (Figure 1). Study findings highlight the importance of monitoring injuries even without time loss so the team’s medical/performance staff could intervene to reduce their impact in athlete’s training and competition. Focus on prioritizing standardized preventive and rehabilitation measures to mitigate the risk of muscle and tendon injuries, and joint sprains, which have the greatest impact on professional Brazilian basketball. This may help reduce time-loss and injury burden.
Limitations of the present study include the possibility of non-reporting injuries by athletes; therefore, some injuries may have been underestimated. Furthermore, the authors cannot rule out data collection bias or reporting fatigue, as the high workload of club professionals may have hampered the reporting of all weekly athletes’ injury complaints. Further epidemiologic studies should be conducted using the OSTRC score to compare to these findings.
Conclusion
The clinical incidence of BRMIs was 1.6 over the 22-week study period, and the observed rate was 5.1 injuries per 1000 hours/practice and 79.6 injuries per 1000 hours/game (~15-fold higher during games than practice). The anatomical location most affected by BRMIs was the knee (19.5%). Muscle injuries had the highest frequency (33.5%) and the highest cumulative severity. These results provide a foundation for future research aimed at injury prevention and suggest that implementation of preventative strategies need to be specific in the professional Brazilian basketball context.
CORRESPONDING AUTHOR
Vinicius Castro Campos
Rua Santos, 297, Apartamento 101, bairro Jardim América, Belo Horizonte
Minas Gerais, Brasil.
Telephone: +55(31)999831016
e-mail: viniciuscastrocampos@gmail.com.
Conflicts of Interest
The authors report no conflicts of interest.
Acknowledgements
The authors would like to sincerely thank their peers for their invaluable help in collecting data from the participating basketball teams. We also extend our gratitude to the athletes, coaches, and staff for their cooperation, which made this research possible. This work reflects the strength of collective effort and collaboration.
DATA SHARING STATEMENT
All data relevant to the study are included in the article or are available as supplementary files.