

INTRODUCTION
Exercise-induced hypoalgesia (EIH) is a well-documented phenomenon where acute exercise results in a reduction in pain sensitivity.1–3 EIH has been studied across various modes of exercise with aerobic, isometric, and dynamic resistance exercises demonstrating consistent reductions in pain sensitivity in healthy individuals.1,4,5 While the mechanisms of EIH are still unclear,5,6 exercise prescription appears to impact EIH, as exercise bouts of higher intensity or longer duration elicit greater magnitudes of EIH.4 This reduction in pain sensitivity may be observed locally, at the exercising muscle, or systemically at a non-exercising site.1,3,7 Local and systemic EIH have been observed during dynamic resistance exercise, but inconsistent methodology has been applied regarding the intensity and duration of exercise required to elicit a greater magnitude of EIH.8,9 EIH research holds clinical relevance, particularly in populations experiencing chronic musculoskeletal pain, where exercise is often recommended as a non-pharmacologic intervention. Understanding the mechanisms and factors influencing EIH responses could enhance its application in clinical and rehabilitative settings, optimizing exercise prescriptions for pain management.
Understanding the inconsistencies when measuring EIH response would provide a model for developing a more standardized methodological approach to assessment. An important first step is measuring the reliability of EIH after dynamic resistance exercise. Recent systematic reviews on this topic report that the reliability of EIH in pain-free individuals is poor.10 However, research is limited, with only five studies, to the authors’ knowledge, examining reliability of EIH.10 Notably, none of these studies have investigated the reliability of EIH following dynamic resistance exercise. Prior studies have also examined EIH with pressure pain threshold (PPT) alone, demonstrating strong correlations and excellent reliability before and after a period of quiet rest.11 Including multimodal measures of pain assessment (heat pain threshold (HPT)) would provide a more comprehensive understanding of the mechanisms involved in EIH and enhance the stability of measurements when assessing HPT and PPT.
Therefore, identifying an exercise model that effectively targets relevant musculature and reliably elicits EIH is necessary for establishing consistent measurement protocol. The 45-degree Roman chair is a dynamic resistance exercise targeting the low back musculature, particularly the erector spinae, hamstrings, and gluteal muscles.12–14 This extension-based exercise mimics activities of daily living and is one of the few dynamic back exercises that can allow for progressive overload of the spinal flexors and extensors directly.12,15 Training the back musculature may help alleviate lower back pain through greater muscular endurance.13 Similar back extension exercises reduce low back pain, yet the unique biomechanics and muscle activation patterns associated with the 45-degree Roman chair warrant specific investigation.16,17 The Roman chair may produce local EIH due to activation of erector spinae during dynamic flexion and extension, while potentially inducing systemic EIH as well. However, to our knowledge, there is no research on this exercise’s impact on pain perception and the ability to reliably produce EIH.1,3
Therefore, the purposes of this study were to determine the reliability of heat pain threshold (HPT) and pressure pain threshold (PPT) measures, examine local and systemic EIH effects after a 45-degree Roman chair exercise, and determine if EIH was produced reliably between sessions.
METHODS
Participants
Thirty-five asymptomatic, healthy participants between 18-60 years and were enrolled from 01/08/2024 to 04/22/2024. All enrolled participants completed all sessions. Exclusion criteria included the following: inability to appropriately perform the intervention, exceeding safety thresholds, non-English speaking, regularly using prescription pain medications, current or history of chronic pain condition, presence of a pain condition known to affect sensation, known presence of cardiovascular, pulmonary, or metabolic disease, currently using tobacco products, not physically ready to exercise without a medical exam as indicated by the Physical Activity Readiness Questionnaire Plus (PAR-Q+), surgery, injury, or fracture within the past 6 months, or pregnant. Participants who exceeded safety thresholds of 50° C or 1000 kilopascals (kPa) of pressure during screening were also excluded from the study. Participants were instructed to continue their normal activities of daily living prior to each session, but no additional pre-visit instructions were given. The University of Central Florida’s Institutional Review Board (IRB) approved this study (Study #6267) and all participants provided written informed consent.
Study Overview
Figure 1 presents the flow of the study. Participants attended two testing sessions separated by a minimum of 48 hours.

Session 1
For all testing sites, the dominant side was tested. Dominance was determined by asking participants which hand was preferred for writing. For HPT, a 6.6 x 4 x 4.4 -cm T11 thermode attached to a TCS-II device (Strasbourg, France) was applied to the skin. The thermode increased from a baseline of 32°C to a maximum of 50°C at a rate of 1°C/second. Participants indicated the transition from warmth to pain by pressing a button when the sensation changed from “comfortable warmth to slightly unpleasant pain.” Participants rated pain during HPT with a 101-point numeric pain rating scale (NPRS) in which 0 indicated “no pain” and 100 indicated the “the most intense pain sensation imaginable.”18–20 HPT testing was applied to the upper trapezius muscle, 10 cm from the acromion in direct line with the seventh cervical vertebra and erector spinae, 3 cm laterally from the 4th spinous process.21–23 During the upper trapezius trials, participants were seated with their legs supported and asked to lie prone on a table for the low back trials. Two trials were taken for each site with 30 seconds of rest in between and the average temperature and pain rating were calculated.
Next, PPT was examined with a computerized pressure algometer (AlgoMed, Ramat Yishai, Israel). Pressure was applied with a 1 cm diameter rubber tip at a constant rate until participants pressed a button when the sensation changed from “comfortable pressure to slightly unpleasant pain” followed by pain rating. Two trials with 30 seconds of rest between, were performed on the upper trapezius and the erector spinae of the low back, with the average value for PPT used for analysis.
After HPT and PPT, participants completed quiet rest for three minutes. Participants sat quietly and after the three minutes had elapsed, HPT and PPT were repeated. Finally, EIH was examined. Participants performed one set of the back extension exercises on a 45-degree Roman chair (Caphaus, Houston, TX) for as many repetitions as possible (AMRAP). This method was chosen because previous studies involving the 45-degree Roman chair have used an AMRAP protocol and EIH literature has reported that higher intensity resistance exercise may elicit a larger magnitude of EIH.4,12 Participants were familiarized with the Borg Rating of Perceived Exertion (RPE), Category-Ratio scale (Borg CR10) and instructed to provide a rating of perceived exertion after completing the exercise. The Roman chair was adjusted so the thigh pad rested just below the iliac crest and the footrest allowed the participants’ feet to rest flat with their ankles comfortably supported. The investigator provided a demonstration of the exercise. Participants were instructed to keep their hands crossed across the chest and to maintain a neutral spine position throughout the exercise, avoiding excessive arching or rounding of the back. To start the movement, participants began with the spine flexed. Instructions were given to engage the low back, gluteal, and hamstrings to extend the spine raising the body until a neutral spine angle was achieved. Spinal flexion was then performed, lowering back to the starting position in a controlled manner. Each participant then performed two to three practice repetitions to familiarize themselves with the equipment and movement. Once the participant was comfortable and ready to begin, a metronome was used to set a consistent pace (60 bpm), and each flexion/extension cycle lasted four seconds. Participants were instructed to perform one set of the exercise for “as many repetitions as possible” and to maintain a consistent pace with the metronome while attaining full range of motion. The test was terminated by the investigator if the participant was unable to keep pace with the metronome or had a breakdown of form, such as not performing a full range of motion. The number of successful repetitions was recorded. Immediately after the exercise, participants rated their exertion using the Borg CR10 scale. HPT and PPT assessment were then repeated at both sites post-exercise.
Session 2
Participants returned for a follow-up session, a minimum of 48 hours and a maximum of two weeks between sessions was allowed. During the second session testing procedures from the first session were repeated, including HPT and PPT before and after a quiet rest period, Roman chair exercise, and post-exercise HPT and PPT.
Statistical Analysis
IBM SPSS statistical software (Armonk, NY, Version 29.0) was used for statistical analysis. Descriptive statistics were calculated to characterize the total sample by demographic factors. All values are presented as mean (standard deviation [SD]).
The primary aim of this study was to determine within session reliability for HPT and PPT measures after a period of quiet rest. A paired samples t-test was performed to analyze HPT and PPT values before and after a period of quiet rest for Sessions 1 and 2. Cohen’s d was used as a measure of effect size, with values of 0.2, 0.5, and 0.8 representing small, medium, and large effects, respectively, to quantify the magnitude of differences between groups.24 Separate tests were performed for HPT and PPT within each session. Pearson’s r and intraclass correlation coefficients (ICCs) for a two-way mixed effect model based on a single rater (ICC3,1) were used, reflecting the ability of the PPT and HPT responses to differentiate between individuals. ICCs and correlations were analyzed for HPT and PPT values pre and post quiet rest to determine within session reliability. When interpreting ICC3,1 >0.75 indicates excellent reliability, 0.40-0.75 indicates fair to good reliability, and <0.40 indicates poor reliability.25 These reliability estimates have been used in prior studies determining EIH reliability.10,11 When interpreting Pearson’s correlation coefficients, 0.90-1.00 is very strong, 0.70-0.90 is strong, 0.50-0.70 is moderate, and 0.30-0.50 is considered a weak correlation.26 These values can be positive or negative to denote directionality.26 The standard error of measurement (SEM) was calculated as: SEM = SD √1-ICC.27 Minimal detectable difference (MDD) needed to be considered real were calculated as: MD=SEM × 1.96 × √2.27
A secondary aim of this study was to compare the changes in PPT and HPT after performing a back extension on the 45-degree Roman chair by testing site. A three-way repeated measures analysis of variance (ANOVA) examined for time (pre-exercise/post-exercise) × site (upper trapezius/low back) × condition (HPT/PPT). Separate analyses were performed for each session. For all repeated measures analyses, simple effects decomposition with a Bonferroni correction was performed and if the assumption of sphericity was violated, the Greenhouse-Geisser correction was applied. An alpha level of 0.05 was established. Partial eta squared (ηp²) was used to measure the effect size, with values of 0.01, 0.06, and 0.14 representing small, medium, and large effects, respectively, to quantify the proportion of variance explained by each factor or interaction in the model.24
The final purpose of this study was to determine the test-retest reliability of EIH assessed with HPT and PPT measures after a back extension exercise. A two-way repeated measures ANOVA was conducted for session × location to analyze EIH values post-exercise between Sessions 1 and 2. Separate analyses were performed for HPT and PPT. ICC3,1 and correlations were performed for post-exercise values for Session 1 and 2 to determine reliability. SEM was calculated as: SEM = SD √1-ICC.27 Minimal difference (MD) needed to be considered real were calculated as: MD=SEM × 1.96 × √2.27 Separate analyses were performed for HPT and PPT.
RESULTS
Descriptives
A comprehensive analysis of the total sample of 35 participants was completed as demonstrated in Table 1.
Reliability of HPT and PPT Measures
HPT Reliability
During Session 1, HPT of the upper trapezius was not significantly different (t(34)=-0.722, p=0.475) with a small effect size (Cohen’s d = -0.122), indicating there were no significant changes in pain threshold before and after a period of quiet rest. HPT of the low back during Session 1 was significantly different (t(34)=-2.055, p=0.048), with a medium effect size (Cohen’s d=-0.347), indicating there was a significant change in pain threshold before and after a period of quiet rest. During Session 2, HPT of the upper trapezius (t(34)=-2.375, p=0.023) and low back (t(34)=-4.021, p<0.001) were significantly different, with small to medium (Cohen’s d=-0.40) and medium to large effect sizes (Cohen’s d=-0.680) respectively, indicating significant differences in pain thresholds for both the upper trapezius and low back after a period of quiet rest. Collectively, HPT may have inherent variability and inconsistent temporal stability.
ICC and correlations were analyzed for HPT values at the upper trapezius and low back pre- and post- quiet rest during each session to examine reliability for each measure. At the upper trapezius, the ICC and Pearson’s r values indicated good reliability and significant correlations were demonstrated for HPT during Sessions 1 and 2, respectively (ICC3,1 Session 1:= 0.881 and 2=0.734) (r Session 1=0.887, p<0.001 and 2=0.741, p<0.001). In Session 1, the SEM for HPT = 0.85°C with a minimal difference (MD) = 2.36°C. For Session 2, the SEM for HPT of the upper trapezius = 1.51°C and the MD = 4.18°C.
At the low back, good reliability and significant correlations for HPT during Sessions 1 and 2 were demonstrated, respectively (ICC3,1 Session 1=0.840 and 2=0.853)(r Session 1=0.866, p<0.001 and 2=0.869, p<0.001). In Session 1, the SEM for HPT of the low back = 0.99°C, with a MD = 2.74°C. For Session 2, the SEM = 1.03°C and the MD = 2.85°C. HPT after a period of quiet rest demonstrates good reliability with significant correlations among sessions over the low back and trapezius.
PPT Reliability
During Session 1, PPT of the upper trapezius (t(34)=-0.463, p=0.646) and low back (t(34)=-1.534, p=0.134) were not significantly different, with small effect sizes (Cohen’s d = 0.078 and -0.259) for each respective site. This suggests significant changes in pain threshold were not observed for either site after a period of quiet rest. During Session 2, PPT of the upper trapezius (t(34)=-0.73, p=0.942) and low back (t(34)=-0.145, p=0.885) were not significantly different, with small effect sizes (Cohen’s d = -0.012 and 0.025, respectively) for each site, indicating no significant changes in pain threshold for either site after a period of quiet rest. This suggests PPT may demonstrate sufficient temporal stability.
To examine reliability of PPT, ICCs and correlations were analyzed for PPT values at the upper trapezius and low back pre and post quiet rest during each session. For the upper trapezius, the ICC and Pearson’s r values indicated excellent reliability with significant correlations for PPT during Sessions 1 and 2, respectively (ICC3,1 Session 1= 0.873 and 2=0.822)(r Session 1= 0.874, p<0.001 and 2=0.810, p<0.001). For Session 1, the SEM of the upper trapezius = 55.25 kpa, with a MD = 153.15 kpa. For Session 2, the SEM for PPT of the upper trapezius= 75.06 kpa, with a MD = 208.05 kpa.
For the low back, excellent reliability with significant correlations among sessions were demonstrated (ICC3,1 Session 1=0.888 and 2=0.952)(r Session 1=0.889, p<0.001 and 2=0.952, p<0.001). For Session 1, the SEM for PPT of the low back = 85.71 kpa with a MD = 237.58 kpa. For Session 2, the SEM for PPT of the low back = 60.41 kpa with a MD = 167.46 kpa. Table 2 displays descriptive statistics, Pearson’s correlation coefficients, p-values, SEM, and ICC3,1 for HPT and PPT.
EIH Effects
Session 1
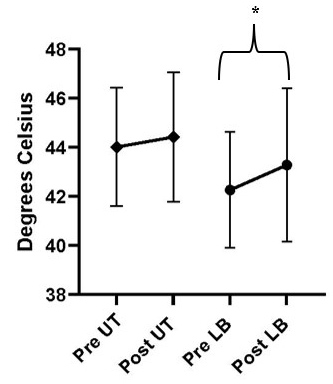
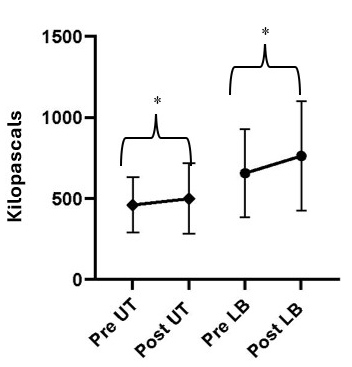
To determine if EIH occurred after the 45-degree Roman Chair, a three-way repeated measures ANOVA examined HPT and PPT changes over the low back and upper trapezius before and after exercise. The three-way interaction effect of time (pre/post exercise) × location (upper trapezius/low back) × condition (HPT/PPT) was significant (F (1, 34) = 9.243, p = 0.002, ηp² = 0.257). A significant increase in HPT was demonstrated in the low back after exercise (F(1, 34)=11.168, p=0.002, ηp²=0.247). There was no significant change observed in HPT of the upper trapezius (F (1, 34) = 3.821, p = 0.059, ηp² = 0.101) after exercise. A significant increase in PPT was observed in the low back (F (1, 34) = 23.952, p<0.001, ηp² = 0.413) and upper trapezius (F (1, 34) = 5.464, p = 0.025, ηp² = 0.138) after exercise. A significant condition × time effect was observed (F (1, 34) = 20.669, p<0.001, ηp² = 0.378), suggesting exercise produced significant hypoalgesia compared to quiet rest. Results for HPT and PPT pre- and post-exercise for the upper trapezius and low back in Session 1 can be found in Figures 2 and 3 respectively. The 45-degree Roman Chair produced significant EIH assessed with HPT and PPT compared to quiet rest.


Session 2
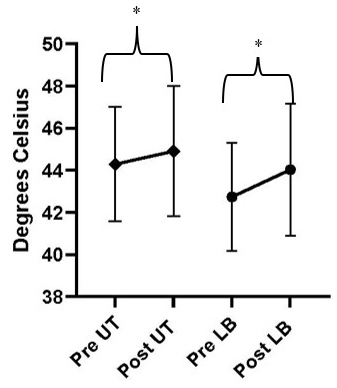
A three-way repeated measures ANOVA was performed to analyze HPT and PPT at the low back and upper trapezius before and after exercise. The three-way interaction effect of time (pre/post exercise) × location (upper trapezius/low back) × condition (HPT/PPT) was significant (F (1, 34) = 9.243, p = 0.005, ηp² = 0.214). There was a significant increase in HPT in the low back (F(1, 34)=156.322, p<0.001, ηp²=0.821) and upper trapezius (F(1, 34)=214.344, p<0.001, ηp²=0.863) after exercise. A significant increase in PPT was observed in the low back (F (1, 34) = 162.188, p<0.001, ηp² = 0.827) and upper trapezius (F (1, 34) = 179.104, p<0.001, ηp² = 0.840). Results for HPT and PPT pre- and post-exercise for the upper trapezius and low back in Session 2 can be found in Figures 4 and 5 respectively. The results from the EIH effects from Sessions 1 and 2 indicate that the 45-degree Roman chair exercise produces local and systemic increases in PPT and local increases in HPT, with inconsistent systemic HPT effects observed across both sessions.


Reliability of EIH
As part of the reliability analysis for HPT post-exercise across sessions, a two-way interaction for session (session 1/session 2) × location (low back/upper trapezius) was not significant (F(1, 34)=0.872, p=0.357, ηp²=0.025), indicating no significant change between sessions 1 and 2. To assess for the reliability of PPT post-exercise between sessions, a two way repeated measures ANOVA was conducted for session × location to analyze PPT values between sessions 1 and 2. The two-way interaction for session (session 1/session 2) × location (low back/upper trapezius) was not significant (F(1, 34)=0.247, p=0.622, ηp²=0.007), indicating no significant change between sessions 1 and 2.
ICC values and correlations were analyzed for the absolute EIH values for HPT and PPT at the upper trapezius and low back between each session to examine between-session reliability. Table 4 displays descriptive statistics, Pearson’s correlation coefficients, p-values, ICC3,1, and SEM to assess the strength and significance among these variables. The results from Table 4 for HPT and PPT revealed good-to-excellent reliability between different body locations. HPT at the upper trapezius (ICC= 0.867) and low back (ICC= 0.903) demonstrate excellent reliability after exercise. Values for PPT showed good reliability at the upper trapezius (ICC= 0.744) and excellent reliability at the low back (ICC= 0.815) after exercise. Good-to-excellent reliability is observed when measuring HPT and PPT after exercising, suggesting EIH effects are reliable between sessions during a 45-degree Roman Chair exercise.
Minimal Detectable Difference (MDD)
For HPT, the MD= 2.91 oC for the upper trapezius and 2.7 oC for the low back. For PPT, the MD= 285.9 kilopascals (kpa) for the upper trapezius and 394.42 kpa for the low back. Four participants reached the MD values for PPT of the low back and 3 participants reached the MDD values for the upper trapezius on an individual basis. Three participants reached the MDD values for HPT of the low back and no participants reached this value for HPT of the upper trapezius when considering individual changes in HPT.
DISCUSSION
The primary aims of this study were to evaluate the reliability of HPT and PPT measures before and after a period of quiet rest to support the presence of EIH observed following the 45-degree Roman chair exercise. Additionally, the study sought to assess the reliability of EIH produced across sessions. The results of this study indicated that while HPT and PPT measures demonstrated good-to-excellent reliability across sessions, there were differences in their measurement stability. Specifically, HPT measures showed significant changes after a period of quiet rest in both the upper trapezius and low back, suggesting potential variability in this measure, while PPT remained stable over time, indicating sufficient stability. Consistent EIH were observed for both measures following the exercise, with significant increases in pain thresholds in both muscular sites. Furthermore, reliability analysis of post-exercise EIH values revealed good-to-excellent consistency between sessions, particularly for HPT and PPT at the low back.
When the reliability of HPT and PPT measures were investigated, both were consistent across sites before and after a period of quiet rest. Both the upper trapezius and the low back demonstrated high correlations (r >0.70) and excellent reliability (ICC>0.75). These results are in agreement with a previous study examining the reliability of PPT after a period of quiet rest, where strong correlations (r >0.95) and excellent reliability (ICC>0.97) were demonstrated in the quadriceps and upper trapezius.11 However, we acknowledge that significant differences were observed at the low back and upper trapezius values for HPT after a period of quiet rest. Despite this, the study adds to the body of literature by including a period of quiet rest to test the within session reliability of both modalities, allowing for greater assessment of measurement stability when assessing HPT and PPT.
When examining the EIH effects, significant increases in HPT and PPT were observed after a 45-degree Roman chair exercise compared to quiet rest. This aligns with existing literature on resistance exercise in a healthy population and its analgesic effects.9,28,29 Specifically, significant increases in PPT were observed over both the erector spinae of the low back and upper trapezius muscles following the exercise, indicating a local and systemic effect across different muscle groups. Larger effect sizes were observed in the low back for both HPT (ηp²=0.247, 0.821) and PPT (ηp² = 0.413, 0.827) across Sessions 1 and 2, respectively. These results are in agreement with a study by Keilman et al., who observed an increase in PPT at local muscle sites in the low back after performing kettlebell swings in healthy participants.30 Similarly, HPT showed significant increases in both the low back and upper trapezius, although not as consistent as PPT, further supporting the exercise’s ability to modulate pain sensitivity. While there are few studies examining HPT after dynamic resistance exercise, the current results align with a previous study from our group, which demonstrated HPT increases at the exercising site after both an upper body and lower body dynamic resistance exercise.7 These increases in HPT specifically support the involvement of the C-fibers in mediating the reduction of pain after a single bout of dynamic resistance exercise.
Finally, to assess the reliability of EIH elicited by heat and pressure stimuli between sessions, post-exercise values from both stimuli were selected for comparison across Sessions 1 and 2, allowing for the evaluation of their consistency between sessions. Good-to-excellent reliability was observed (ICC > 0.73) for both sites with heat and pressure, with significantly greater increases in HPT and PPT in Session 2 than in Session 1. This may be due to the higher number of repetitions performed in Session 2, averaging four more than Session 1. These results contrast with prior research on EIH reliability in healthy individuals, which reported poor reliability for the magnitude of EIH.10 A 2024 systematic review concluded that the test-retest reliability in healthy subjects is insufficient and unreliable between sessions.2,10,31 The poor reliability in these studies may stem from the calculation method used for EIH. While understanding the magnitude of change is clinically important in determining the positive or negative directionality in terms of the efficacy of the intervention, using values that could be negative or positive may impact reliability results. The magnitude of change in the reliability aspect of this study should reflect the absolute size of the difference, not its direction. Using absolute values for change, rather than directional changes, could provide a more accurate reflection of variability and agreement over time. Additionally, the cited systematic review incorporated studies with a broad range in statistical value parameters for kappa, SEM, and ICC, this variability can undermine the consistency and comparability of the findings across studies. Finally, this systematic review did not include any studies specifically for musculoskeletal pain, although it was listed as a key term. Due to the overlooked factors of the most recent EIH reliability literature, by focusing on post-exercise values across sessions, this study provides a clearer picture of changes induced after exercise. This approach will aid clinicians and researchers in better demonstrating the efficacy of their interventions on EIH over time.
Implications for Clinical Practice
The results of this study suggest the 45-degree Roman Chair reliably induces a significant EIH effect local to the exercising muscles in the low back with inconsistent effects systemically. However, these results should be interpreted cautiously as this study was conducted in healthy participants and future trials are needed to examine this effect in individuals with chronic pain. Individuals with chronic pain may display great variability in response to EIH with some demonstrating hyperalgesia.1 Nonetheless, understanding the analgesic effects of the 45-degree Roman chair exercise has potential implications for clinical practice. First, this exercise is novel to the rehabilitation setting and demonstrates the dynamic resistance exercise of the low back may be beneficial. The 45-degree Roman chair is one of the few exercises that can be easily applied in the clinic to progressively overload spinal musculature. Furthermore, the flexion and extension of the spine during this exercise mimics functional movements performed in everyday life. Although this exercise is not a compound movement like the deadlift, an exercise demonstrated to be safe to perform in individuals with low back pain, the Roman chair presents the added benefit of needing less equipment and familiarization.32,33 Second, this study adds to this body of literature by demonstrating there may be favorable benefits in lessening of pain sensitivity when completing the Roman Chair exercise. The significant effect in pain reduction observed in low back after performing this exercise across multiple sessions could make this a viable intervention. Finally, EIH may be reliable across sessions indicating that, not only does this exercise induce hypoalgesia, but it may be used as a practical outcome measure in studies aiming to assess for change in EIH in individuals with low back pain. Incorporating this exercise into rehabilitation protocols could potentially enhance pain management strategies.
Study Limitations
The methodological design of this study with its inclusion of one set for as many repetitions as possible likely impacted reliability due to uncontrolled variability in participants’ training status. While previous studies using the Roman chair have utilized the AMRAP approach, their study design loaded the exercise over time.12 This design may not have been as practical for bodyweight repetitions, as the average of 38 repetitions across both sessions is more indicative of muscle endurance rather than strength. Future studies should employ a design that allows for sufficient fatigue but is not dependent on participants’ physical fitness levels. The authors acknowledge not controlling timing between sessions was also a limitation of the study design.
Additionally, the multifaceted nature of pain perception, influenced by psychological, physiological, and environmental factors, further complicates the measurement of EIH. Therefore, the current study’s findings add to the existing literature by including dynamic resistance exercise and assessing EIH with a multimodal approach. This investigation also highlighted the inconsistencies in interpreting and reporting EIH reliability, underscoring the need for standardized protocols and rigorous methodologies to enhance the reproducibility of EIH research across different populations and conditions. Future studies could include diverse demographic groups and individuals with chronic pain conditions to assess the exercise’s efficacy across different patient profiles. Moreover, while the study focused on acute effects, longitudinal investigations are necessary to examine the long-term benefits of incorporating the 45-degree Roman chair exercise into rehabilitation strategies.
Conclusion
The findings of this study demonstrate that HPT and PPT have excellent reliability when performed before and after a period of quiet rest, allowing for more certainty that increases in pain threshold after exercise are not due to measurement instability. The results of this study also indicate that the 45-degree Roman chair exercise induces significant EIH, as evidenced by increased pain thresholds in both local and systemic sites. Additionally, the good-to-excellent reliability found when examining the magnitude of EIH produced across sessions may be seen as a potential benefit for clinicians hoping to apply dynamic resistance exercise as an intervention, with consistent reductions in pain viewed positively. However, further research exploring the underlying mechanisms of EIH, as well as the long-term effects of this exercise modality is recommended to optimize its therapeutic application.
Data availability statement
Data set available upon request.
Conflict of Interest Disclosure
The authors report there are no competing interests to declare.