BACKGROUND
Reinjury rates of up to 28% after primary anterior cruciate ligament reconstruction (ACLR) have been reported among individuals returning to high levels of physical activity and sports.1,2 Quadriceps weakness is associated with an increased risk of second ACL injury,3–5 altered gait and biomechanics,6–10 poor self-reported outcomes,4,11–15 and cartilage degeneration.16–18 Consequently, restoring quadriceps strength is a focal point of ACLR rehabilitation, but presents a significant rehabilitative challenge as evidenced by continued quadriceps weakness at six to 12 months post-ACLR. In a review of 37 studies, Lepley et al. reported an average quadriceps strength deficit of 23% ± 8% at six months, and 14% ± 6% at 12 months, with only five studies meeting clinical recommendations for strength at six months, and only nine studies meeting clinical recommendations for strength at 12 months.13 Therefore, identification of early post-operative measures of quadriceps muscle performance that can predict quadriceps strength and functional outcomes in the late stages of rehabilitation is of clinical importance. This can facilitate targeted clinical interventions in the early stages of rehabilitation and better inform return to sport (RTS) decision making.
Maximum quadriceps strength is the most often quantified measure of neuromuscular function after ACLR,19 and in addition to hop testing, is also the most cited objective test utilized in RTS testing.20 Early measures of quadriceps isometric and isokinetic performance are also moderately correlated with quadriceps strength in the late stages of rehabilitation. McHugh et al. found that isometric quadriceps strength measured at 30° flexion at five weeks post-ACLR was moderately correlated with residual isometric quadriceps weakness at six months post-ACLR.21 Giampetruzzi et al. examined adolescents post-ACLR and identified that three-month post-operative isometric quadriceps peak torque predicted 37% of the variance of isokinetic quadriceps peak torque at six months.22 A moderate positive correlation between the limb symmetry index (LSI) of isokinetic knee extension at three and six months post-ACLR in subjects with hamstring grafts has also been reported.23 The LSI defined as the ratio of the isokinetic knee extension strength of the operated limb to that of the non-operated limb, expressed as a percentage.23 Hannon et al. reported isokinetic quadriceps strength at three months accounted for 47% of the variance in quadriceps strength at time of return to sport in adolescent patients.24 Given this context, early strength measures have historically explained only a limited amount of the variance in quadriceps strength during the late rehabilitation stages. Furthermore, despite ongoing efforts to develop quadriceps strength in the early stages of rehabilitation, deficits persist in the later stages. This suggests the potential for incorporating other trainable measures during early rehabilitation that may also impact late-stage quadriceps strength.
Maximum strength or peak torque alone does not provide a complete understanding of muscular performance. Rate of torque development (RTD) has been proposed as an assessment to evaluate quadriceps strength after ACLR.25–30 RTD is force production per unit time, which reflects the torque generated by a muscle during the initial phase of muscle contraction.31 Quadriceps RTD is crucial because functional sporting movements like sprinting, kicking, cutting, and jumping require shorter contraction times than maximal quadriceps peak torque, which takes more than 300ms to develop.32 Similar to quadriceps weakness, authors have shown that RTD is also reduced at three months,26 six months,27,28,33 and nine to12 months post-ACLR.30
Early measures of quadriceps RTD have been shown to predict functional measures used for RTS decisions in the late stages of rehabilitation.26,34,35 RTD and quadriceps strength are highly correlated at six weeks post-ACLR and are complementary but distinct predictors of hopping and jumping performance at six months post-ACLR, with RTD more strongly associated with vertical jump height and vertical ground reaction force.34 Quadriceps RTD limb symmetry index during serial testing at four, six, and nine months post ACLR was more strongly associated with the recovery of knee biomechanics during running than strength at two years after surgery.36 Early RTD measures may predict late-stage quadriceps strength, given that RTD is distinct yet related to quadriceps peak torque,35,37–40 is associated with late rehabilitation functional measures, and is trainable early in rehab. However, it is currently unknown whether early measures of quadriceps isometric RTD post-ACLR correlate with quadriceps isokinetic peak torque measures in the late stages of rehabilitation.
Therefore, the purpose of this study was to examine the correlation between quadriceps RTD values at four months post-ACLR and quadriceps isokinetic peak torque values at six months post-ACLR. Identification of clinically modifiable predictors of quadriceps strength during the early phases of rehabilitation could improve treatment outcomes. It was hypothesized that isometric RTD at four months would be significantly correlated with isokinetic peak torque at six months post-ACLR. A secondary hypothesis was that the involved limb RTD would be significantly slower than the uninvolved limb at four months post-operative.
METHODS
Participants
This retrospective case series was approved by the university’s institutional review board. The electronic medical records of patients who underwent unilateral ACL reconstruction and subsequent post-operative rehabilitation at one center from September 15th, 2018 to December 30, 2020 were searched. Patients were included if they were 13-55 years old, underwent unilateral ACL reconstruction with or without concurrent meniscus repair/meniscectomy at one institution, and received subsequent post-operative rehabilitation at the same institution’s rehabilitation clinic. Patients were excluded if they did not undergo both post operative isometric and isokinetic quadriceps strength testing. All patients went through a post-operative rehabilitation program that included controlled weight bearing based on post-operative weightbearing restrictions, knee range of motion, lower extremity motor control training and progressive strength training with emphasis on quadriceps strength, and neuromuscular training. The information collected included patient’s age, height, mass, date of surgery, surgeon, sport activity, and operative report surgical details. The research team determined if there was complete patient testing data and if the patient met the inclusion criteria for the study.
Procedures
Quadriceps RTD, peak isometric torque at four months, and quadriceps isokinetic peak torque at six months were assessed using a single HUMACNORM (CSMi, Stoughton MA) isokinetic testing machine. Patients were tested in a seated position with hips at 90° flexion with straps placed across their chest, waist, and distal femur for stability. The pad of the testing apparatus was set anteriorly on the distal tibial just proximal to the malleoli. Isometric testing was performed in either 60° (n=19) or 90° (n=28) of knee flexion, based on therapist preference. Rate of torque development and isometric peak torque values for the injured side for these two positions were not found to be significantly different, so the data were used from both positions. A 10-second effort was recorded to capture both rate of torque development and peak torque per clinic protocol. One submaximal trial followed by two 10-second maximal isometric knee extensions were completed as per clinical protocol. Subjects were familiar with this isometric activation approach on the HUMACNORM device as isometric training was used in the same way as testing during their formal rehabilitation before testing. Therefore, it was felt that one submaximal trial was enough for familiarization to the testing procedure. Patients were instructed to extend their knee as quickly and forcefully as possible with strong verbal encouragement provided during testing to capture rate of torque development measures. Real time feedback via a force time curve was available for patients to view during the test to give further motivational feedback. Subjects were given 30 seconds of recovery between maximal trials. Isokinetic testing was performed through an arc of motion 90°-10° from full extension with the same instructions as isometric testing. Four submaximal repetition warmups at both 60°/sec and 180°/sec followed by the performance of maximal isokinetic knee extensions at 60°/sec (5 reps) and 180°/sec. (15 reps).
Data Processing
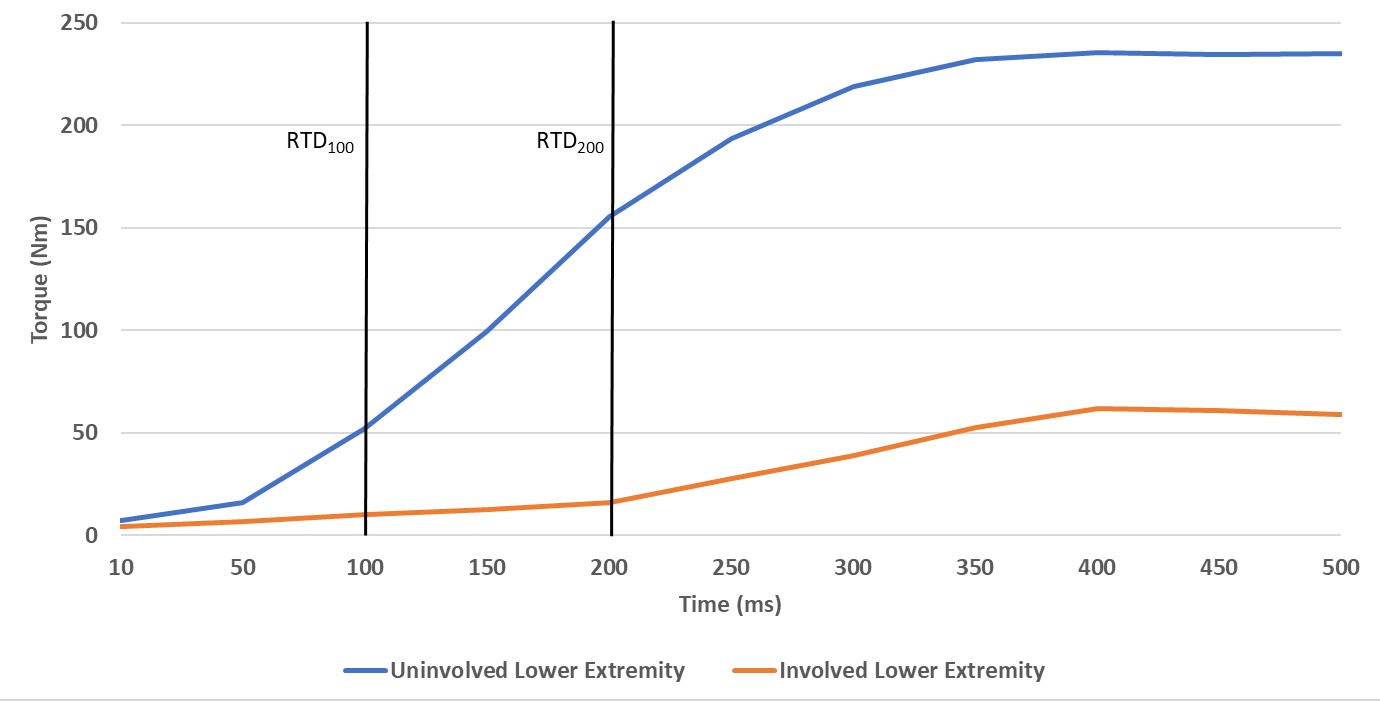
The isometric torque raw data was collected at 100Hz from the Humac software and was exported into .csv files. A template was developed in Excel (Microsoft, Redmond, WA) to analyze the data using the slope function to calculate “early” rate of torque development from 0-100ms (RTD100) during knee extension. The zero time point was indicated when the torque curve exceeded 1 Nm. The same function was used to calculate “late” rate of torque development from 100-200ms (RTD200) during knee extension. RTD100 and RTD200 were selected as peak RTD has been shown to occur during the first 200ms of muscular contraction.34 RTD from these time windows also reflects the demand of most explosive sport specific tasks and captures the primary contributions to rapid force production.35 Further, these physiologic contributors to rapid force production have been shown to have different levels of influence on early vs. late RTD.31,37,41–46 Several studies examining similar constructs have also utilized the same timeframes.27,29,35,37 The average of the two trials was used and the units of RTD was Nm/second. The max function in excel was used to determine the peak knee extension isometric force reached during the 10 seconds of data collection. The average peak torque of the two trials were recorded in Newton-meters. Isometric measures occurred at approximately four months post-surgery. Isokinetic knee extension peak torque at 60°/sec and 180°/sec was recorded from the summary report into an Excel database created for this study. Isokinetic testing occurred at approximately six months post-surgery.
Data Analysis
All analysis was performed using SPSS version 27. Data were evaluated for normal distribution using a Shapiro-Wilk test and found not to be normally distributed. Therefore, median and interquartile ranges were calculated to describe the data for rate of torque development, isometric and isokinetic peak torque values. Data that is not normally distributed is presented in this manner to describe the skewed data more accurately. As the data did not meet criteria for normal distribution, Spearman’s rho correlations were utilized to determine the level of correlation between the injured limbs’ four-month isometric RTD100, RTD200, and peak isometric torque to the injured limb’s six-month isokinetic peak torque at 60°/sec and 180°/sec. Effect sizes were classified as < 0.3 (weak), ≥ 0.3 to < 0.5 (moderate), and ≥ 0.5 (strong).47 Wilcoxon Signed Rank paired comparison was used for RTD100 and RTD200 between limbs with significance set at p ≤ 0.05.
RESULTS
The final sample of patients included 47 patients out of a possible 87 patients that were screened, and the demographic information, surgical procedures, and sport involvement are described in Table 1. The patient’s mean Tegner activity scale score was 6.5 ± 1.6, with the majority of patients involved in interscholastic cutting sports. The patient’s average time to isometric testing was 4.0 ± 1.1 months. The patient’s average time to isokinetic testing was 6.7 ± 1.5 months.
The descriptive data for all strength measures, presented as median and interquartile values, is provided in Table 2. The Spearman rho correlations revealed significant correlations (p ≤ 0.001) between the isometric four-month measures and the isokinetic measures at six-months (Table 3). RTD100 demonstrated a strong positive correlation with isokinetic peak torque at 60°/sec (ρ = 0.54) and a moderate positive correlation at 180°/sec (ρ = 0.45). RTD200 demonstrated strong positive correlations with isokinetic peak torque at both 60°/sec (ρ = 0.63) and 180°/sec (ρ = 0.52). The RTD100 of the uninvolved limb median (interquartile range) was 235.3 Nm/s (148.3, 347.4) compared to the involved limb 136.5 Nm/s (74.9, 237.2) at four months (p <0 .001). The RTD200 uninvolved limb was 238.6 Nm/s (166.9, 443.7) compared to the involved limb 132.6 Nm/s (63.3, 185.4) at four months (p< 0.001). An example of one subject’s differences in force time curves between legs is represented in Figure 1.

DISCUSSION
To the authors’ knowledge, this is the first study to demonstrate a moderate to strong correlation between quadriceps isometric RTD at four-months post-ACLR and quadriceps isokinetic peak torque at six months post-ACLR. All measures of quadriceps RTD at the four-month visit post-ACLR were significantly correlated with the six-month measure of quadriceps isokinetic peak torque at both 60°/sec and 180°/sec, with stronger correlations seen at 60°/sec. This suggests that early measures of quadriceps isometric RTD can serve as a partial predictive marker for later quadriceps strength outcomes. The secondary hypothesis was supported as all four-month measures involved in lower extremity RTD were at least 40% lower than the uninvolved lower extremity.
The best predictors of isokinetic peak torque were found to be four-month peak torque and RTD200. Isometric peak torque demonstrated a strong positive correlation with isokinetic peak torque at 60°/sec (ρ = 0.771), with RTD200 also demonstrating a strong positive correlation at 60°/sec (ρ = 0.629). These findings lend further support to the existence of a positive relationship between maximum strength and the ability to rapidly generate force.37,39 They also have implications on early phase rehabilitation strategies designed to mitigate quadriceps weakness in the later stages of rehabilitation. At both isokinetic peak torque speeds, RTD200 was more strongly correlated to six-month peak torque than RTD100. The difference in correlation strength is expected when examining the specific physiological factors responsible for RTD at these time intervals and their associations with maximum strength. RTD100 has been shown to be primarily affected by muscle fiber type and neural factors including motor unit recruitment, firing frequency, and neural drive.31,37,41–46 In contrast, RTD200 is more affected by maximum volitional contraction force, muscle size, and muscle tendon complex stiffness.37,41 Additionally, the factors influencing RTD200 have stronger associations with maximum strength compared to those affecting RTD100. Both RTD200 and maximum strength are affected by muscle cross sectional area and efferent motor outflow. Anderson et al. found that maximal muscle strength accounted for 80% of the variance in volitional rate of force development (RFD) during contraction time intervals of 150-250ms, while RFD during early time intervals (< 50ms) was only moderately related to evoked muscle contractile properties and maximal volitional contraction.37 Anderson37 measured RFD, which is the rate at which an individual can generate linear force, as opposed to RTD, which measures rotational force. However, strong correlations have been shown between RFD and RTD, supporting the influence of muscular strength on torque application.48,49
Quadriceps RTD of the involved lower extremity was 40-42% slower than the uninvolved lower extremity at four months. This finding supports the second hypothesis and adds to the growing evidence of reduced quadriceps RTD during early post-operative ACLR rehabilitation from three to six months.26–28,33,35 Additionally, the current study identified that at four months RTD LSI deficits in all measures were greater than peak torque deficits; RTD100 LSI was 58 % and RTD200 was 55.6%, while peak torque LSI was 67.9%. These findings are consistent with Knezevic et al. who noted greater asymmetries in isometric RTD at four months post-ACLR with similar LSI values of 58% for RTD50 and RTD150, 57% for RTD250, and 68% for peak torque.28 This suggests that at four months post-ACLR, the ability to rapidly generate force is more impaired than the ability to generate maximal force.28 Further, the results of the current study indicate significant reductions in both early and late phase RTD, which is also in agreement with studies showing reductions in both phases of RTD (RTD50, RTD100, RTD150, RTD200, RTD250) at similar post-operative ACLR timepoints of three to five months.26,28,35 These reductions at both time intervals indicate that ACLR negatively impacts neural-mediated mechanisms, as well as muscular composition and contractile properties, with these reductions being particularly evident in the early stages of rehabilitation.
Clinically, the significant correlation between quadriceps isometric RTD in the early phases of rehabilitation and later isokinetic peak torque underscores the potential for early intervention strategies to enhance quadriceps strength and rehabilitation outcomes. Quantification of quadriceps strength deficits early in rehabilitation followed by targeted interventions are paramount in ACLR rehabilitation. Traditional strength training utilizing heavy loads >/= 75% of a one-repetition maximum have been shown to be effective in improvements in both RTD and maximum strength31 and are utilized in ACLR rehabilitation. However, utilization of such a training intensity is not feasible to drive quadriceps strength in the early stages of rehabilitation. Considering that the current study has demonstrated that RTD is reduced following ACLR and is related to future strength, and given that other studies have identified methods beyond progressive overload to enhance RTD, it may be clinically advisable to focus on improving RTD early in rehabilitation to improve quadriceps strength. Evidence suggests that maximal intentional force development during exercise is the most efficient training modality, regardless of the training load used, to maximize gains in force production rate and muscle activation at contraction onset.50 Further, strong relationships have been shown in RFD/RTDpeak, RFD/RTD0–100, and RFD/RTD0–200, and indicate that the ability to develop force or torque rapidly (i.e., RFD/RTD) was transferable when measured during knee extension, isometric mid-thigh pull (IMTP), or sprint cycling.48,49 It therefore appears plausible to incorporate intentional rate-based training into exercises commonly completed in early stages of ACLR rehabilitation once initial exercise form and technique are mastered and prior to resistance training using heavier loads. Quadriceps isometric exercises such as seated knee extension or IMTP completed in a fast manner, or completion of early closed chain exercises such as squats, step ups, or step downs with the intent to move fast during concentric or eccentric quadricep activation phases all serve as viable clinical examples. The key is that the patient must intend to activate the muscle or move as fast as possible as this is more important than the actual movement velocity or focusing on the force achieved.51–54
This study has several limitations. Quadriceps muscle performance testing was completed at four months and six months post-ACLR and results at different time points may have altered results. Further, all subjects completed post-operative rehabilitation in the same sports clinic utilizing the same rehabilitation protocols and thus different protocols could lead to different results. Finally, this was a retrospective study in which two knee flexion angles of 60° and 90° were utilized during isometric quadriceps testing based on therapist preference, which could affect comparison of findings between subjects. However, studies have shown that both knee flexion angles of 60°22,54,55 and 90°13,14,25,27,36,56,57 have consistently been utilized in isometric quadriceps strength and RTD assessment in subjects post-ACLR. Furthermore, in healthy subjects, studies have revealed that peak extensor torque values were similar in magnitude at 60° and 90° of knee flexion and that side-to-side knee extensor torque ratios at 60° and 90° of knee flexion were not significantly different, suggesting that testing at either of these respective angles is defendable.58,59 Conversely, a study by Hsiao et al. did show some differences in isometric quadriceps testing at 50°, 70° and 90° degrees at three months post-ACLR.60 However, it was not reported whether these differences were significant, and data were collected from a small number of ACLR subjects. It remains unclear whether RTD differences exist at these testing angles, given the prior studies reported on peak torque measurements.
CONCLUSION
The results of this study provide evidence supporting the use of quadriceps isometric RTD at four months post-ACLR as a partial predictor of quadriceps isokinetic peak torque at six months post-ACLR. These findings contribute to the growing body of evidence emphasizing the clinical importance of early quadriceps performance measures in ACLR rehabilitation. Given that RTD assessments can be clinically challenging to complete and not fully integrated in standard assessment guidelines, future research should continue to explore the relationship between early RTD measures and long-term functional outcomes, as well as investigate the effects of early rehabilitation RTD interventions on quadriceps strength in late-stage rehabilitation and at the time of return to sport.
Conflicts of interest
The authors report no conflicts of interest related to this work.