


INTRODUCTION
Hip muscles are essential for lower extremity stability and postural control.1,2 Deficiencies in hip strength have been linked to various musculoskeletal pathologies (e.g., anterior cruciate ligament sprain,3,4 patellofemoral pain,5,6 chronic ankle instability7,8); hence, objective assessments of hip strength are widely performed in both clinical and laboratory settings.9,10 While an isokinetic dynamometer (IKD) is regarded as the “gold standard” for assessing hip strength,9,11 it is often impractical for clinical use due to its cost, lack of portability, and the need for substantial space. As an alternative, portable dynamometers (PD) are used in clinical practice as a reliable and valid testing option for evaluating hip strength.9,12
One important aspect of muscle capacity is the ability to generate torque rapidly, known as the rate of torque development (RTD).13 This concept has gained attention in the literature14,15 because RTD, which accounts for the time-dependent characteristics of muscle contraction, shows stronger associations with daily and sport activities than traditional peak isometric strength measures.13 Recent evidence supports the importance of RTD in pathological conditions, demonstrating that lower hip RTD, but not strength, has been associated with greater lower extremity frontal plane projection angles during functional tasks in individuals with patellofemoral pain.16 Given that RTD can be calculated from a maximal voluntary isometric contraction,17,18 assessing RTD using a PD appears feasible in clinical practice. Based on previous evidence,13,19,20 an in-depth analysis of RTD, distinguishing between the early (e.g., RTD0-100_ms) and late (e.g., RTD100-200_ms) phases, may provide insights into more specific neuromuscular impairments, such as motor unit recruitment and muscle fiber type. Clinicians may consider incorporating fast-velocity concentric and eccentric resistance training to address deficiencies in early-phase RTD,21,22 while non-explosive high-intensity resistance training for improvements in late-phase RTD.20
Current literature recommends the belt-stabilized PD method since the assessor’s sex or strength can influence PD assessments.23,24 The belt-stabilized PD can be performed through two different methods: the push (PDpush) and pull (PDpull) methods.25 The PDpush method entails placing the PD directly on the individual’s body, whereas the PDpull method positions the PD against the back of a stationary object (e.g., treatment table) to measure force by the individual exerting pressure against the rigid structure. The PDpull method has previously exhibited greater validity and offered more comfortable performance (i.e., less perceived patient discomfort) for assessing knee extension strength than the PDpush method,25 indicating that the choice of fixation method could affect the assessment outcomes. Some studies26–28 suggest that the PD can be a valid tool for measuring hip strength and RTD; however, there is no research on the validity between the two different fixation methods (PDpush vs. PDpull) and how these measurements compare to the absolute values obtained by IKD. Evidence shows that PD often overestimates hip strength values compared to those measured by the IKD.29,30
The primary purpose of this study was to determine the validity and agreement of hip abduction and extension isometric strength and RTD measurements using an PD with two different fixation methods (PDpush or PDpull) in comparison with an IKD. The secondary purpose of this study was to compare the level of discomfort among the three different assessment methods (PDpush vs. PDpull vs. IKD). It was hypothesized that an PD would be a valid tool for assessing hip strength and RTD, with the PDpull method demonstrating strong validity and the PDpush method showing moderate validity while its assessments would yield higher values than those obtained from IKD. It was also hypothesized that the IKD would be more comfortable than both the PDpush and PDpull methods, with the PDpull method being more comfortable than the PDpush method.
MATERIALS AND METHODS
This was a cross-sectional study reported according to the Standards for Reporting Diagnostic accuracy studies (STARD) guidelines.31 The independent variables were the device and fixation method (PDpush, PDpull, and IKD). The dependent variables were hip (abduction and extension) neuromuscular function (strength and RTD) and level of discomfort.
Participants
A priori sample size calculation was performed using G*Power software (version 3.1.9.6; Universität Düsseldorf, Düsseldorf, Germany). The effect size was estimated based on a previous study32 that investigated the validity of knee extension RTD assessment using an PD. To achieve a power analysis with an α=.05, β=.20 (80% power), and a one-tailed test, a minimum of 20 participants were necessary for this study.
Twenty healthy, physically active individuals were recruited from a local university and surrounding community via flyers and advertisements between March 2024 and May 2024. To be eligible for participation in this study, participants had to (1) be between the ages of 18 and 35 years and (2) self-report engaging in physical activity of moderate-to-vigorous intensity for at least 30 minutes per day on a minimum of three days per week. Participants were excluded if they had (1) a history of low back or lower extremity surgery; (2) low back or lower extremity injury or pain within the prior six months; or (3) were diagnosed neurological or cognitive impairment. Participants were verbally instructed to refrain from lower extremity resistance training 24 hours before testing. The study was approved by the University of Connecticut Institutional Review Board, and written informed consent was obtained from all participants.
Procedures
Once the eligibility screening and informed consent were completed, the participants’ age, height, and mass were obtained. Current physical activity levels were then assessed using the Tegner Activity Scale, a reliable and valid single-item questionnaire that measures sport and work activity levels.33 The Tegner Activity Scale ranges from 0 to 10, with 10 being the most active.33 Prior to testing, participants were asked to wear comfortable clothing. The dominant limb, defined as the limb used to kick a ball, was evaluated for all testing. A single assessor (XX) with eight years of experience conducting strength and RTD assessments with IKD and PD completed all data collection.
All participants underwent maximal voluntary isometric contractions of hip abduction and extension using an IKD (Biodex System Pro 4; Biodex Medical Systems Inc., Shirley, NY) (Figure 1), followed by assessments using an PD (microFET2; Hoggan Scientific LLC., Salt Lake City, UT) (Figure 2). All devices were calibrated at the beginning of the study following the manufacturer’s operational guidelines to ensure accurate measurements throughout the study. Data was collected between April 2024 to May 2024.
_hip_abducti.jpeg)

The testing order for hip muscle groups (extension and abduction) and fixation methods for PD (push and pull) was randomized by a coin toss. A coin toss was conducted in two stages: first to determine the muscle group, followed by a second toss to select the fixation method. To familiarize themselves with the muscle contractions, participants performed a series of gradual warm-up sessions, involving three-second isometric contractions at 50%, 75%, and 100% of their self-perceived effort.18 Each level of exertion was performed only once, with a one-minute rest between each level. No additional warm-up activities were permitted to minimize fatigue. After completing the warm-up, participants were given a rest period of up to three minutes before the testing began. Subsequently, participants were instructed to exert maximal force as hard and fast as possible for actual data collection. Standardized verbal encouragement was also provided during each trial to elicit their maximum effort. The assessments consisted of three trials with five-second maximal contractions, with participants given a one-minute rest period between trials and a five-minute rest period between testing positions. We confirmed verbally that participants were not experiencing perceived fatigue immediately before each trial; and, additional rest periods were provided if necessary to ensure they could perform the subsequent trial with maximum effort. Following each trial, participants were asked to rate their level of discomfort related to the placement of the PD or IKD by drawing a vertical line on a 10 cm visual analog scale (VAS: 0=no discomfort; 10=worst discomfort imaginable). They were carefully instructed to exclude any discomfort related to muscle soreness during maximal force exertion.
IKD Assessment
The prone position for hip extension and the side-lying position for hip abduction were used, which provide reliable and consistent measurements of hip muscles.9
For the hip abduction measurement, participants were placed in a side-lying position, with the testing limb placed on top of the non-testing limb at 20° of hip abduction supported by the IKD (Figure 1A).34 To minimize accessory motions, the non-testing limb and trunk were stabilized with straps. The axis of rotation was aligned anteriorly to the anterior superior iliac spine at the level of the greater trochanter of the testing limb. The center of the lever arm was positioned at a point 5 cm above the lateral femoral condyle. Participants were instructed to raise their testing limb towards the ceiling with maximum force and speed.
For the hip extension measurement, participants were placed in a prone position, with both the hip and knee of the testing limb in 90° of flexion (Figure 1B).34 The non-testing limb was comfortably supported on a stool with a cushion. To minimize accessory motion, participants were instructed to warp their arms around the chair of the dynamometer, and their trunk was stabilized with straps. The axis of rotation was aligned with the greater trochanter on the testing limb. The center of the lever arm was positioned at 5 cm above the popliteal fossa. Participants were instructed to kick their testing limb back with maximum force and speed.
For both measurements, participants were instructed to start from a fully relaxed state. Colored stickers were applied to mark both the axis of rotation and the point of resistance to ensure a consistent lever arm for PD assessments. Considering potential sticker movement, anatomical landmarks were confirmed prior to each trial to precisely detect the axis of rotation. The distance between markers was measured using a standard tape measure to determine the lever arm length (m).
PD Assessment
Participants conducted the PD assessments using a treatment table, and all methods were consistent with those employed during the IKD assessment. For the PD assessments, stabilization straps (i.e., gait belts) were utilized to secure the PD and stabilize participants’ non-testing limb and trunk. The belt length was adjusted to achieve the same joint angles as in the IKD assessment at the participant’s hip during maximal abduction (Figures 2A and 2B) and extension (Figure 2C and 2D), as measured using a goniometer.
During hip abduction measurements, the assessor supported the participant’s limb to counteract gravity, ensuring participants remained fully relaxed without exerting any effort to lift their limbs. During hip extension measurements, with the hip flexed at 90°, the thigh’s orientation was aligned parallel to gravity, omitting the need for any support from the assessor. However, since the PD’s force threshold was 10 N, participants were instructed to apply a minimum pre-tension before starting the assessment, while still being advised to maintain a relaxed state as much as possible prior to trials.
For the PDpush method (Figure 2A and 2C), the PD was placed directly on the participant’s body and positioned at the location where resistance pads were used during the IKD assessments. During the PDpush method, force was measured by pushing the PD against the gait belt as participants abducted or extended their hips. For the PDpull method (Figure 2B and 2D), the PD was situated against the back of the treatment table, employing the same level of positioning as in the PDpush method. During the PDpull method, force was measured by compressing the PD against the table as participants abducted or extended their hips. A flat attachment was used for both fixation methods.
Data Processing
The IKD was interfaced with a data acquisition system (Noraxon USA Inc., Scottsdale, AZ) and recorded at a sampling rate of 1500 Hz. The PD, with a fixed sampling frequency of 100 Hz, wirelessly transmitted force signal data to a laptop computer via a manufacturer-supplied USB receiver using ergoPAK software (version 2.2.1; Hoggan Scientific LLC., Salt Lake City, UT).
Since the PD measures force (N), torque (Nm) was calculated by multiplying the force (N) by the lever arm (m). For hip strength data, peak torque was obtained from maximal voluntary isometric contractions and then normalized to body mass (Nm/kg). The RTD data were computed using custom MATLAB code (MathWorks Inc., Natick, MA), which calculated the slopes within two different time intervals: (1) RTD0-100_ms (early phase) and (2) RTD100-200_ms (late phase).35,36 Each slope value was then normalized to each time interval and body mass (Nm/s/kg). Three trials of hip abduction and extension strength and RTD were averaged for each testing condition, and the average was used for analysis.
The average level of discomfort (cm) recorded across the three trials of hip abduction and extension RTD for each testing condition was also calculated.
Statistical Analysis
Descriptive statistics (mean ± standard deviation) were calculated for all variables. Data were inspected for normality using Shapiro-Wilk tests. Concurrent validity was assessed using Pearson r or Spearman ρ correlation coefficients where appropriate. The strength of the correlations was interpreted as weak (<0.40), moderate (0.40-0.70), and strong (>0.70).37 Agreement between methods was assessed using Bland-Altman plots with mean differences ± 95% limits of agreement (LOA). Root mean square error (RMSE) and mean difference were also calculated to assess the overall magnitude of error and identify any systematic differences between the measurements. Differences in hip strength, RTD and level of discomfort among the three different testing conditions (PDpush vs. PDpull vs. IKD) were determined using repeated measures analysis of variance (ANOVA) or Friedman tests, based on normality. Relevant post-hoc tests (paired t or Wilcoxon signed-rank tests) were performed in the presence of significant findings, to determine differences between testing conditions. All correlation analyses, repeated measures ANOVA, Friedman tests, and post-hoc tests were conducted in SPSS (version 29.0; SPSS Inc., Chicago, IL), with an a priori alpha of p < 0.05. Bland-Altman plots with mean differences ± 95% LOA were calculated using Microsoft Excel 2018 (Microsoft Corp., Redmond, WA).
RESULTS
Participant demographics are presented in Table 1. All strength and RTD data were normally distributed (p>0.05), except for hip extension RTD0-100_ms (p=0.013). None of the discomfort level data were normally distributed (p<0.05).
Validity
Significant moderate-to-strong correlations were found between PD (both PDpush and PDpull methods) and IKD for all hip strength (r=0.46-0.73; p<0.05) and RTD (r=0.45-0.73, ρ=0.80; p<0.05) measures (Table 2). The PDpull method demonstrated strong correlations for hip abduction RTD0-100_ms and hip extension strength and RTD100-200_ms (r=0.70-0.73; p<0.001), whereas the PDpush method showed moderate correlations (r=0.45-0.58; p<0.05) (Table 2).
Agreement
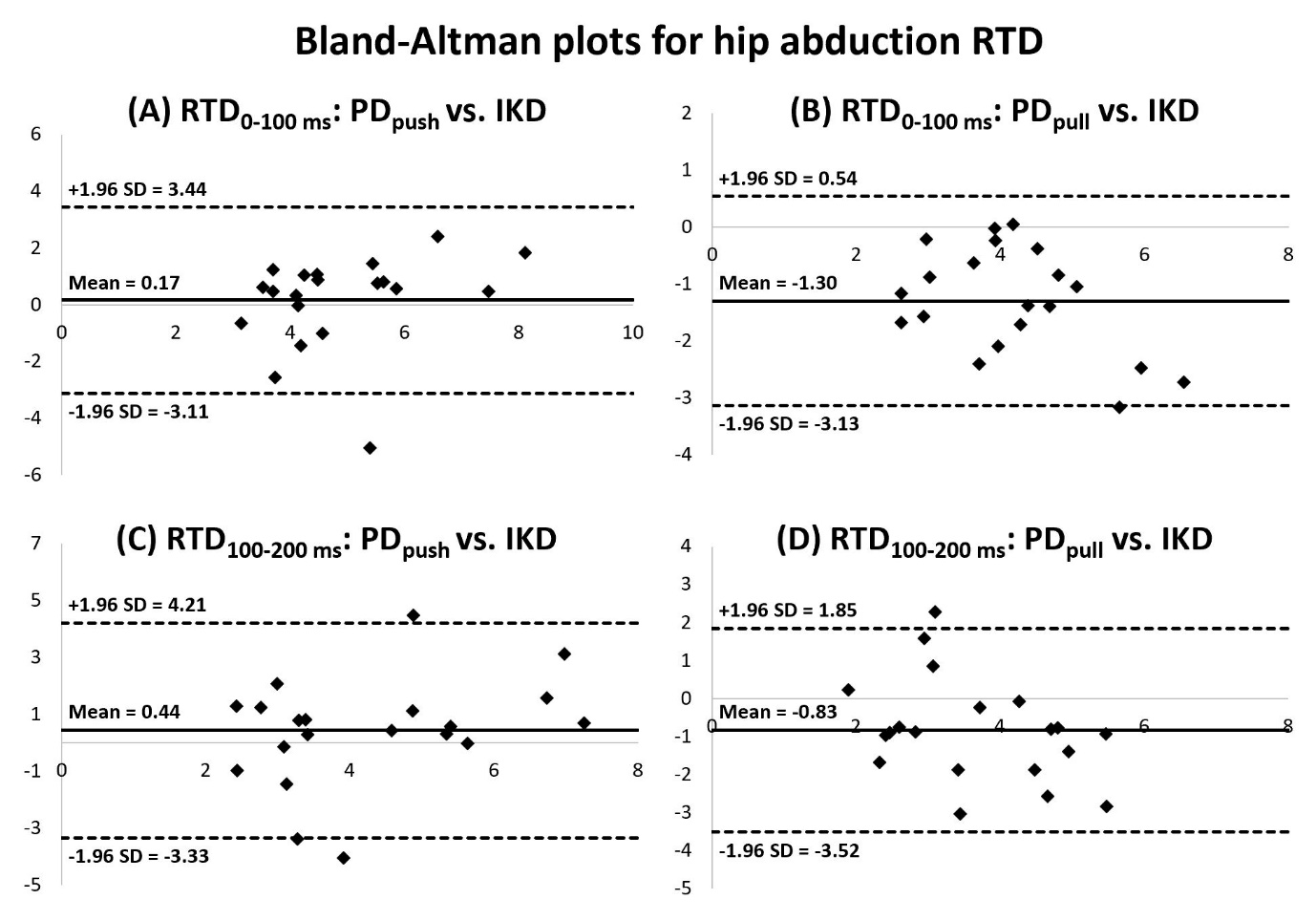
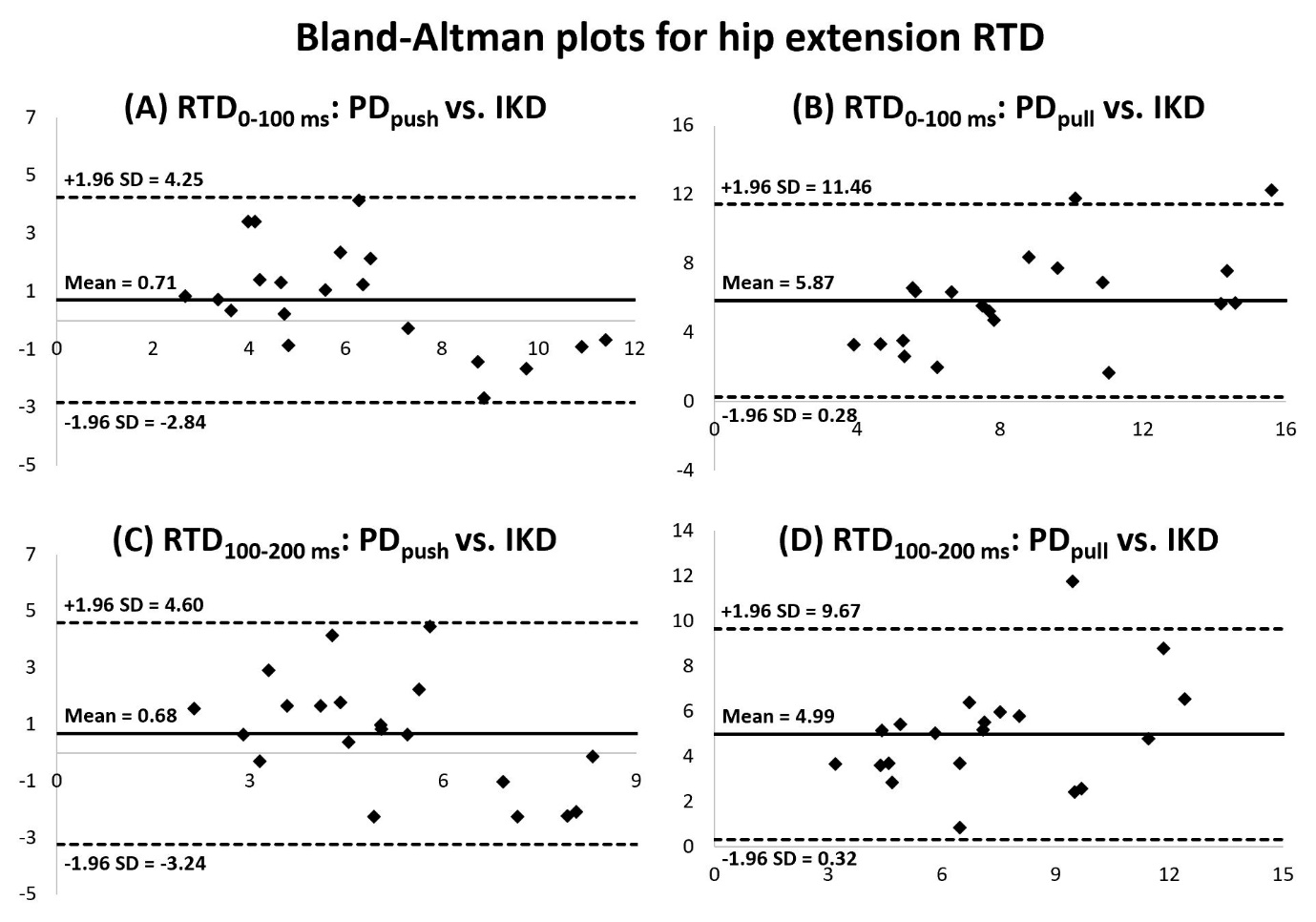
Bland-Altman plots with mean differences ± 95% LOA indicated that the PDpush method overestimated all hip abduction and extension strength (0.35±0.27 to 0.48±0.41 Nm/kg; Figure 3) and RTD (0.17±1.67 to 0.71±1.81 Nm/s/kg; Figures 4 and 5). The PDpull method overestimated hip abduction and extension strength (0.13±0.23 to 1.89±0.64 Nm/kg; Figure 3) but had mixed results for RTD, either underestimating hip abduction RTD (-1.30±0.94 to -0.83±1.37 Nm/s/kg; Figure 4) or overestimating hip extension RTD (4.99±2.39 to 5.87±2.85 Nm/s/kg; Figure 5).



There were significant differences in hip strength and RTD among the three testing methods (p≤0.017; Table 2). Both the PDpush and PDpull methods resulted in significantly greater hip abduction and extension strength compared to IKD (p≤0.017; Table 2). The PDpull method resulted in significantly lower hip abduction RTD (RTD0-100_ms: p<0.001; RTD100-200_ms: p=0.014) and greater hip extension RTD (RTD0-100_ms: p<0.001; RTD100-200_ms: p<0.001) compared to IKD (Table 2); yet, there were no significant differences in any hip RTD measures between the PDpush method and IKD (p>0.05; Table 2). RMSE and mean difference between the measurements are provided in Supplementary Material 1.
Level of Discomfort
No significant differences in the level of discomfort were observed for both hip abduction (p=0.18) and extension (p=.027) measures among the three testing methods (Table 3).
DISCUSSION
The purpose of this study was two-fold: (1) to determine the validity and agreement of hip abduction and extension strength and RTD using an PD with two different fixation methods (PDpush or PDpull) in comparison with an IKD and (2) to compare the level of discomfort among the three assessment methods (PDpush vs. PDpull vs. IKD). These findings indicate that the PD provides valid measures of hip strength and RTD, with the PDpull method demonstrating strong validity for specific measures. However, the absolute values did not show concordance between the PDpush or PDpull and the IKD. There were no significant differences in the level of discomfort among the assessment methods.
Moderate-to-strong correlations were found between the PD and IKD for hip abduction and extension strength measures (r=0.46-0.73), consistent with earlier findings (r=0.42-0.84).29,38,39 Similarly, the current study found moderate-to-strong correlations between the PD and IKD for all hip abduction and extension RTD measures (r=0.45-0.73, ρ=0.80), regardless of the PD fixation methods. The validity of our PDpush method, showing moderate-to-strong correlations, aligns with a recent study.26 Another study27 also reported moderate associations between the PD and IKD for hip abduction and extension RTD; although this study27 compared PD methods with belt-stabilization and tension. These data indicate strong correlations with the PDpull method for specific measures, where the PD was directly compressed against a stationary table (i.e., without a lockout cable used in the previous study27). Nevertheless, direct comparisons with these prior studies26–28 are challenging due to methodological differences, such as variations in testing positions (e.g., supine or standing for hip abduction, fully prone for hip extension).
One unique and notable finding of the current study was that the PDpull method exhibited strong validity for certain hip strength and RTD measures (r=0.70-0.73), while the PDpush method showed moderate validity (r=0.45-0.58), despite no significant differences in discomfort levels on the VAS between the fixation methods (PDpush: 1.7-1.8 cm vs. PDpull: 1.2-1.8 cm). In contrast, a prior report25 examining RTD in knee extension found strong correlations between IKD and both the PDpush (r=0.87) and PDpull (r=0.93) methods, even though the PDpush method reported significantly higher discomfort levels on the VAS (PDpush: 3.1 cm vs. PDpull: 1.1 cm). These findings suggest that discomfort levels may not be a significant factor affecting hip strength and RTD assessments. One potential reason for the relatively lower validity (moderate) of our PDpush method might be the positioning location of the PD. The PD was positioned at a point 5 cm above the lateral femoral condyle or popliteal fossa, which engages regions more abundant in soft tissue and muscle (iliotibial band/vastus lateralis for hip abduction and hamstrings for hip extension), unlike its placement on the more rigid bone (tibia) for knee extension assessment.25 Such placements on bulkier areas during the PDpush method potentially absorb some of the force and/or cause the device to become unstable when generating force momentarily. This speculation may be supported by the strong validity of the PDpull method, as it provides a more stable environment by exerting pressure against a more rigid object. Still, this is all conjecture, and future research is required to investigate whether different PD positioning locations influence force absorption and/or measurement stability and validity across various muscle groups and body regions.
Although moderate-to-high validity was found across all measures, the Bland-Altman plots revealed a tendency towards systematic bias in hip abduction and extension strength and RTD measurements between PD and IKD. These results were expected, as the disagreement between the PD and IKD has often been reported in previous studies.25,29,30,40 Both our PDpush and PDpull methods consistently overestimated hip strength, which aligns with prior data.29,30 Both fixation methods also tended to overestimate most hip RTD measures, except for hip abduction, where the PDpull method underestimated RTD (-0.79 ± 1.32 to -1.30 ± 0.94 Nm/s/kg). Assessing hip RTD using two distinct fixation methods is relatively novel, with limited literature available for direct comparisons.
One possible contributing factor to the underestimation of hip abduction RTD might be the testing position. Unlike the prone position used for hip extension (Figure 2C and 2D), hip abduction was evaluated at 20° in a side-lying position (Figure 2A and 2B), which requires support against gravity. While the IKD offers full support for limb weight during 20° of hip abduction, PD assessments require the assessor to stabilize the limb with pre-tension on the gait belt. The manual stabilization by the assessor may not be as robust as the fixed IKD apparatus. Despite efforts to ensure limb relaxation before trials, the lack of complete support may have led participants to preemptively tense their muscles, especially compromising their ability to generate rapid torque at the beginning of muscle contraction. Since RTD measurements necessitate starting from a relaxed state, testing positions against gravity may not be ideal when using the PD. Future studies may consider the force at the starting point for RTD in their analysis or could utilize electromyography to verify that trials start from a relaxed condition.
Another potential explanation for the underestimation of hip abduction RTD in the PDpull method could be the difference in interface alignment. In the PDpush method for hip abduction (Figure 2A), the PD interface remains parallel to the body, allowing for direct force application, whereas the PDpull method (Figure 2B) introduces a slope between the gait belt and treatment table, altering the angle of direct force application. Future investigations should examine the influences of various testing positions and identify optimal positions for accurate assessment. Nevertheless, the PD can still be deemed a valid tool, given that it evaluates what it purports to measure and demonstrates moderate-to-strong correlations with the criterion standard.
Clinical Implications
In clinical settings, the PD is preferred for its practicality, especially given its ease of use and cost-effectiveness. Given the growing evidence linking RTD deficits to various orthopedic pathologies, such as patellofemoral pain16 and total knee arthroplasty,41 monitoring hip RTD alongside strength in routine clinical practice could be crucial for preventative measures in healthy individuals. The data supports that the PD provides valid measures for both hip strength and RTD from the same time-torque graph during maximal voluntary isometric contraction.28,42 The simultaneous assessment of strength and RTD streamlines the process, eliminating the need for additional resources or time dedicated to evaluating each measure separately, thereby enhancing clinical efficiency. However, it should be acknowledged that coding for RTD calculation may not be common practice in clinical settings. It is recommended to obtain RTD from a torque-time curve graph by manually identifying specific torque and time points (e.g., 0-100 ms).
Based on our findings, it is also recommended that clinicians prioritize using the PDpull method to obtain more valid measures compared to the PDpush method. These findings have practical implications due to the potential reproducibility of evaluation settings, such as acquiring gait belts and treatment tables that would allow for PD testing. The PDpull method may also reduce the need for clinicians to stabilize the device during measurements, which could simplify the assessment process and minimize potential clinician-induced variability. However, it is important to note that the absolute values derived from PD should not be interpreted as equivalent to those obtained from IKD, and vice versa. Clinicians should refrain from interchangeably using the PD and IKD when monitoring assessments across different time points, individuals, or limbs.
Limitations
The sample in this study comprised healthy, physically active individuals aged between 18 and 35 years limiting the applicability to those outside this age range or those with pathological conditions or sedentary lifestyles. The data is limited to findings for hip abduction with a side-lying position with a 20° abduction and hip extension with a standing position with both hip and knee angles at 90°. Future research should explore hip neuromuscular function across various testing positions and joint angles and examine other muscle groups (e.g., hip external and internal rotation) using similar PD configurations. Another limitation is the potential measurement issue caused by not aligning the PD perpendicularly to the body during the pull method for hip abduction (Figure 2B) and by tissue deformation during the push method for hip extension (Figure 2C), both of which may have led to an underestimation of the actual torque. While a standard testing procedure was attempted across all three methods, clinicians should note this potential discrepancy, especially if using a similar setup in clinical practice. Clinicians should recognize that placing the PD on the hamstrings during hip extension testing could dampen the RTD due to tissue deformation before the force is transmitted to the dynamometer. Due to the PD’s 10 N force threshold, participants were instructed to apply a minimum pre-tension before the assessment while maintaining a relaxed state as much as possible. This lack of standardization across participants highlights the need for further studies to explore how the torque level before the trial influences the strength and RTD values. Also, factors including different co-contraction and counteract movement patterns across participants may have influenced the peak torque or RTD generated,43 despite participants receiving the same instructions and undergoing practice trials prior to the measurements. For example, despite the use of stabilization straps, some participants attempted to erect their trunks during hip extension testing, which may be a movement pattern to perform hip extension contractions effectively. Lastly, performing multiple muscle contractions within a single day may have caused fatigue, potentially influencing the results despite the randomization of the testing order.
CONCLUSION
The findings of this study suggest that the PD assessments were valid for evaluating hip abduction and extension strength and RTD in healthy, physically active individuals. The PDpull method demonstrated strong validity for specific measures, including hip abduction RTD0-100_ms and hip extension strength and RTD100-200_ms, whereas the PDpush method showed moderate validity. However, caution is warranted when interpreting the PD measurements, as they may be less suited for absolute strength and RTD assessments due to potential systematic bias compared to IKD.
Conflicts of Interest
The authors report no conflicts of interest.